
Abstract
Purpose
Thailands’ informal workers are faced with job insecurity and poor working conditions. Good health status can promote lifelong working and increase quality of life. This study analyzed factors associated with the health status of the community informal workers.
Methods
A cross-sectional study was conducted with 390 informal workers aged 15 to 59 years in Thasala district, Nakhon Si Thammarat, southern Thailand. A multi-stage sampling method using proportional to size selection was employed in various types of informal workers. The interviews on self-reported health status, health behaviors, occupational hazards, healthcare utilization, occupational health and safety (OHS) access are reported as descriptive. The multivariate association was explored using the simple logistic regression.
Findings
The results revealed that 80.77% of the participants had good health, 57.44% had healthy behavior, 76.41% had safe work practices, 22.05% had moderate to high exposed of occupational hazards, and 56.41% had the low OHS access. Safe work practices, moderate to high OHS access, low exposed to occupational hazards, and low income were more likely to produce good health status, which yielded the adj. OR 2.57, 1.86, 0.39, and 0.48, respectively.
Conclusions
The community informal workers health status was associated by income, work practices, occupational hazards, and OHS access. To strengthening the informal workers’ health, the OHS program should be managed intensively by the primary care services, especially the OHS risk management.
Introduction
The report of the International Labour Organization (ILO), 2019 shows that the global working-age population was 5.7 billion. Out of these, 3.3 billion people (57%) were in employment, whilst most of them (61%) was in the informal sector. 1 In the same year, Thailand had a total of 37.5 million employed people, of which 20.4 million (54.3%) were informal workers. 2 Most of them work in agriculture (56.4%) followed by the service and trade sectors (33.1%) and the manufacturing sector (10.5%), 2 which is similar to other low and middle income countries for which agriculture is the highest sector for informal employment.1,3 The informal workers are largely excluded from any protections provided by national labor laws and regulations. They are still faced with the need for fair compensation from the government 52.8%, hard work 17.1%, and not receiving continuous employment 16.6%. The rest is a matter of no welfare, no working days, and regular hours. Nevertheless, job insecurity and poor working conditions often leave informal workers particularly vulnerable to catastrophic health crises.4,5 The workers’ health affects national productivity, increasing the nations’ economic value and reducing healthcare costs. 5 Legally, informal workers do not have the right to receive benefits equivalent to formal workers.6,7 As a result, rural informal workers, such as agriculture and self-employed workers, cannot access adequate occupational health and safety (OHS) measures as required by law and the social security program.
There were 2 973 633 informal workers in the southern region of Thailand in 2016. Nakhon Si Thammarat province had the most at 18.9%, which amounted to 65.4% of the total labor force. Most were worked at the rural area and engaged in agriculture and fishery (58.4%), followed by general service (19.5%), and skilled work (10.6%), respectively. 8 The rate of injury or illness due to employment increased by 6.9% compared to 2015. Most illness causes were due to unsafe work practices and environments, exposure to chemical hazards, low compensation, and discontinuous work. Health risks in the workplace were heat, noise, dust, chemical, biological or ergonomic hazards, unsafe machines, and psychological stress, caused work-related diseases and aggravated other health problems.
Moreover, the inability to access OHS services significantly influences workers’ health, including health-related behaviors and noncommunicable diseases (NCDs). 9 Therefore, the OHS services for the community informal workers are needed and should be explicitly implemented and systematically. This action will increase social and health protection because the informal workers are considered a lack benefits, insurance and other benefits coverage of employment.10,11
In Thailand, the informal workers could access to health care services by the Universal Health Coverage Scheme (UCS), which covers health insurance of medical care, health promotion and disease prevention in the community health care.2,12,13 The principle of community health services were based on primary care practice but not specific to the OHS services. The sub-district health promoting hospital and community hospital in the district primary care network integrated the OHSs’ action by health promotion and prevention practices. However, little study reported the association of health status, work environments, and community OHS accessibility of the informal workers in rural of Thailand. This study health status and the association of its determinants and the OHS accessibility among informal workers in Thai rural community. The study benefit was to enable community health care organization to promote the OHS action following the fundamental rights of workers as well as health promotion, disease prevention, and protection for the informal workers to have the better long-term working ability.
Methods
Study Design and Setting
This cross-sectional study was conducted in the Thasala district, a rural site located in Nakhon Si Thammarat province, southern Thailand. The informal population in 2017 was 118 229. The informal workers were in rubber and fruit plantations (60%), rice farms (25%), coastal fisheries (7.2%), livestock (5%), and grocery (2.8%). The health care system in Thasala included the district hospital, and 16 sub-district community health promoting hospitals. The community health services had at least 1 professional nurses, 1 or more public health practitioners, 10 or more village health volunteers, and insurance coverage.
Sample Size and Sampling
Participants in the study were Thai informal workers aged 15 to 59 years. In 2017, the study population was 23 353 (Community development office of Thasala district, 2016), of those were calculated sample size by the finite population proportion formula 14 with p 0.64, 15 z 1.96, e 0.05 and adjusted extra 10% then yielded the minimum sample size of 390. Community areas and types of occupation were employed by multi-stage sampling with proportional to size selection. The district was divided into clusters by using 10 sub-districts and 6 occupations followed by a simple random sampling technique from the informal worker database.
Materials and Data Collection
The community survey were operated by questionnaire, which comprised of 4 parts. Part 1 composed of sociodemographic characteristics (gender, age, education, occupation, income per month; the median of income set cut of point 8000 Thai baht), and health history. Part 2 was for total health status assessment by the Short-Form Survey Version 2.0 (Thai version) 16 ; 36 questions with 2 main components of the physical and mental health. Part 3 composed of health behavior, working practices and occupational hazards exposure; food consumption, exercise, recreation, substances abuse, and housing sanitation, compliance with OHS and work environment, hazards exposure; physical hazards (hot environment, insufficient light, glare, noise), chemical hazards (pesticide, gas or vapors, dust), biological hazards (poisonous animal, mold), biomechanical hazards (awkward posture, lifting or moving heavy object, and repetitive work motion), and psychosocial hazards (unstable income, fast work pace, work overload, and work-related stress). Part 4 was for the health promotion and UCS utilization in community health services; general health education, primary care services and disease prevention, OHS access (accessibility and availability to the community OHS services during the last 12 months, cholinesterase screening, job analysis and work processes risk assessment, occupational diseases, and injuries primary diagnosis and prevention).
The questionnaires’ content validity was checked by 5 experts, which yielded the index of item objective congruence (IOC) 0.8 to 1.0. The researchers collected data during August-September 2017.
Statistical Method
Both descriptive and inferential statistics were carried out using R 3.2.1 for Windows. 17 The access to care and utilization score were categorized into 3 levels according to the class interval calculation as “low,” “moderate,” or “high” classes. These variables were dichotomized by combining the categories “moderate,” “high” to indicate “moderate to high,” “low” stilled the same. Pearson’s Chi-squared and Fisher’s exact tests were used to compare the rates of health status for crude association. The potential variables were selected with P-value less than or equal to .20 from bivariate analysis to perform the final model. Simple logistic regression modeling was performed to detect multivariate associations. A significance level of .05 was defined.
Approval and Consent Participate
The study protocol was approved by the Scientific and Ethical Committee in Human Research, Walailak University, No. WUEC-16-049-01. Written informed consent was obtained from all participant at the beginning of the study.
Results
Out of the 390 samples 207 were females with ages ranging from 18 to 59 years (mean age 42.7, SD 9.34 data did not show in Table), most of them were Buddhist (84.1%), and married (89.23%). The informal workers who had monthly income less than or equal to 8000 Thai baht were 67.95%, however 54.36% could balance their expenses. The health status showed that most of the informal workers were good health (80.77%) and educated by primary school (53.59%), the most common diseases were hypertension (8.97%), followed by dyslipidemia (6.41%). Most of the informal workers in southern Thailand are self-employed agricultural worker, such as rubber and fruit, and oil palm or coconut plantation. Some workers worked more than 1 type of crop. The highest proportion of workers were in rubber plantations (57.95%), followed by fruit plantations (22.05%). The average current year of working duration was 15.73 years (S.D. = 9.76). All of the informal worker utilized healthcare services by the UCS in community. Of them, 70.5% indicated “moderate to high,” while 29.5% indicated “low” utilization.
Most of the study sample were healthy behaviors corresponded to safe work practices, 57.44% and 76.41%, respectively. Of those, 63.85% were exposed to heat, and 80.51% were exposed to poisonous animals. Awkward posture and lifting or moving heavy object were the top 2 hazards exposure which were 96.67% and 91.54%, respectively. They also worked with sharp machine/tools at 81.03% followed by working in wet areas 44.10%. It was noted that unstable income was the greatest risk (92.82%) of psychological hazards. (Table 1)
General Characteristics, Behaviors and Working Environments of Informal Workers (n = 390).
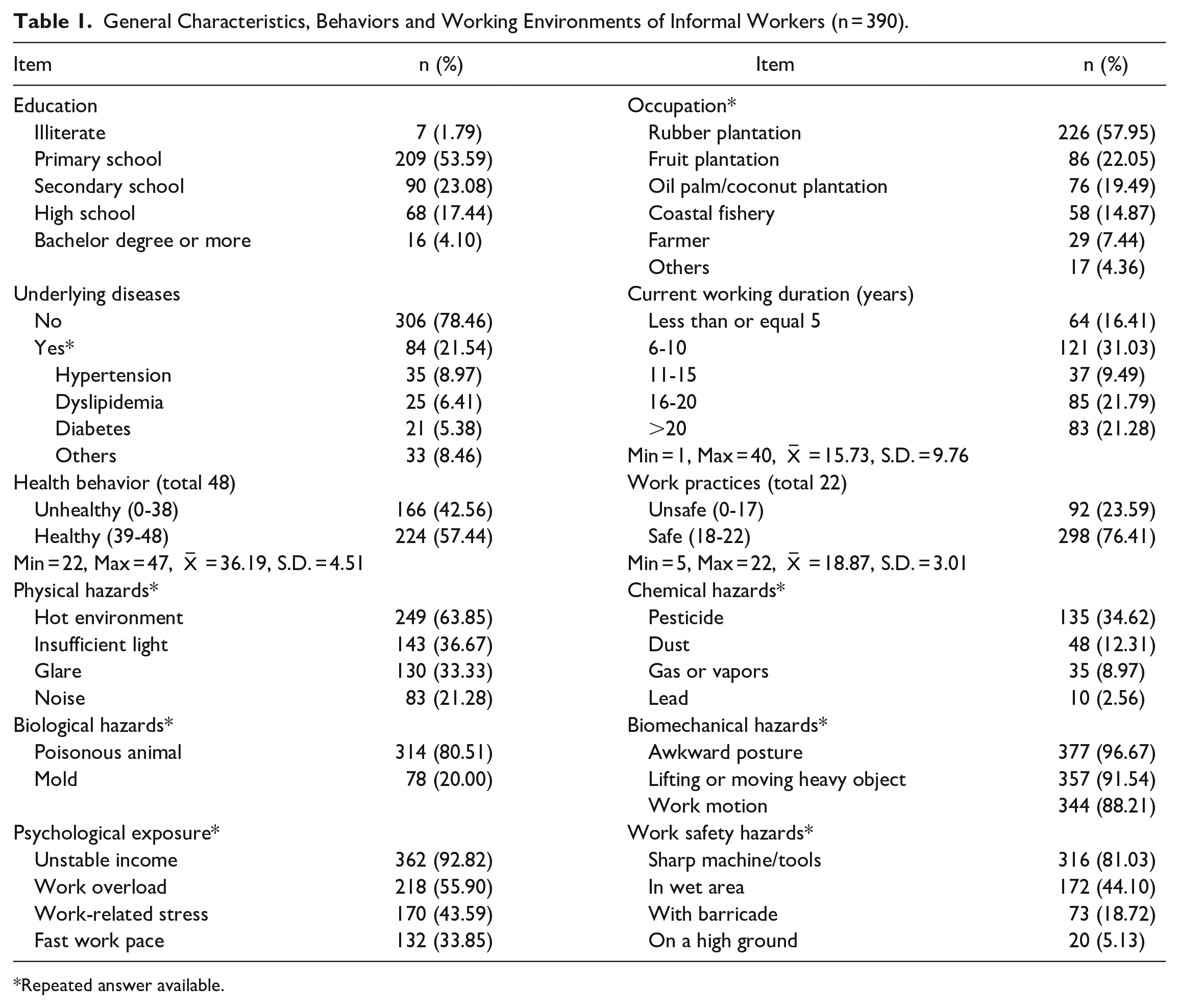
Repeated answer available.
Table 2 demonstrated the association of health status and its determinants. The significant associations were found in income, work practices, occupational hazards exposure, and OHS access (P < .05, χ2 test). The highest proportion of good health were found in the low income (57.95%) and safe work practices (64.87%). Aside from occupational hazards exposure, the workers who worked in the low exposed group had good health status (65.38%) more than the moderate and high exposed group. The analysis also showed that the low OHS accessed informal worker group had good health status (43.33%).
The Crude Association of Health Status and Sociodemographic Characteristics, Health Behavior, Work Environments and Health Care Access Among Community Informal Workers (n = 390).

Chi-square test.
1 USD equals to 31.20 Thai Baht.
Fisher’s exact test.
Universal health coverage scheme.
Occupational health and safety.
P < .05.
Table 3 reports odds ratios and 95% confidence interval from the binary logistic regression analyses of association among health status and the potential determinants from crude association analysis adjusted by age and gender. The statistically significant factors associated with health status were income (adj. OR: 0.48, 95% CI: 0.25, 0.93), work practices (adj. OR: 2.57, 95% CI: 1.47, 4.49), occupational hazards exposure (adj. OR: 0.39, 95% CI: 0.22, 0.70), and OHS access (adj. OR: 1.86, 95% CI: 1.07, 3.25).
The Associations of Income, Work Practices, Occupational Hazards, OHS Access and Health Status Among Community Informal Workers (n = 390).

Abbreviations: CI, confidence interval; OR, odds ratio.
Discussion
Most of the community informal workers in southern Thailand were females in the agriculture sector and educated at primary school. This is in line with the findings from a previous study that showed informal workers often have low education.1,18,19 The study by Rios and Nery 5 stated that low education reinforces the hypothesis that many workers in the informal sector may lacked the necessary skills to obtain healthy working skills and protection. Thailands’ the ninth national plan 20 promoted education, health, skills and a social welfare system, as well as the development of labor and the OHS standards in line with international standards for informal wokers. 21 Therefore, the OHS access by the community health care sector was the important measure for the equity in the health care protection of those workers.22,23
This studys’ main finding revealed that multiple factors associated with informal workers’ health status are income, work practices, occupational hazards exposure, and the OHS access. Most of participants are adult workers, and have good health status. However, gender and age group are not associated with health status. The previous study of informal employment and health status in Central America indicated that poor self-perceived and mental health status depended on no social security coverage and there was no difference in both gender. 24 Therefore, the access to social security is the important determinant of health status among informal workers. In our study, the low-income workers had their health status better than the high-income group (adj. OR 0.48). Most of them are adult worker, good health and income less than 8000 Thai baht. Obviously, the healthy worker effect was found among the adult workers, although they had less income. In addition, the total health status was measured by both physical and mental health. The participants 54.36% reported they could balance their living expenses, although a large proportion of unstable income. The findings then supported that informal workers in rural community had a good health, although they had less income. In addition, the UCS provided by the government in community health services covered all informal workers in Thailand. Therefore, there was no economic barrier to access health services in the low-income group to access health care services according to health need. In Thailand, almost all people received medical treatment from primary health care systems under the Thai UCS. 12 The UCS mechanism focused on health promotion and disease prevention by the community health volunteers services through community hospitals. The 1997 and 2007 Thai constitutions asserted that every Thai citizen has a right to health care and that it should be free for the poor, including informal workers.25,26 Many studies of illness expenditures in Thailand have confirmed that the UCS system substantially reduced the financial burden of health care among low-income and poor people. 26 Therefore, the informal workers may be satisfied with the health care services that affected their health status report in the study.
The second findings were safe work practices and low hazards exposure had a positive association to good health status. The result indicated that 76.41% of informal workers reported that they had safe work practices. Those encouraged all informal workers, including self-employed persons, to take care of their workplaces to promote safety and health at work to meet applicable standards. In the past 20 years, there has been the first training program for occupational health and safety programs for informal workers groups known as Work Improvement in Neighborhood Development (WIND) in Thailand.27-29 WIND was an effective tool to use when promoting health and safety for the informal sectors. It encouraged the workers to improve the quality of their own lives and workplaces voluntarily. Most of the workplaces of community informal workers resided in their home or nearby. However, those program are still not integrated in community health routine services. Our finding will then support the program benefit that the safety practices and environments can significantly promote informal workers’ health. The last finding showed that the moderate to high access OHS was associated positively with a good health status (adj. OR 1.86). The finding confirmed that the sufficiency OHS services were a crucial factor for good health status. Our result differed from the study of Akazili et al, 30 which reported that informal workers who were mainly in the poor group in Ghana could not access health care because of the economic barrier.24,31 The integrated OHS services with health promotion activities by the Thai UCS services can be promoted accessibility and coverage. However, more than half of the respondents reported insufficient OHS services specific to occupational health risks management. This finding reflected the awareness and demand of work-related health care of the workers that required participatory measures in action by the community health services sector.32,33
Conclusions and Recommendations
The informal workers in rural communities, southern Thailand, face unstable income and various occupational hazards. The health status was associated with income, work practices, occupational hazards exposure, and the OHS access. Thailand UCS services played a vital role to operate health prevention and promotion for the informal workers in rural communities. The OHS access is explicitly associated with the informal workers’ good health status, mostly in low-income groups. Thus, to strengthening the informal workers’ health, the OHS program should be managed intensively by the primary care services, especially the OHS risk management and program in the agriculture segment. The community OHS programs’ development should be integrated with the UCS services and the local administrative management for social welfare protection. Those model development should have consisted of (1) capacity building of health personnel in occupational health risk analysis; (2) emphasizing occupational health intervention specific to health risk exposure; (3) monitoring and controlling the program by networking for learning and supports.
Footnotes
Acknowledgements
The authors are grateful thank to health personnel and community group members at Thasala Nakhon Si Thammarat province who participated in the study. They also would like to thank Walailak University for facilities and supports.
Author Contributions
ST, CT, and SK were responsible for the concept, development, interview conduct, and supervision of the research. SK collected community data and analyzed data. ST and CT analyzed the data and constructed the manuscript. All authors contributed to the preparation of the manuscript, reviewing and approving the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study has been approved by the Human Research Ethics Committee of Walailak University, Thailand (No. WUEC-16-049-01). Written Informed consent was obtained from all participants at the beginning of the study. The participants were reminded that the study was voluntary, confidential and the results would remain anonymous.