
Abstract
Background:
Over-nutrition and diet-linked non-communicable morbidities are showing increasing trend overtime. Even if there are different factors that affect the change in BMI other than ART, several authors have reported increases in BMI among PLHIV on treatment that are equal to or surpass the general population. This study is aimed to estimate the prevalence of obesity and overweight among adult HIV infected peoples taking ART in Ethiopia.
Method:
PubMed, CINAHL, Web of science, global health and Google scholar electronic databases were used to perform a systematic literature search. Two authors independently extracted all the necessary data using a structured data extraction format. Data analysis was done using STATA Version 14. The heterogeneity of the studies was assessed by using I2 test. A random-effects model was used to estimate the pooled prevalence. Publication bias was checked using Funnel plot and Egger’s test.
Result:
Two thousand seven hundred and fifty-one studies were reviewed and 13 studies fulfilling the inclusion criteria were included in the meta-analysis. The meta-analysis of 13 studies, comprising 4994 participants resulted in pooled prevalence of overweight to be 17.85% (95% CI: 12.22-23.47). Whereas, the pooled prevalence of overweight was found to be 3.90 (95% CI: 2.31-5.49) but after adjusting for publication bias using trim and fill analysis it has become 3.58 (95% CI: 2.04-5.13). Magnitude of both overweight and obesity was higher in studies conducted in Addis Ababa, studies done after 2016 and studies having sample size of less than 400, in subgroup analysis.
Conclusion:
The magnitude of overweight and obesity among HIV infected peoples taking ART in Ethiopia is high. There is a need to have a routine screening to PLWHA on the risk of over-nutrition in order to facilitate early detection.
Keywords
Introduction
Starting from its emergence, globally approximately 75 million people have been infected by Human Immune Deficiency virus (HIV) epidemic and nearly 43% of those infected have died from illnesses related to acquired immunodeficiency (AIDS). 1 After the discovery and wide spread availability of antiretroviral therapy (ART) in the mid-1990s, human immunodeficiency virus (HIV) related morbidity and mortality has reduced drastically.2,3
Overweight and obesity are becoming a major global public health concern. Over nutrition and diet-linked non-communicable morbidities are showing an increasing trend overtime. 4 Overweight and obesity usually refer to an disproportionate accumulation of fat that will place people at greater risk of impaired health. 5 Chronic and age-related disease prevalence is increasing, since, people taking ART age and live longer with HIV infection.6-8 Less than 25% of deaths among HIV infected peoples taking ART are due to AIDS while up to 50% are secondary to non-communicable causes such as cardiovascular disease (CVD), cancer (other than AIDS related cancer), and renal disease.7,9
Due to the associated wasting, there is a general understanding that people living with HIV (PLHIV) are mostly underweight. Hence HIV infection is referred as the ‘slim disease’.10,11The change in the clinical presentation of HIV/AIDS or the weight gain is believed to be linked with ART regimens as an adverse effect, where as others argue that it is a result of positive immunological response.12,13
Over two thirds of all people living with HIV live in the sub-Saharan African (25.7 million). Of these nearly 18 million people were receiving antiretroviral therapy (ART). In Ethiopia in 2018, 690 000 people were living with HIV. Of all adults aged 15 years and over living with HIV, 66% were on treatment. 14 commonly considered as indicator of clinical treatment success, PLHIV are encouraged to gain weight quickly. Hence, the increase in BMI in adult PLHIV, secondary to treatment has been commended.
Accordingly, even if there are different factors that affect the change in BMI other than ART, several authors have reported increases in BMI among PLHIV on treatment that are equal to or may surpass the general population.15-17 In this meta-analysis we estimated the prevalence of obesity and overweight among adult peoples infected with HIV taking ART in Ethiopia in the last ten years.
Method
Searches
A systematic literature search was performed by using PubMed, Cochrane library, CINAHL and Google scholar. We applied Boolean operator like “AND,” “NOT,” and “OR.” Through consideration of the Boolean operator we searched as follows: ((“obesity”[MeSH Terms] OR obesity[Text Word])) OR (“overweight”[MeSH Terms] OR overweight[Text Word])) OR (“nutritional status”[MeSH Terms] OR nutritional status[Text Word])) OR (“malnutrition”[MeSH Terms] OR malnutrition[Text Word])) OR (“malnutrition”[MeSH Terms] OR undernutrition[Text Word])) AND (“hiv”[MeSH Terms] OR HIV[Text Word])) AND (“antiretroviral therapy, highly active”[MeSH Terms] OR HAART[Text Word])) AND (“ethiopia”[MeSH Terms] OR Ethiopia[Text Word]) (see Table 1 below).
Summary of Search Results for the PubMed, Google Scholar and Other Databases.
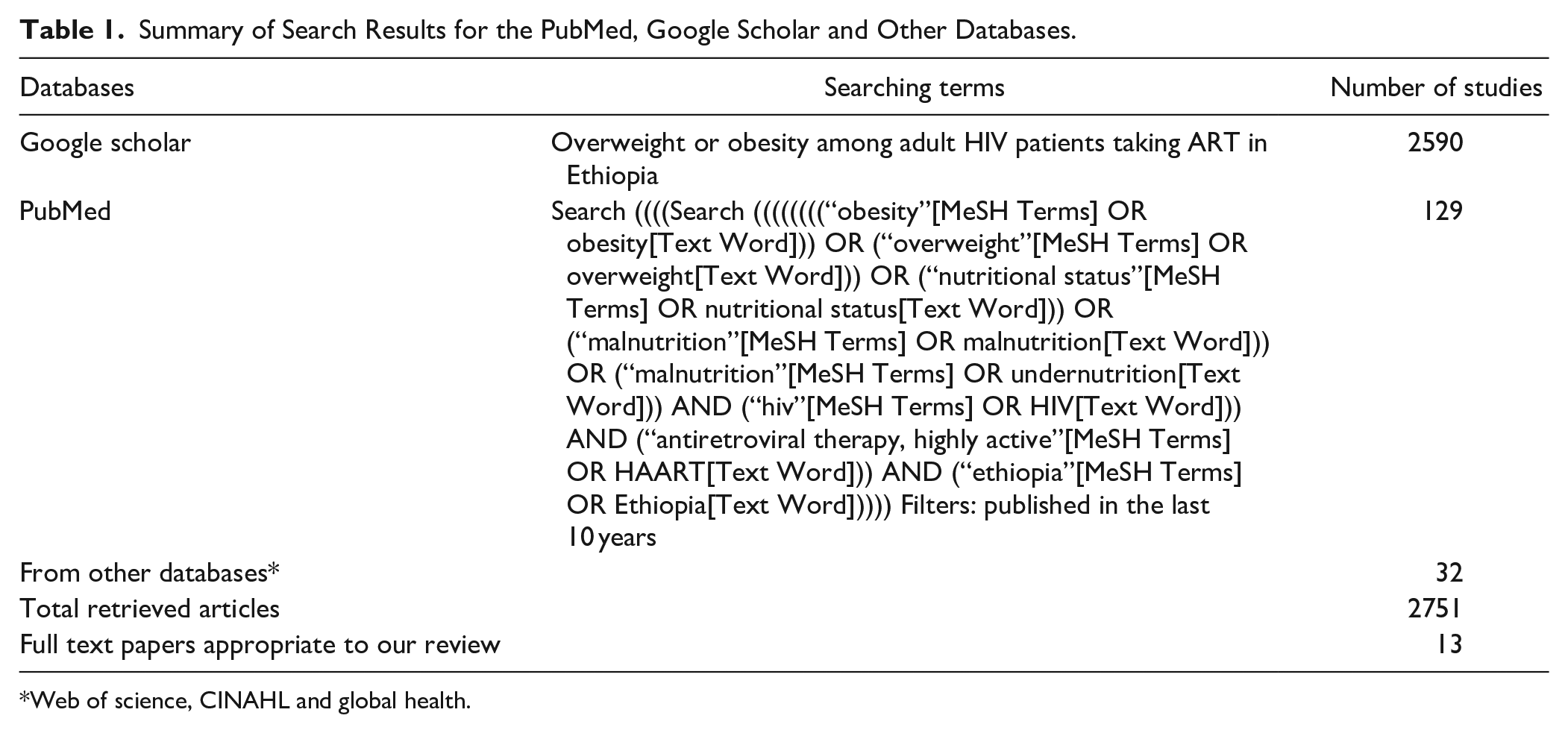
Web of science, CINAHL and global health.
Eligibility Criteria
Based on the mentioned inclusion and exclusion criteria, abstracts were reviewed from search results.
Inclusion Criteria
Study area: studies conducted in Ethiopia only.
Study design: observational studies (cross-sectional, case-control and cohort studies)
Language: studies published/written in the English language only were included
Population: studies conducted among adults.
Publication issue: both published and unpublished articles were searched.
Study period: 2010-2020
Types of Studies Included
Systematic searching of the studies was undertaken from November 15th, 2020 to the 1st of December, 2020 and all results were limited to articles published in English Language from 2010 till December 2020 G.C. Additionally all observational studies (case control, cross sectional and cohort) studies were included. Case reports and case series were excluded from this study.
Initially, availability of full text titles, and abstracts of the articles were assessed. Then the full papers of relevant articles were reviewed. We excluded articles with inaccessible full paper and those published before 2010 from the analysis.
Data Extraction
Two authors (RH and SN) independently extracted all the necessary data using a standardized data extraction format prepared in Microsoft Excel. Disagreements between the authors during data extractions was discussed and reached on consensus. The data extraction format includes first author, publication year, Name of region, number of samples, response rate, and number of event, prevalence with 95% CI.
Outcome Measurement
There are 2 main outcomes in this study. Both the prevalence of overweight and the prevalence of obesity were estimated as the total number of overweight or obese cases divided by the total number of HIV infected peoples participating in the studies multiplied by 100. Overweight and obesity were defined as follows based on the WHO Classification of BMI; overweight if the BMI is 25.0 to 29.9 kg/m2 and obesity if the BMI is ≥30.0 kg/m2. 18
Risk of Bias
Two authors (RH and SN) independently assessed the risk of bias for each article. For assessing the quality of the studies, Newcastle-Ottawa Scale quality assessment tool was used. 19 The tool has indicators consisting of 3 main parts in which, the first part has 5 components and it assesses the methodological quality of each study. The second part of the assessment tool examines the comparability of the studies. The last part of the tool measures the quality of the original articles with respect to their statistical analysis. Using an assessment tool as a guideline, 2 authors independently evaluated the qualities of the original articles. Quality of each study was evaluated using these parameters; those with medium (fulfilling 50% of quality assessment criteria) and high quality (>=6 out of 10 scales) were included for analysis. Disagreements between assessors were solved by taking the mean score of their assessment results.
Data Processing and Analysis
After extraction, the data were imported to STATA Version 14.0 statistical software for analysis. Heterogeneity among reported prevalence was assessed by using I2 test static and its p value. 20 As the test statistic showed, there is significant heterogeneity among the studies (I2 > 95%, P < .0001, for both outcomes) as a result a random effects meta-analysis model was used to estimate the pooled effect. 20 To reduce the random effect variations between the point estimates of the primary studies, a subgroup analysis was done based on study region where the study was conducted and sample size. Egger’s test at 5% significant level was used to assess publication bias. 21 In addition, trim-and- fill analysis was done to assess and adjust for any publication bias. This method is used to first trim the studies that cause publication bias so that the overall effect estimate produced by the remaining studies can be considered least affected by publication bias, and then to fill imputed missing studies in the funnel plot based on the bias-corrected overall estimate. 22 For reporting the finding ‘Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)’ protocol was used.
General Characteristics of Studies
In the first step screening, we got a total number of 2751 papers and 593 papers were excluded due to repetition. According to the titles and abstract 2124 papers were excluded. Thirty-four full text papers were screened for suitability but 21 of them do not report the outcome of interest. After assessing the quality of 13 full text papers. Finally, 13 studies were included (Figure 1).
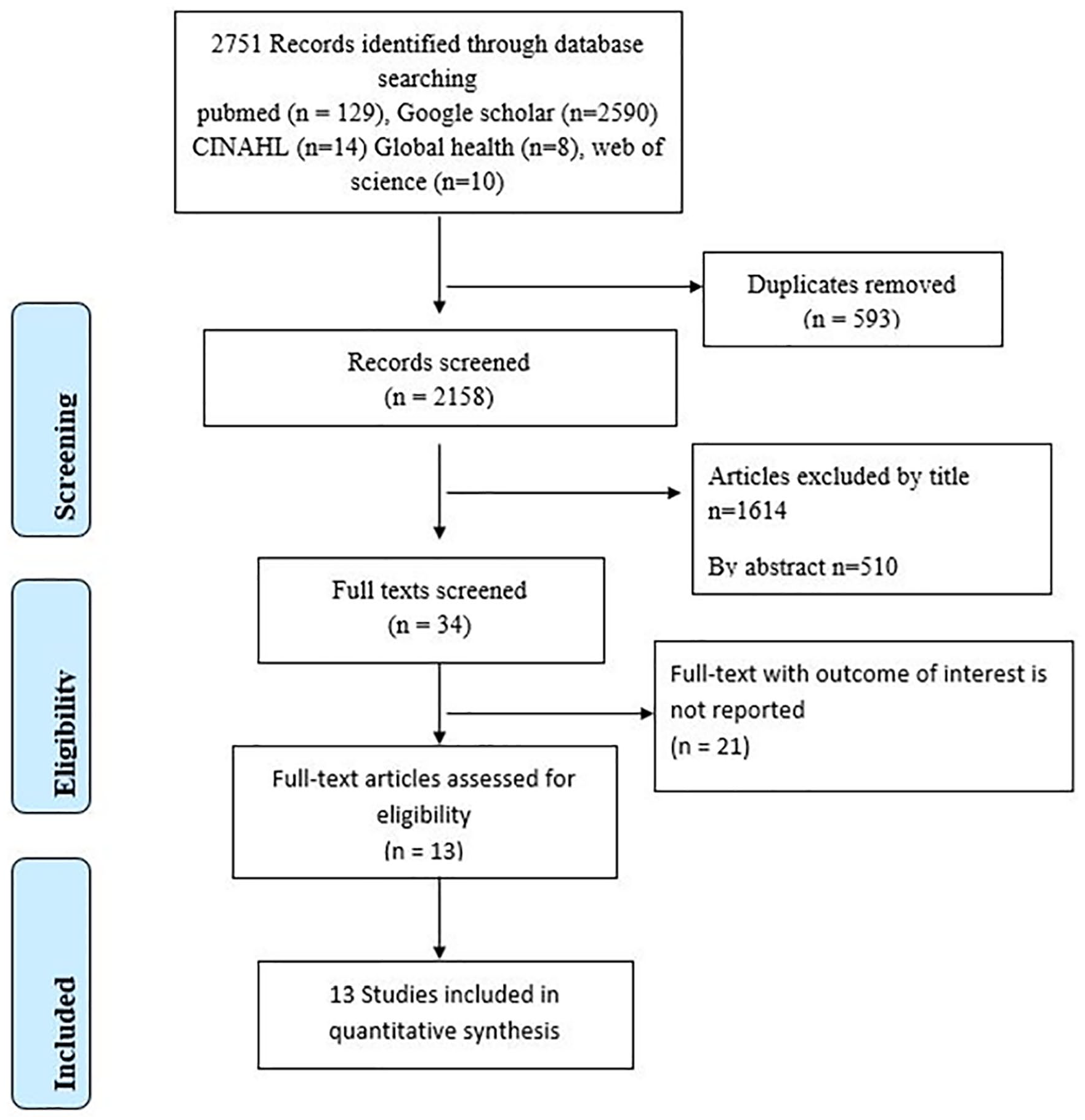
Diagrammatic flow of data extraction process for systematic review and meta-analysis of the Magnitude of Overweight and Obesity among adult HIV patients taking ART in Ethiopia.
Description of Included Studies
A total of thirteen studies, comprising 4994 participants were included in this study. The least number of participants included in a study was 126 and the largest consisted 1097 participants. All the included studies were institution based cross-sectional studies published between 2010 and 2020 (see Table 2 below).
Summary of 13 Studies Included in the Systematic Review and Meta-Analysis of the Magnitude of Overweight and Obesity among Adult HIV Patients Taking ART in Ethiopia.

Risk of Bias
The risk of bias for each original study was assessed by using Newcastle-Ottawa assessment tool which encompassed ten different items. 19 Among the 13 articles included, our summary assessment showed that all (100%) of the included studies had a low risk of bias. (Supplemental Table 1)
Prevalence of Overweight and Obesity
The pooled prevalence of overweight and obesity among HIV infected peoples taking ART in Ethiopia was 17.85% (95% CI: 12.22-23.47) and 3.9% (95% CI: 2.31-5.49). High heterogeneity was observed across the included studies (I2 = 97.1%, P = .000) and (I2 = 93.4%, P = .000) for overweight and obesity respectively. Hence, random effects model was used to calculate the pooled prevalence. See Figure 2 below

Forest plot showing the pooled prevalence of: overweight (A) and obesity (B) among adult HIV infected peoples taking ART in Ethiopia, 2020.
Presence of publication bias was evaluated by using Funnel plot and Egger’s test. The result of funnel plot showed that there was relatively symmetrical distribution for overweight but asymmetrical distribution was seen for obesity across included articles (Figure 3a and b).

Funnel plot with 95% confidence limits for the pooled prevalence of: overweight (A) and obesity (B) among adult HIV infected peoples taking ART in Ethiopia, 2020.
The result of Egger’s test for small-study effects showed that there was no statistically significant publication bias in estimating the prevalence of prevalence of overweight (P = .065) but a statistically significant small study effect was observed for obesity (P = .001). In order to account for the publication bias observed in estimating obesity, we conducted a trim-and-fill analysis. Trim-and-fill analysis imputed on study, and the prevalence of obesity becomes 3.58 (95% CI: 2.04-5.13), a relatively similar finding with previous one but with reduced heterogeneity (I2 = 7.36, P = .000).
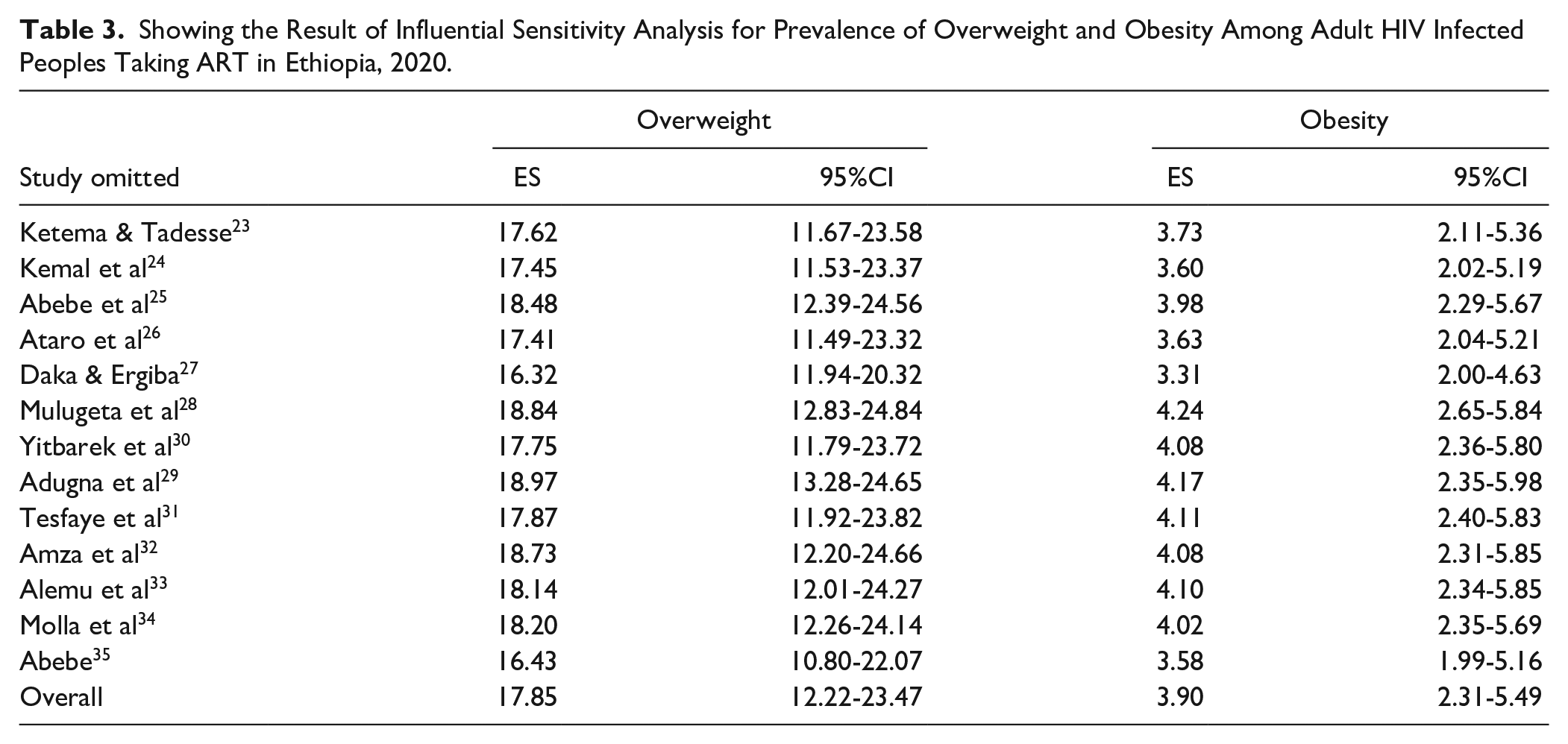
In addition, we conducted influential sensitivity (leave 1 out) analysis to see the effect of individual study on the observed heterogeneity. The results suggest there is no single study that has high contribution for the heterogeneity (see Table 3 below).
Showing the Result of Influential Sensitivity Analysis for Prevalence of Overweight and Obesity Among Adult HIV Infected Peoples Taking ART in Ethiopia, 2020.
The subgroup analysis was done by Region where the studies were conducted, year of publication and their sample size. The higher prevalence of obesity and overweight was observed among studies done after 2016 and studies having a sample size less than 400. (Table 4)
Subgroup Prevalence of Overweight and Obesity Among Adult HIV Infected Peoples Taking ART in Ethiopia, 2020 (n = 13).

Discussion
This systematic review and meta-analysis presents the magnitude of obesity and overweight among adult HIV infected people taking ART in Ethiopia. The magnitude of overweight and obesity ranges from 6.4% 28 to 36.1% 34 and 0.2% 28 to 9.4% 34 respectively.
The finding of this review revealed that the prevalence of overweight and obesity among HIV patients who are taking ART is 17.85 (95% CI: 12.22-23.47) and 3.90 (95% CI: 2.31-5.49) respectively. However, due to the presence of publication bias in estimating obesity, after adjustment with the trim and fill analysis, the estimated prevalence of obesity was changed to 3.58 (95% CI: 2.04-5.13). This finding is higher than reports from Ethiopian demographic health survey of 2011 and 2016, 36 which is done on apparently healthy individuals. The possible reason the discrepancy may be the difference in time, hence globally there is an increase in trend of obesity both among general population and among HIV infected populations.37,38
The finding was comparable to large national level cross sectional study done in Tanzania among adult people living with HIV. 39 Furthermore, the finding was also consistent with the findings of a systematic review and meta-analysis done among general population in Ethiopia that reported the prevalence of obesity to be 5.4% and overweight to be 20.4%. 40 Both developed and developing countries have reported an increasing prevalence of overweight and obese states in HIV-infected persons, consistent with trends in the general population.41-43 Among those who are taking ART, under-nutrition has become less common and there is an increase in weight gain irrespective of ART regimen.13,41,42 This poses a huge troublesome among HIV patients, since even without obesity, individuals living with HIV are at greater risk for non communicable diseases like diabetes and other cardiovascular diseases.44,45
In subgroup analysis, both overweight and obesity was observed to be higher in Addis Ababa and Harar regions of the country. This could be attributed to the relative urban nature of the 2 regions. Similarly, in reports of Ethiopian demographic health survey the prevalence of overweight and obesity was reported to be higher in urban areas. 36 Urban residence is common risk factor for overweight and obesity since people living in urban settings are believed to be at an increased risk of sedentary type lifestyles. 46
In addition, in subgroup analysis, both overweight and obesity were higher among studies having a sample size <400 as compared to their counter parts. Obesity and overweight is higher in studies conducted after 2016 as compared to studies done before 2016, 19.06 versus 13.48 and 4.41 versus 2.29, respectively. This can be explained an increasing trend in the prevalence of overweight and obesity globally and locally.13,39,41
Despite the familiar perception that PLHIV are usually undernourished, 11 there is a shift in nutritional status of HIV patients. Higher prevalence of overweight and obesity in HIV-infected persons have important physiologic consequences that add up to the existing morbidity and mortality. Hence, the results this study imply for the need of nutritional care services for HIV patients in addition to the existing medical care for early to mitigation of the impacts over-nutrition early.
Limitations of the Study
Inclusion of articles written in English only was only among the limitations of this study. This meta-analysis represented study reported from 5 regions of the country only, which may reflect as under-representation.
Conclusion
The magnitude of overweight and obesity among HIV infected peoples taking ART in Ethiopia is high. Due emphasis to people on HAART is needed. There is a need to routine screening to PLWHA on the risk of over-nutrition in order to facilitate early detection. Interventions like life style modification and health education to reduce the burden in this section of the population are also needed.
Supplemental Material
sj-docx-1-jpc-10.1177_2150132721993647 – Supplemental material for Overweight and Obesity Among Adult HIV Infected Peoples Receiving ART in Ethiopia: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-jpc-10.1177_2150132721993647 for Overweight and Obesity Among Adult HIV Infected Peoples Receiving ART in Ethiopia: A Systematic Review and Meta-Analysis by Robel Hussen Kabthymer, Solomon Nega Techane, Temesgen Muche, Helen Ali Ewune, Semagn Mekonnen Abate and Mohammed Feyisso Shaka in Journal of Primary Care & Community Health
Supplemental Material
sj-docx-2-jpc-10.1177_2150132721993647 – Supplemental material for Overweight and Obesity Among Adult HIV Infected Peoples Receiving ART in Ethiopia: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-2-jpc-10.1177_2150132721993647 for Overweight and Obesity Among Adult HIV Infected Peoples Receiving ART in Ethiopia: A Systematic Review and Meta-Analysis by Robel Hussen Kabthymer, Solomon Nega Techane, Temesgen Muche, Helen Ali Ewune, Semagn Mekonnen Abate and Mohammed Feyisso Shaka in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We acknowledge the authors and participants of the included original studies in this systematic review and meta-analysis.
List of Abbreviations
Author Contributions
RK conceived the idea, done data extraction, and analysis. SN had also a role in data extraction. All authors have contributed to the analysis, writing, drafting, and editing. All the authors read and gave final approval for the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of Data and Materials
Data will be available upon reasonable request of the corresponding author.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.