
Abstract
Background
Loyola Medical Center is located in Maywood, IL, a community that faces high rates of poverty, violence, and barriers to healthcare. These factors can contribute to toxic stress, which has been shown to negatively impact children’s health.
Objectives
The goal of this project was to partner with community organizations to obtain a baseline needs assessment from families in Maywood regarding sources of toxic stress and to identify interventions of interest.
Methods
In total, 75 anonymous surveys were collected from the Loyola Outpatient Center Pediatric Clinic and a Maywood community center. Survey responses were statistically analyzed in order to determine toxic stressors most commonly impacting families in Maywood as well as interventions of most interest to the community.
Results
There were 78 respondents for a response rate of approximately 71%. The most common stressors were smoking in the home (33.3%), food insecurity (29.5%), and exposure to violence (26.9%). In this sample, Black respondents were 11.5 times more likely than non-Black respondents to report that their child was exposed to violence in the community – even after controlling for concern about their child’s behavior which served as a surrogate measure of the child’s exposure to toxic stress (P = 0.001). Further, those living with food insecurity were 7.40 times more likely to report that access to food and transportation vouchers were important (P < .001). For every 1-point increase in the total toxic stress score, respondents were 1.35 times more likely to report that increasing access to mental health resources was important to them, though this was not significant (P = .10).
Conclusion
The data demonstrate that toxic stressors, health risks and unmet social needs are prevalent in the Maywood community, which puts local children at risk for future adverse health outcomes. With this information, pediatricians at Loyola Medical Center can work with community organizations to allocate resources to address toxic stressors in Maywood.
Keywords
Introduction
Children are exposed to different stressors throughout their lives that evoke emotional, behavioral, and physical responses. A healthy person physiologically responds to stress with symptoms including increased heart rate and blood pressure as well as cortisol and catecholamine release, preparing the body to confront the stressor. 1 Typically, stressors are temporary and the body readjusts to baseline once the stressor is removed. Toxic stress occurs when a child experiences a chronic source of stress without the necessary caregiver support to blunt its detrimental effects.2,3 Examples of toxic stress are abuse, neglect, and maltreatment, which can all negatively impact a child’s development - sometimes permanently. 4
Chronic stress exposes the developing brain to high cortisol levels, which can alter the child’s neuroendocrine-immune network and suppress the immune system, thus increasing vulnerability to disease.4,5,7 This can permanently change the developing brain and without appropriate intervention can contribute to chronic health conditions such as cardiovascular disease, depression, cancer, and asthma.5-7 The well-known Adverse Child Experience (ACE) study at Kaiser Permanente 7 identified 7 categories of toxic stress: psychological, physical, or sexual abuse; violence against mother; and living with household members who were substance abusers, mentally ill or suicidal, or ever imprisoned. 7 This study found a positive correlation between number of ACE’s and risk for adulthood conditions including heart disease, chronic lung disease, cancer, liver disease, and skeletal fractures. 7 It is crucial to identify sources of toxic stress to prevent chronic health problems in vulnerable children. Primary care physicians can play a crucial role in identifying stressors and exploring interventions.
Promoting healthy futures by preventing these long term health effects requires a multidisciplinary approach including families, community members, educators, and healthcare providers. 8 Pediatricians play a key role in implementing interventions targeting toxic stress as they are at the forefront of topical scientific research and oftentimes have strong lifetime relationships with families alongside a vested interest in children’s health.9,10 While the optimal intervention strategies for pediatricians are still being investigated, existing studies show that an important first step is administering standardized surveys during pediatric visits to assess existing sources of stress among patients.9-12 Incorporating such a survey into natural gaps in clinic flow, such as during waiting or check-in times, would require limited resources and produce minimal strain on practices. Following each assessment, pediatricians can address the patient’s psychosocial needs and connect families to community resources (eg, food access, housing assistance, or alcohol cessation programs). Such intervention requires provider education regarding available community resources and well-developed relationships with community organizations, which are critical for project sustainability. This also asserts the physician’s role in community pediatrics, maximizing the quality of care that patients and their families receive.10,13
This pilot study aims to fill a knowledge gap by assessing the presence of toxic stressors in Maywood, IL via administration of a survey in a local community center and in the pediatric clinic of an academic medical center. Future studies will evaluate the incorporation of the survey results into general pediatric practice and partnerships with local organizations to address the needs indicated in this pilot study.
Methods
A multivariable exact logistic regression model was used to compare the odds of exposure to community violence between respondents identifying as Black versus non-Black while controlling for whether respondents worry about their child’s behavior. Due to the sparse event rate, this was the only covariate considered for the multivariable model. 14 Finally, an ordinal logistic regression model was used to test for an association between food insecurity and the importance of receiving vouchers for food or transportation. The same approach was used to test for an association between the total number of responses pertaining to toxic stressors or unmet social needs and the importance of access to mental health resources. In both models, the proportional odds assumption was assessed using a score statistic as described by Agresti 15 and, due to the small sample size, profile likelihood (rather than Wald) confidence limits were used to report the precision of the odds ratio. 15 All analyses were completed using SAS version 9.4 (Cary, NC).
Results
The response rate for the survey was approximately 71% (n = 78/approximately 110). Among these 78 respondents, most identified as Female (n = 57/76 or 75%) and Black (n = 42/75 or 56%). On average, the respondents were approximately 44 (SD = 17) years old and reported a median of 2 (IQR: 1-3) children under age 18 living in the household. Nearly all respondents reported that they use English as their primary language (n = 76/78 or 97%). See Table 1.
Respondent Characteristics.

Abbreviations: IQR, interquartile range; SD, standard deviation.
Unless otherwise noted, the valid N = 78.
In this sample, there was no association between respondents’ access to reliable transportation and their child’s access to vaccines (P = .40) or healthcare insurance (P = .19), See Table 2. There was also no association between participants’ race and their responses to individual toxic stress items except for the item measuring exposure to violence in the community. For this item, Black respondents were more likely than non-Black respondents to report that their child was exposed to violence in the community—even after controlling for whether they worry about their child’s behavior. However, the effect size for this association is imprecise due to the sparse number of affirmative responses reported in the survey (OR = 11.54, 95% CI: 2.35-113.49; P = .001). See Tables 3 and 4.
Healthcare Access for Those with and without Reliable Transportation.

Valid N = 77. Significance value (P-value) is based on the Fisher exact test.
Toxic Stress Responses for Black and Non-Black Respondents.
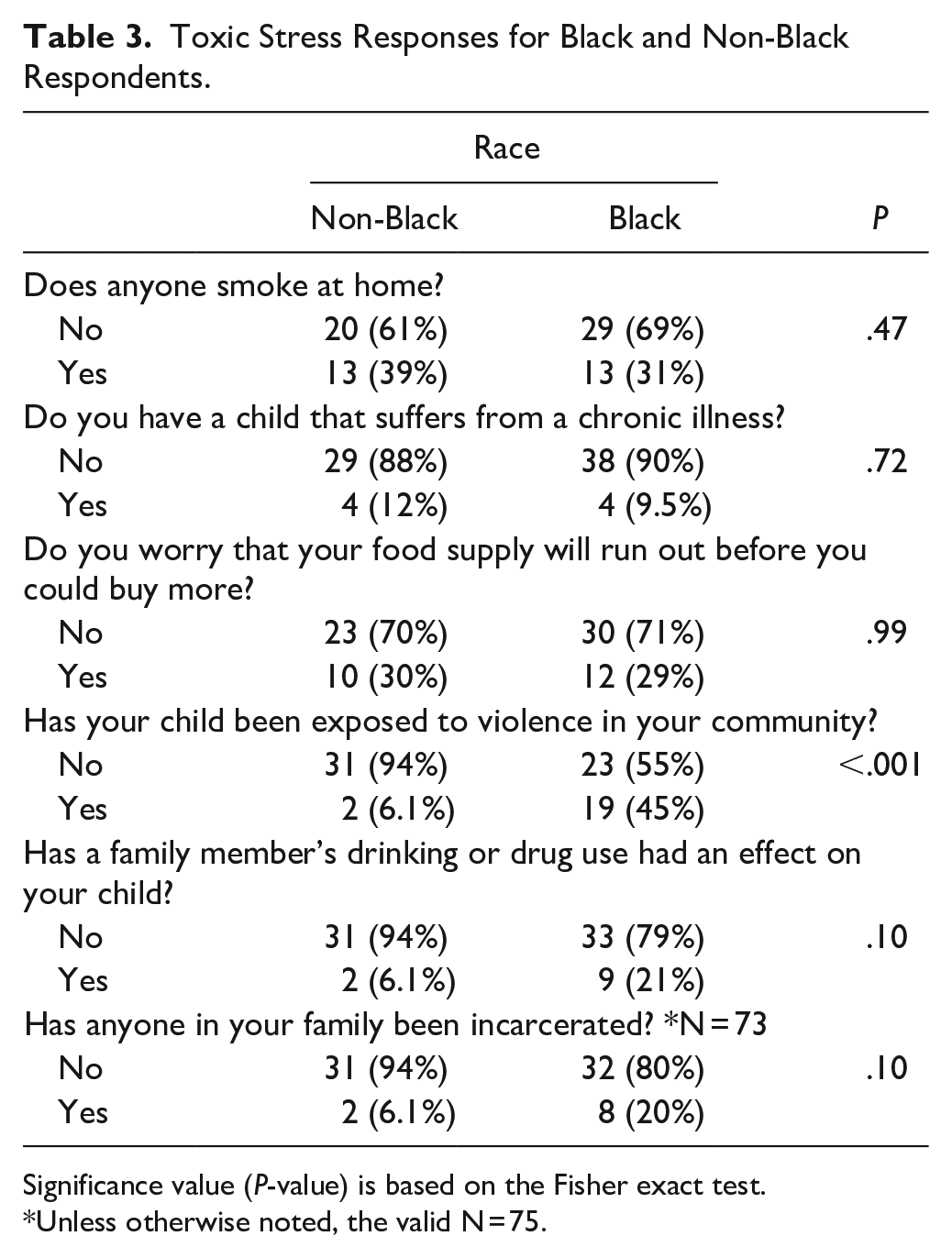
Significance value (P-value) is based on the Fisher exact test.
Unless otherwise noted, the valid N = 75.
Adjusted Odds of Exposure to Community Violence.

Valid N = 75 with 21 (28%) reporting violence in their community. The effect size, confidence limits, and significance value are from an exact binary logistic regression model.
Regarding the importance of vouchers for food and transportation, respondents living with food insecurity were 7.40 (95% CI: 2.49-24.13) times more likely to report that access to food and transportation vouchers were important (P < .001). See Table 5. Similarly, for every 1-point increase in the total toxic stress and unmet social needs score, respondents were 1.35 times more likely to report that access to mental health resources was important—though this result was not statistically significant (95% CI: 0.95-1.93; P = .10). See Figure 1. Figure 1 shows the probability of reporting the priority of mental health resources as a function of the total toxic stress and unmet social needs score. As this score increases, the probability of reporting a low priority for mental health resources declines. Conversely, as this score increases, the probability of reporting that mental health resources are extremely important increases.
Importance of Food or Transportation Vouchers for Those with and without Food Insecurity.

Valid N = 63. Significance value (P-value) is based on the ordinal logistic regression model.

Importance of mental health resources by total number of toxic stress-associated responses.
Discussion
The data demonstrate that toxic stressors, health risks and unmet social needs are prevalent in the Maywood community, which puts local children at risk for future adverse health outcomes. Common health risks and unmet social needs endorsed by Black and non-Black respondents were smoking in the home and food insecurity. Black respondents were more likely to report that their child has been exposed to violence in the community, with this being the most commonly reported toxic stressor for Black respondents. Black respondents were also more likely to report that a family member’s drinking or drug use has had an effect on their child, and that someone in their family has been incarcerated, although there were no statistically significant differences noted. This is similar to previous data that shows that Black children are more likely to be exposed to toxic stressors as compared to their non-Black counterparts. 16
A significantly different result between Black and non-Black respondents was exposure to violence in the community as a function of race and worry about child’s behavior, which acted as a measure of a child’s outcome in regard to toxic stress exposure. It was found that when controlling for worry about child’s behavior, Black respondents were 11 times more likely to report exposure to violence in the community as compared to their non-Black counterparts.
There are many implications of and future directions for this data. First, smoking appears to be highly prevalent in this population. Although this study focused on a pediatric population, this data suggests the necessity for smoking cessation interventions for parents in Maywood. Exposure to second-hand smoke in the home has various negative effects on children including increased frequency and severity of asthma exacerbations, increased frequency of ear infections, increased frequency of respiratory infections, and increased incidence of sudden infant death syndrome (SIDS). 17
Second, food insecurity was noted in about one-third of participants. There was a significant association between those who reported food insecurity and those who ranked food or transportation vouchers as an extremely important resource. This demonstrates a clear opportunity for intervention in the Maywood community. Possible interventions include increasing awareness of established community programs providing food resources to families, expanding capacity to help families apply for public assistance programs in the pediatrician’s office, and partnering with community organizations to develop new programming for residents. Further, Maywood is known to be a food desert with little access to grocery stores offering fresh fruits and vegetables. Therefore, advocacy efforts should focus on increasing access to healthy choices for Maywood residents.
Although not statistically significant, there was a positive association between the number of toxic stress endorsements and reported interest in mental health resources. Studies have shown that integration of mental health resources with regular pediatric care can improve resilience and reduce negative outcomes that toxic stressors provoke for children’s development.18,19
Furthermore, toxic stressors, health risks, and unmet social needs were more often endorsed in families of Black respondents as compared to non-Black respondents, which requires special attention. There is a racial divide in the United States in terms of toxic stress. Studies show that Black families face more sources of such stress, which may contribute to established disparities in health, wealth, and opportunities. Allocation of mental health resources for individuals of all races should be prioritized, with advocacy efforts directed at promoting access regardless of insurance status. Insurance plans frequently offer extremely limited affordable therapy or psychiatry service options, with families often reporting significant wait times as well. 20 This must be addressed in order to promote the health of those exposed to toxic stressors early in life.
Limitations
A number of limitations exist with this study. First, data collection was limited geographically to families with children in Maywood, IL, which does not necessarily represent the entire Loyola patient population. Furthermore, the small sample size (N = 78) could contribute to an unequal representation of the Maywood population. According to 2019 census data, Maywood, IL has a population of approximately 23 158 people, with the distribution of races reported as 68.6% Black/African American, 26.9% Hispanic/Latino, 18.2% White, 0.2% American Indian/Alaska Native, 0.5% Asian, and 2.2% 2 or more races. This can be compared to the survey demographics data (see Table 1), showing that there was a different distribution of race/ethnicity compared to Maywood demographic data (The population of survey respondents was 56% Black, 20% Hispanic, 13% White, and 11% other).
Next, there was a 29% overall non-response rate and a survey question to which over 10% of participants did not respond (See Table 5, importance of food or transportation vouchers for those with and without food insecurity, N = 63). The non-response rate could introduce a non-response bias, excluding individuals at the 2 extremes: those who either do not feel that toxic stress impacts their lives enough to complete a survey and those who are too busy balancing toxic stressors in their lives that they are unable to take the time to complete a survey. Additionally, the incomplete response rate could potentially limit the validity of the data collected from this survey question.
Last, data collected at pediatric clinic visits potentially carries selection bias, as parents of children presenting to clinic visits might report different stressors and healthcare concerns when compared to the general Maywood population. Researchers planned to partner with several community organizations to increase the study’s sample size and gather a more representative data set. Further survey collection was halted in March of 2020 due to the worldwide coronavirus disease 2019 (COVID-19) pandemic, thus limiting sample size. As the pandemic continued, it was decided that any data collected during or after the pandemic could not be analyzed alongside pre-pandemic data, as multiple new challenges may have emerged for respondents, thus altering survey results.
Conclusion
In conclusion, this needs assessment identified multiple ways in which the medical community can partner with the local community to provide useful intervention to alleviate sources of toxic stress and unmet health and social needs among Maywood families. Future recommendations include the following:
Build upon established connections between Loyola and Maywood community organizations and services to facilitate opportunities for equitable resource distribution in the future.
Improve education among Loyola physicians regarding toxic stress and poor health outcomes, as well as sources of toxic stress in the community.
Continue ongoing research and assessment of social determinants of health among Loyola pediatric patients and their families, coupled with resource distribution to address food insecurity as well as financial and transportation difficulties.
Supplemental Material
sj-docx-1-jpc-10.1177_21501327211030136 – Supplemental material for Toxic Stress in a Mid-Sized Urban Community: An Initial Needs Assessment of Families with Children in Maywood, IL
Supplemental material, sj-docx-1-jpc-10.1177_21501327211030136 for Toxic Stress in a Mid-Sized Urban Community: An Initial Needs Assessment of Families with Children in Maywood, IL by Erin McCune, Jennifer Wojtowicz, William Adams, Garry Sigman, Collette Williams, Pauline Ahn, Ashley Ciliberti, Lena Hatchett and Julie O’Keefe in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to acknowledge and thank Ragini Bhadula, MD, who initially conceived of this project and the application for the AAP CATCH grant. Without her efforts, it is unlikely that the project would ever have been initiated.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.