
Abstract
Background
Family Medicine was introduced as a major undergraduate clinical rotation in 2016 after the medical college at Imam Abdulrahman Bin Faisal University revised its curriculum.
Objective
Assessing how students’ medical knowledge has improved post Family Medicine introduction to the revised medical school curriculum.
Study Design
This was a cross-sectional epidemiological study among fifth year clinical medical students (n = 219). A pretest and post-test was distributed to all fifth year clinical medical students voluntarily during the period of October 2017 to May 2018. They were asked to rate the exam as well.
Results
The mean exam grades were 25.52 (SD = 4.44) and 34.16 (SD = 5.76) for pre-rotation and post-rotation, respectively. There was a statistically significant difference between post and pre rotation exam grade for the overall sample (t (218) = 23.73, P < .0001) indicating that students had a statistically significantly higher exam grades post-rotation (M = 34.16, SD = 5.76) than pre-rotation (M = 25.52, SD = 4.44). Females had a statistically significantly larger difference in post-rotation and pre-rotation exam grade than males indicating that they improved more in the post rotation exam. It was found that nearly 60% (59.36%) of subjects considered the exam difficult before the rotation; however, only around 40% (40.18%) considered the exam difficult after the rotation.
Conclusion
Students benefited after taking the course of family medicine. This helps in advocating for both the importance of this specialty and for the university’s decision in incorporating family medicine as a major clinical rotation for undergraduates.
Introduction
Although more and more medical students are enrolled in family medicine training programs each year, the overall recruitment in this crucial medical specialty still proves to be challenging.1,2 The demand is much higher than the supply as medical care is moving toward generalization as opposed to super-specialization. 3 The situation is of no difference here in the Kingdom of Saudi Arabia as all efforts are made to draw fresh medical graduates toward the specialty of family medicine in concordance with the 2030 Saudi vision. 4
In Imam Abdulrahman Bin Faisal University (IAU), the world trend was followed 5 as family medicine was introduced as a major undergraduate rotation in fifth year in 2016. All undergraduate medical students who pass the first 3 pre-clinical years of medical school go through major clinical rotations in their clinical years, year 4, 5, and 6.
The family medicine rotation in fifth year is held 4 times throughout the year. Two batches of all male and all female students per semester attend clinics, lectures, tutorials, and skill labs for 8 consecutive weeks that end in an end of rotation multiple choice questions (MCQ) exam. In order to pass the rotation, Students attend an end of semester objective structured clinical examination (OSCE) composing 10 clinical stations. 6
Family medicine academic staff from university demonstrators to professors collaborate in the teaching of the family medicine undergraduate module. The academic staff and the hospital appointed staff are an integral part of the student educational environment. 7 No efforts are spared to enrich the students’ experience and positively influence their medical education. 8
In this current study we aimed at assessing students’ knowledge prior to and post family medicine rotation and how participants’ medical knowledge developed after taking the family medicine rotation after the university revised its curriculum in 2016 by adding family medicine as a major clinical rotation. 6 We aimed at assessing gender and batch ranking differences in medical knowledge achievement and perception of exam difficultly throughout the whole year. To our limited knowledge and up to this current time, no studies were performed in the region to address the same objectives.
Materials and Methods
This cross-sectional epidemiological study was conducted during the period of October 2017 to May 2018 among fifth year clinical medical students that were due to start the family medicine clinical rotation clerkship. The total number of students in the fifth-year clerkship was 246 students, after excluding students who have not attended the orientation or who have not completed their exams, we ended up with 219 students included in the study. These students were divided into 4 batches, 2 per semester. In the first semester, the first batch was all male students (n = 53) then the second batch were all female students (n = 58). The second semester started in the opposite way, as female students were in the third batch (n = 58) and lastly, our fourth batch constituted of all male students (n = 50).
When 1 batch attended a clinical rotation, other batches had other major clinical rotations to attend as well so that by the end of the year, each student would have attended 4 major clinical rotations. These are: Family Medicine, Mental Health, Obstetrics and Gynecology, and Pediatrics. This deems the first batch that started family medicine in the year a fresh batch that has not passed by any clinical rotation before and the last batch to take family medicine in fifth year a batch that is more experienced with more exposure as they have taken all other 3 majors before joining the family medicine rotation.
In the first day of the rotation, students were greeted and introduced to the course and the course objectives were explained. They were given all important related information that were prepared by the authors as well, about material covered, clinics, portfolios and the assessment methods. At the end of the day, a pretest constituting of 50 single best answer multiple choice questions (MCQs) was distributed to all students who attended, and they were asked to answer it. Students were clearly told that this was voluntary to test their knowledge prior to the course and it will not be graded or added in their final rotational grade. It was treated as a mock exam as no open books or questions were allowed. The time allowed for the exam was 45 minutes. All copies distributed were recollected making sure that students filled in their names and ID numbers. Students were assured that all personal data will remain confidential and will be used for research purposes only. All the multiple-choice questions included in the exam were about basic family medicine pertinent medical information that would be later coved in the rotation itself. Each MCQ had a short vignette with 4 possible answers in a simple and direct English language that students are used to following the standard MCQ writing procedure to avoid any vagueness. 9 Ethical approval to conduct this project was granted from the faculty of medicine student council and the vice deanship of academic affairs at Imam Abdulrahman Bin Faisal University administration.
Students were asked to rate their exam at the end by either easy, fair, or difficult. The same process was repeated in the last week of the rotation after completing all the required training and before entering the end of rotation examination. The same exam was distributed to the batch as a post rotation test and they were asked to rate it again. Each exam was corrected with scores ranging from 0 to 50 (highest). And exam rating was 3 levels. (1 = easy, 2 = fair, and 3 = difficult).
Statistical Analysis
Data were imported into and analyzed using SAS version 9.4 for Windows (SAS Inc., Cary, NC). Data were examined for missing values. Only subjects with complete data were retained in the analysis. Normality of the data (pre-rotation grade, post-rotation grade, and difference between post and pre rotation exam grade) was examined though z-scores of skewness and kurtosis. 10 Paired t-test was performed to determine if there was a statistically significant difference between pre-rotation exam grades and post-rotation exam grades for the overall sample, for each gender, and for each rotation group.
Two-sample t-tests and 1-way analysis of variances (ANOVA) were conducted to determine if there was a statistically significant difference in exam grades between males and females (2-sample t-tests) and among the 4 rotation groups (ANOVAs). Chi-square tests of independence were conducted to determine if there was an association between exam rating and, gender and rotation group, before and after rotation. Bowker’s tests of symmetry were used to determine if there was a difference between pre exam rating and post exam rating.
As exam grades and exam ratings were measured before and after rotations, observations from the same subject were related, and hence repeated measures analyses were conducted to determine the relationships between exam grade, exam rating, gender, and rotation group.
Two linear mixed-effects models were conducted to investigate if there was a relationship between exam grade, and gender, rotation group, and exam rating. For both models, interaction effects of time (pre, post) and the other 2 predictors were included in the model in order to examine if the effects of the predictors depended on time. The unstructured covariance matrix was employed to model the correlation between the 2 observations from the same subject. No random effects were included in the models. Both logistic regression models modeled the probability of viewing the exam as difficult (ie, the higher category of the ratings). Odds ratios (OR) and the 95% confidence intervals (CI) were computed to quantify the results of pairwise comparisons and determine the strength of association between the outcome variables and the predictors for any factors with more than 2 levels (eg, rotation group), if the effect was significant, pairwise comparison was performed to see at which 2 levels the statistical significance occurred. For any tests, a P-value less than .05 indicated significance. All P-values were 2-sided.
Results
The data of 246 subjects were collected. Subjects with incomplete data for exam grades and exam ratings (data for pre and post rotation) were excluded from the data analysis. The final sample size for the study was 219. Among the 219 subjects, slightly over half of them were female (n = 116, 52.97%) and the rest were male students (n = 103, 47.03%). There were around 50 subjects in each rotation group (n = 53 (all male) for group 1, n = 58 (all female) for group 2, n = 58 (all female) for group 3, and n = 50 (all male) for group 4.
Table 1 shows the descriptive statistics of exam grades (pre-rotation grade, post-rotation grade, and difference between post and pre rotation exam grade (post-pre)). The z-scores of skewness and kurtosis for the data were within ±2.58, indicating the data were normally distributed. The mean exam grades were 25.52 (SD = 4.44) and 34.16 (SD = 5.76) for pre-rotation and post-rotation, respectively. The average difference between post and pre rotation exam grade was 6.84 (SD = 5.39). The results of the paired t-test indicated that there was a statistically significant difference between post and pre rotation exam grade for the overall sample (t (218) = 23.73, P < .0001) indicating that students had a statistically significantly higher exam grades post-rotation (M = 34.16, SD = 5.76) than pre-rotation (M = 25.52, SD = 4.44). Figure 1 shows box plots of exam grades (pre-rotation grade, post-rotation grade, and difference between post and pre rotation exam grade (post-pre)
Descriptive Statistics of Exam Grades (Pre-Rotation Grade, Post-Rotation Grade, and Difference between Post and Pre Rotation Exam Grade (Post-Pre)).

n = 219.
Abbreviations: Q1, lower quartile (the first quartile); Q3, upper quartile (the third quartile); SD, standard deviation; SE, standard error; Zskewness, z-score of skewness; Zkurtosis, z-score of kurtosis.
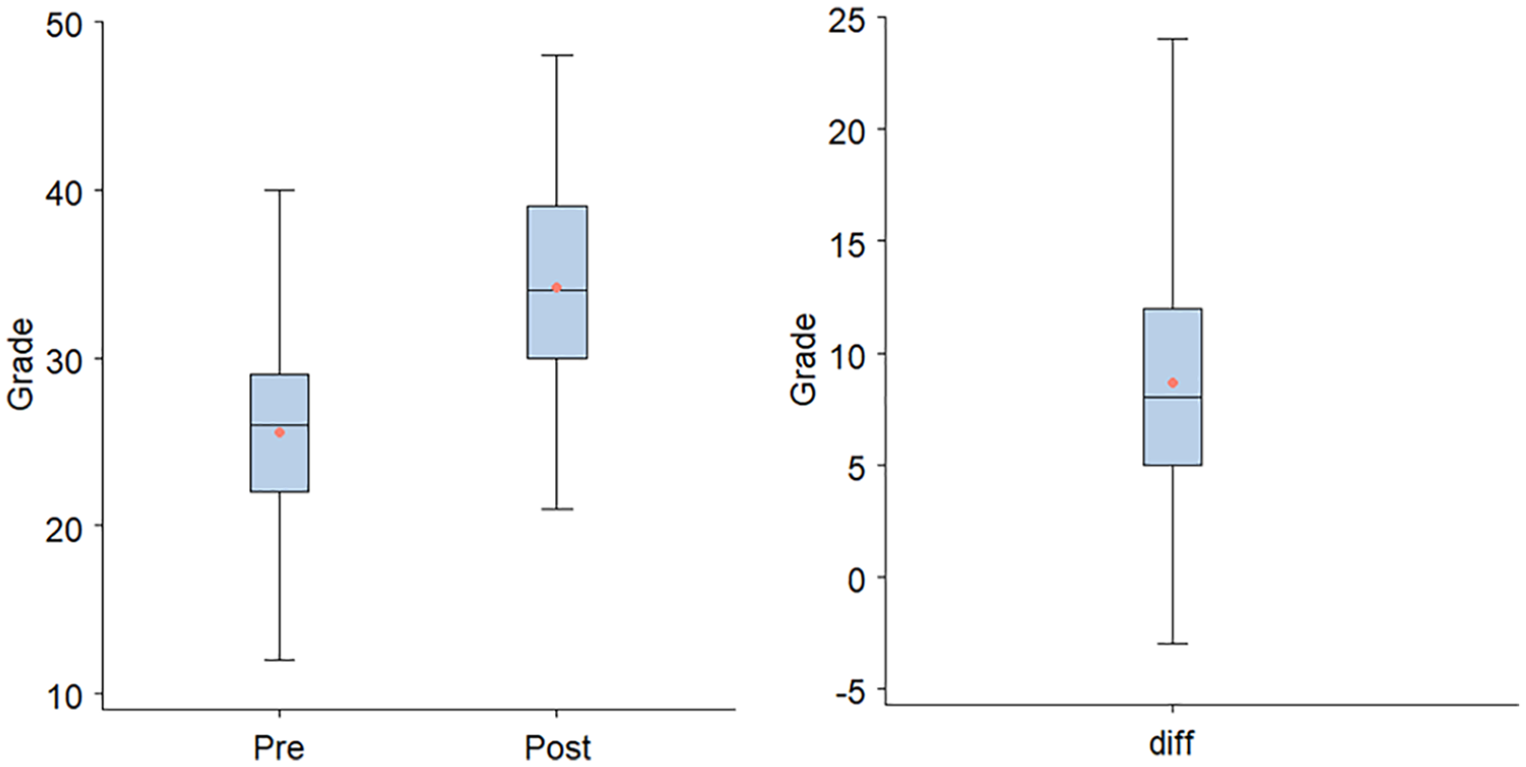
Box plots of exam grades (pre-rotation grade, post-rotation grade, and difference between post and pre rotation exam grade (post-pre)), overall where endpoint of upper whisker represents maximum, upper edge of box represents the third quartile (75th percentile), line inside box represents median (50th percentile), symbol marker represents mean, lower edge of box represents the first quartile (25th percentile), and endpoint of lower whisker represents minimum.
The analysis of the exam grades by gender revealed that according to the analysis of the 2-sample t-tests, Females had statistically significantly higher pre-rotation/post-rotation exam grade than males. Females also had a statistically significantly larger difference in post-rotation and pre-rotation exam grade than males indicating that they improved more in the post rotation exam. The results of the paired t-test indicated that there was a statistically significant difference between post and pre rotation exam grade for females (t (115) = 19.74, P < .0001) and males (t (102) = 14.41, P < .0001) (Table 2).
Descriptive Statistics of Exam Grades (Pre-Rotation Grade, Post-Rotation Grade, and Difference between Post and Pre Rotation Exam Grade (Post-Pre)), by Gender.
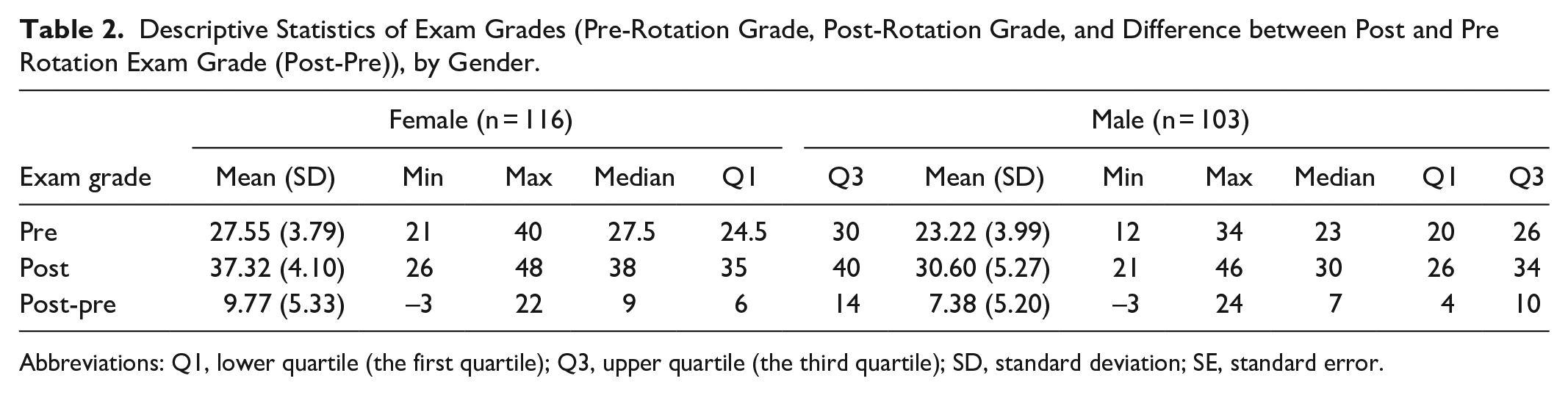
Abbreviations: Q1, lower quartile (the first quartile); Q3, upper quartile (the third quartile); SD, standard deviation; SE, standard error.
According to the results of paired t-tests, post-rotation exam grade was statistically significantly higher than pre-rotation exam grade for subjects in all rotational groups. (Table 3) 1-way ANOVAs were performed to determine if there was a statistically significant difference in exam grades among the 4 rotation groups. Rotation group 1 had statistically significantly lower pre-rotation and post rotation exam grades than all other rotation groups. Rotation groups 2 and 3 (all females) had a statistically significantly higher pre-rotation and post rotation exam grades than rotation group 4. There was no statistically significant difference in pre-rotation and post rotation exam grades between groups 2 and 3 (P = .4036/P = .2196 respectively).
Descriptive Statistics of Exam Grades (Pre-Rotation Grade, Post-Rotation Grade, and Difference between Post and Pre Rotation Exam Grade (Post-Pre)), by Rotation Group.

Abbreviations: Q1, lower quartile (the first quartile); Q3, upper quartile (the third quartile); SD, standard deviation; SE, standard error.
The improvement in exam grades for rotation group 1 was statistically significantly less than rotation groups 2, 3, and 4. There was no statistically significant difference in differences between post-and-pre-rotation exam grades between groups 2 and 3 (P = .9755), between groups 2 and 4 (P = .9966), and between groups 3 and 4 (P = .9279) (Table 4).
Improvement of Exam Grades between Different Rotation Groups by Pairwise Comparisons.

n = 53, 58, 58, and 50 for rotation group 1, 2, 3, and 4, respectively.
Abbreviations: P, P-value; t, t-statistic.
Indicates significance at the 0.05 level.
By analyzing the results for exam ratings, by gender and by rotation group, it was found that among the 219 subjects, nearly 60% (59.36%) considered the exam difficult before the rotation; however, only around 40% (40.18%) considered the exam difficult after the rotation. Females were more likely to consider the exam difficult than males (% difficult: 69.83% for female and 47.57% for male). Similar observations were found in terms of rotation group as rotation groups 2 and 3 (all females) were more likely to consider the exam difficult than rotation group 1 and 4 (all males) (% difficult: 47.17% for group 1, 48.00% for group 4, 75.86% for group 2, and 63.79% for group 3). This was statistically significant for gender (χ2 (2) = 11.7595, P = .0028) and rotation group (χ2 (6) = 16.1164, p = .0131).
According to the results of the odds ratio (Table 5), regardless of time (pre-rotation or post-rotation), subjects with higher exam grade were statistically significantly less likely to consider exam difficult (OR = 0.927, 95% CI = (0.885, 0.970)). And regardless of time (pre-rotation or post-rotation), subjects in rotation group 1 were statistically significantly less likely to consider exam difficult than subjects in group 2 (OR = 0.130, 95% CI = (0.065, 0.259)), group 3 (OR = 0.157, 95% CI = (0.079, 0.312)), and group 4 (OR = 0.491, 95% CI = (0.271, 0.891)). Subjects in group 2 (OR = 3.790, 95% CI = (2.066, 6.955)) and group 3 (OR = 3.127, 95% CI = (1.721, 5.661)) were statistically significantly more likely to consider exam difficult than subjects in group 4 indicating that females are more likely to consider exam difficult than males and this was statistically significant in the ordinal logistic regression model (OR = 4.195, 95% CI = (2.551, 6.896).
The Odds Ratio Estimates for Effect of Exam Grades and Group Number on Exam Rating (For Fignificant Effect Only).

Abbreviations: CI, confidence interval; Diff, estimated mean differences between groups i and j; Lower, lower bound of CI; OR, odds ratio; P, P-value; SE, standard error; Upper bound of CI; z, z-statistic.
Indicates significance at the 0.05 level.
Discussion
Traditionally, the medical environment encourages learning through extensive facts to enhance medical knowledge and to adapt the disease-oriented approach in medical encounters rather than the simpler and cost-effective approach of “rational problem solving of the commoner medical problem.” 11 This is where the importance of incorporating family medicine in a linear method through the clinical medical years really shines. It should be an integral part of any medical curriculum helping students understand the role of this specialty in leading the health care system with high quality and a patient advocating matter. 12
Multiple choice questions (MCQs) were used to asses’ students’ basic family medicine knowledge prior to taking the family medicine clerkship. This method was used as it is the best estimator of the “knows” area of miller’s pyramid. 13 MCQs are also a quick and objective method of knowledge estimation. 14
We have found that students’ grades in general improved at least a full grade on average in their test scores after completing the clinical rotation. This was similar throughout the year and for all batches indicating that students’ knowledge did improve with the clinical exposure and the hands-on experience. Although, in order to properly asses the improvement in medical knowledge, skills should be assessed as well and the grading to be taking into consideration. 15 The most accurate method to do so was proven in many literature reviews to be the OSCE.16,17 We sufficiently chose the more convenient method of MCQs to evaluate student’s comprehension and grasp over material taught by possibly spanning through Bloom’s taxonomy of the course educational objectives. It has been reported as well that MCQ grading and OSCE grading are not necessarily correlated for the same student and for students with different achievement levels. 18
This study demonstrated that female students did better in the rotation globally. They scored higher in tests at the beginning of the rotation, even before it started and scored better afterwards. Their grade of improvement was higher than their fellow male medical students as well. This fact is not a strange one, as it has been long observed and reported worldwide. Two studies did come up with the same conclusion here in the Kingdom. The first one showed that both the global score for the whole course where OSCE and portfolio scores were included as well as the written MCQ exam, were better for the female students with a mean of 81.5 ± 7 compared to 76.8 ± 9 for male students. In the other study, Female students also scored significantly more compared to male students in total (60.8 ± 7.42% vs. 56.81 ± 8.78%) as well as individually in MCQs.19,20 However, in 1 study done in the capital, Riyadh city, no statistically significant difference in global exam scoring was appreciated between male and female students taking the psychiatry course. 18
Several factors could contribute in the explanation of such a finding. Some social factors could include that female students are less influenced by their peers or what is called “peer pressure” as they are more focused and grounded. 21 The dominance of males in the medical field makes female students at a constant struggle to prove themselves. 22 Other physiological factors could include the previously reported fact that females are better at scanning the physical environment and associative memory. 23 Anatomically females have much more white matter in the sulci of memory and intelligence brain areas. 24
Although female students scored better, it was observed that they tended to rate the exam as hard more than their male counterparts. This observation was reported in a previous study pertaining to student’s perception of the OSCE as an undergraduate assessment tool. Although the exam was perceived positively, female students rated it as hard more often than male students. 25 This may be explained by the anxiety that exams usually trigger 26 and that females are more prone to anxiety then males. 27
Conclusion
This study demonstrated that students benefited, at least as an increase in knowledge and cognitive skill, after taking the course of family medicine clerkship that included a condensed exposure to clinical training and formal lecturing. This helps in advocating for both the importance of this specialty locally and globally and for the university’s decision in incorporating family medicine as a major clinical rotation for undergraduates in their clinical years.
As we have demonstrated an improvement in medical students’ cognitive knowledge in the field of family medicine after partaking in the newly introduced family medicine clerkship rotation, further studies that focus on the impact of such rotations on the students’ clinical skills is advisable.
Footnotes
Author Contributions
MA, NA, and AS designed the study. AS prepared the exam. MA, NA, and MD, collected the data. AS and SA conducted the statistical analysis. MA, NA, and MD analyzed the data. MA and SA wrote the main manuscript. All authors critically reviewed approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
Approvals necessary were obtained from the students council and the vice dean of academic affairs in the college of medicine September 17, 2018. A written consent was obtained from all participating students.
Availability of Data and Material
All materials used in this research are available from the corresponding author upon request.