
Abstract
Introduction/Objectives:
Pre-exposure prophylaxis (PrEP) use in the southern United States is low despite its effectiveness in preventing HIV acquisition and high regional HIV prevalence. Our objectives were to assess PrEP knowledge, attitudes, and prescribing practices among Tennessee primary care providers.
Methods:
We developed an anonymous cross-sectional electronic survey from March to November 2019. Survey development was guided by the Capability, Opportunity, Motivation, and Behavior framework and refined through piloting and interviews. Participants included members of professional society and health center listservs licensed to practice in Tennessee. Respondents were excluded if they did not complete the question regarding PrEP prescription in the previous year or were not in a position to prescribe PrEP (e.g., hospital medicine). Metrics included PrEP prescription in the preceding year, PrEP knowledge scores (range 0-8), provider attitudes about PrEP, and provider and practice characteristics. Knowledge scores and categorical variables were compared across PrEP prescriber status with Wilcoxon rank-sum and Fisher’s exact tests, respectively.
Results:
Of 147 survey responses, 99 were included and 43 (43%) reported PrEP prescription in the preceding year. Compared with non-prescribers: prescribers had higher median PrEP knowledge scores (7.3 vs 5.6, P < .01), a higher proportion had self-reported patient PrEP inquiries (95% vs 21%, P < .01), and a higher proportion had self-reported good or excellent ability to take a sexual history (83% vs 58%, P = .01) and comfort taking a sexual history (92% vs 63%, P < .01) from men who have sex with men, a subgroup with high HIV risk. Most respondents felt obligated to provide PrEP (65%), and felt all primary care providers should provide PrEP (63%).
Conclusion:
PrEP provision is significantly associated with PrEP knowledge, patient PrEP inquiries, and provider sexual history taking ability and comfort. Future research should evaluate temporal relationships between these associations and PrEP prescription as potential routes to increase PrEP provision.
Introduction
Over 1 million individuals in the United States (U.S.) are estimated to be living with HIV, and there were over 37 000 estimated new HIV-infections in 2018. 1 About 70% of new U.S. HIV-infections occurred in men who have sex with men (MSM), followed by heterosexually active adults and people who inject drugs (PWID). 1 One objective of the 2019 U.S. Ending the HIV Epidemic (EHE) initiative is to prevent new HIV-infections using proven interventions, including HIV pre-exposure prophylaxis (PrEP). 2 The Food and Drug Administration (FDA) has approved 2 combination antiretroviral drugs for PrEP: emtricitabine-tenofovir disoproxil fumarate (FTC/TDF), 3 and emtricitabine-tenofovir alafenamide (FTC/TAF). 4 If taken daily by an HIV-negative individual, PrEP provides over 90% reduction in HIV acquisition.5-7
It is estimated that over 1.2 million adults in the U.S. are eligible for PrEP, including 25% of sexually active MSM, 19% of PWID, and 0.4% of heterosexually active adults. 8 PrEP use is on the rise in all regions of the U.S., however overall uptake of PrEP is low,9-14 and there is a discordance between the number of PrEP providers and persons at high risk for HIV. 15 This is most notable in the U.S. South, which despite having the highest regional burden of new HIV diagnoses (and approximately half of the country’s new HIV diagnoses) 1 contains only 25% of the nation’s PrEP providers 15 and has the lowest PrEP use relative to the number of new HIV diagnoses. 16 Regions of the South are also vulnerable to injection drug use-associated HIV transmission, in part due to limited availability of harm reduction programs and disproportionately low PrEP use among PWID.17-19 Among the priority geographic areas identified in the U.S. EHE initiative, 6 of the 7 states with high rural HIV burdens and 23 of the 48 high HIV burden counties are in the South. 20
Despite the need to characterize unique aspects of the U.S. South that may limit PrEP provision, most provider surveys have not specifically targeted Southern healthcare providers.21,22 Additionally, contemporary data is lacking on provider barriers to PrEP prescription following CDC (2017) 23 and USPSTF (drafted 2018, 24 finalized 2019 25 ) recommendations regarding PrEP use, which prior surveys had reported could increase PrEP prescription.26,27 We developed a survey for primary care providers (PCPs) in Tennessee (TN), a state located in the U.S. South, to examine behaviors, knowledge, and attitudes surrounding PrEP in order to inform future research and interventions to facilitate more robust provision of PrEP and, ultimately, reduce HIV incidence in TN.
Methods
We conducted a cross-sectional survey among TN PCPs to examine PrEP knowledge, attitudes, and prescribing practices. Survey development was informed by prior literature and the Capability, Opportunity, and Motivation (COM-B) theoretical framework of behavior, which facilitated comprehensive assessment of factors influencing the behavior of PrEP prescription (Table 1). 28 The primary outcome of interest was provider self-reported prescription of PrEP within the year preceding survey administration. Preliminary data from pilot testing (n = 25) and qualitative analysis of open-ended interviews (n = 8) were used to refine the final questionnaire, which consisted of 56 questions (https://redcap.vanderbilt.edu/surveys/?s=KLHA3YDC3X).
Survey Topics Organized by COM-B Framework.

Abbreviations: COM-B, capability, opportunity, motivation, and behavior; PrEP, pre-exposure prophylaxis.
There were 7 questions about provider demographics that did not fall into the COM-B framework (county of practice, gender, sexual orientation, race, ethnicity, type of practice).
Eligible respondents included physicians, nurse practitioners (NPs), physician assistants (PAs), and pharmacists in the fields of Internal Medicine (IM), Medicine-Pediatrics, Family Medicine, Infectious Diseases (ID), and Obstetrics-gynecology (Ob-gyn) licensed to practice in TN. The electronic survey was disseminated via email to employees of TN medical centers, and to members of professional society listservs. Respondents were excluded if they did not indicate if they had prescribed PrEP in the past year or were not in a position to prescribe PrEP (e.g., nurses, providers who worked primarily in an inpatient setting). A minimum sample size was not calculated given the formative nature of the research.
Surveys were collected and managed using Research Electronic Data Capture (REDCap).29,30 The final survey was disseminated in March 2019 as a REDCap link via email, and 2 reminder emails were sent. Respondents were anonymous, and no follow-up occurred. Survey data were downloaded for analysis in November 2019. A PrEP knowledge score was calculated from 8 equally-weighted knowledge questions (total score range 0-8). “Select all that apply” questions were scored as 1 point if all correct answers were selected, a fraction of a point when at least 1 but not all correct answers were selected, 0 points if no correct answers were selected, or “missing” if both the directly preceding and directly subsequent multiple choice questions were missing. Scores were not calculated for surveys missing knowledge question responses. The knowledge questions as an aggregate tool were not previously reported in literature, but were informed by CDC guidelines and input from local providers with substantial clinical expertise in providing PrEP. Other methods of operationalizing PrEP knowledge were not employed given the lack of validated tools.
The sample was characterized with descriptive statistics. The median and IQR were reported for knowledge scores as a continuous variable; all other variables were categorical and reported as counts and proportions. Incomplete surveys were incorporated into the analysis if the primary outcome (PrEP prescription in the previous 12 months) was answered. Missing values for variables other than the primary outcome were excluded when making comparisons. Fisher’s exact tests were used to compare categorical variables, both for global tests of provider characteristics and for pairwise 2-by-2 tests comparing mutually exclusive categories within individual characteristics across PrEP prescribing practices. Kruskal-Wallis tests were used to assess knowledge scores across provider characteristics, and Wilcoxon rank-sum tests were used to compare knowledge scores across 2 mutually exclusive categories within individual characteristics across PrEP prescribing practices. The final sample size did not permit multivariable analysis. Cronbach’s alpha was reported for the knowledge tool to assess internal consistency. Data were analyzed in Stata version 15.1 and are available upon request from the corresponding author (StataCorp, College Station, TX).
Results
Of 147 returned surveys, 99 (67%) were included for analysis. Surveys missing the primary outcome were excluded (n = 21), and were attributed to respondents exiting the survey early; the number of missing values trended upward for each question. The other surveys (n = 27) were excluded for respondent inability to prescribe PrEP.
Among 99 included surveys, 43 (43%) had prescribed PrEP in the previous 12 months. All respondents trained in ID had prescribed PrEP (n = 3). A higher proportion of PrEP prescribers trained in IM or ID compared to non-prescribers (56% vs 25%, P < .01), and a lower proportion of PrEP prescribers were NPs or Ob-gyn trained, compared to non-prescribers (12% vs 34%, P = .02 and 2% vs 18%, P = .02, respectively) (Table 2). The majority of PrEP prescribers were located in the Nashville/Davidson County TN Department of Health region (n = 18) (Figure 1). 31
Provider and Practice Characteristics by PrEP Prescriber Status.
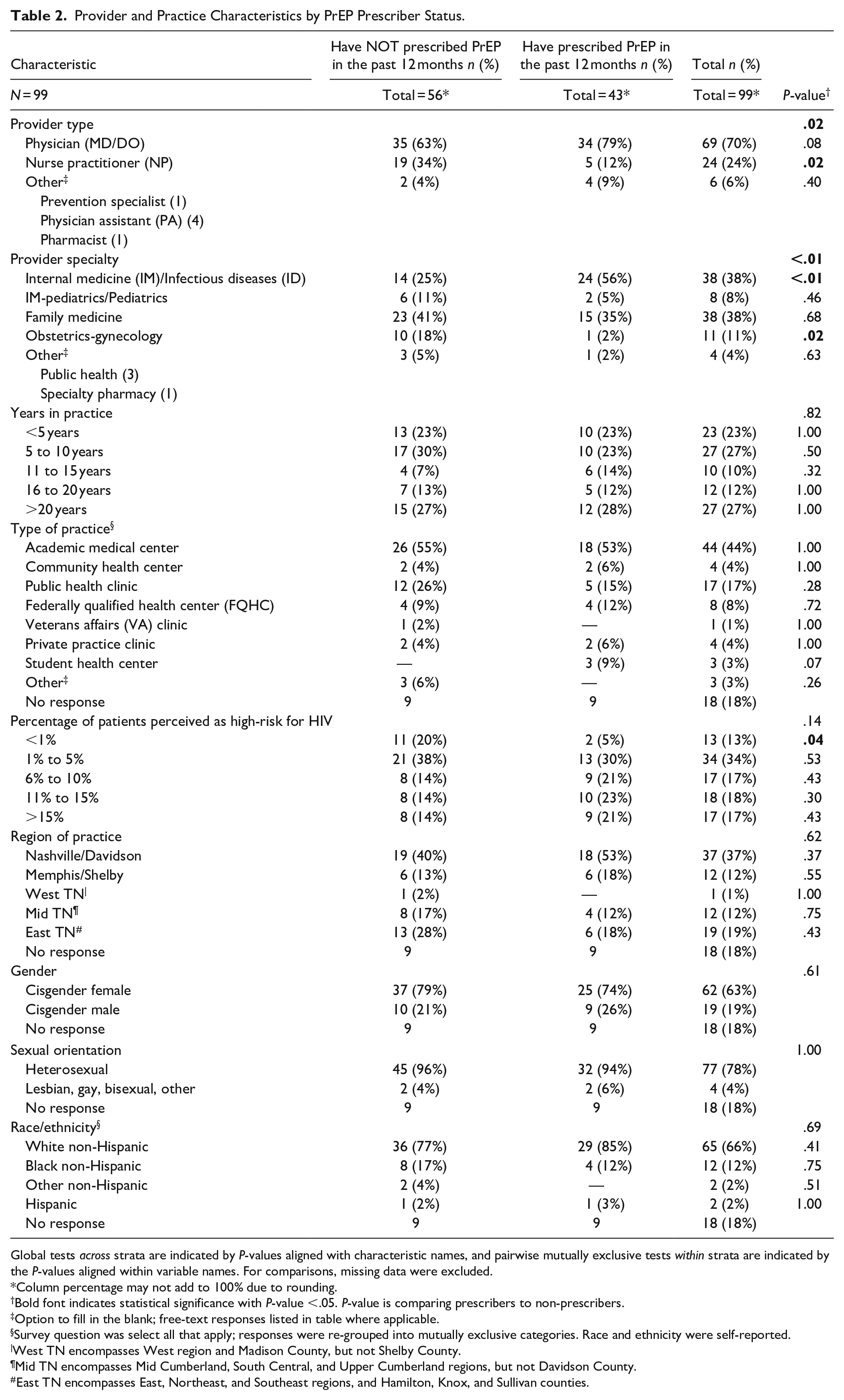
Global tests across strata are indicated by P-values aligned with characteristic names, and pairwise mutually exclusive tests within strata are indicated by the P-values aligned within variable names. For comparisons, missing data were excluded.
Column percentage may not add to 100% due to rounding.
Bold font indicates statistical significance with P-value <.05. P-value is comparing prescribers to non-prescribers.
Option to fill in the blank; free-text responses listed in table where applicable.
Survey question was select all that apply; responses were re-grouped into mutually exclusive categories. Race and ethnicity were self-reported.
West TN encompasses West region and Madison County, but not Shelby County.
Mid TN encompasses Mid Cumberland, South Central, and Upper Cumberland regions, but not Davidson County.
East TN encompasses East, Northeast, and Southeast regions, and Hamilton, Knox, and Sullivan counties.

New HIV diagnoses per 100 000 residents and number of PrEP provider survey respondents by public health region of TN.
A PrEP knowledge score was calculated for 87 (88%) participants. The median PrEP knowledge score was 6.3 (Interquartile Range [IQR] 5-7.5). Median knowledge scores were higher among prescribers (7.3, IQR 5.7-7.6) compared to non-prescribers (5.6, IQR 4.6-6.6, P < .01) (Figure 2).

Violin plot showing distribution of PrEP knowledge scores by PrEP prescriber status.
Cronbach’s alpha was 0.57 for the final knowledge tool. Total knowledge scores did not vary significantly across any global provider characteristic. Within provider characteristics across PrEP prescriber status, prescribers had significantly higher knowledge scores than nonprescribers for multiple groups including physicians, NPs, IM, and ID physicians (Supplemental Table 1). Significantly more prescribers than nonprescribers knew that FTC/TDF was approved for use as PrEP (100% vs 86%, P = .02), but only 27% of all respondents, and 23% of PrEP prescribers, answered the question regarding CDC recommendations for patient PrEP eligibility with complete accuracy (Table 3).
Individual PrEP Knowledge Questions Stratified by Prescriber Status.

Abbreviations: CDC, Centers for Disease Control; PrEP, pre-exposure prophylaxis.
For select all that apply questions, n (%) recorded reflects participants who selected all correct options available; no partial credit reflected here.
Column percentage may not add to 100% due to rounding.
Bold font indicates statistical significance with P-value <.05. P-value is comparing prescribers to non-prescribers. Pairwise mutually exclusive tests of question score by prescriber status within a variable are indicated by the P-value aligned with the variable value. For comparisons, missing data were excluded.
At the time of survey dissemination, Descovy had not yet been approved by the FDA.
Respondents most frequently believed that sexual risk compensation (44%) and serious adverse events (72%) due to PrEP were Very Unlikely or Unlikely, that optimal PrEP adherence was Very Likely or Likely (40%), and that financial difficulties with PrEP were Very Likely or Likely (45%). No respondent was morally opposed to PrEP among those that answered (n = 81). The majority of all respondents reported a sense of obligation to provide PrEP (65%), and a higher proportion of prescribers reported feeling obligated to provide PrEP compared to non-prescribers (91% vs 70%, P = .03). Most respondents felt that all PCPs should provide PrEP (63%) (Table 4).
Provider Beliefs About PrEP by Prescriber Status.

Abbreviations: PCP, primary care provider; PrEP, pre-exposure prophylaxis.
Global tests across strata are indicated by P-values aligned with characteristic names, and pairwise mutually exclusive tests within strata are indicated by the P-values aligned within variable names.
Column percentage may not add to 100% due to rounding.
Bold font indicates statistical significance with P-value <.05. P-value is comparing prescribers to non-prescribers. For comparisons, missing data were excluded.
Among the 43 providers who prescribed PrEP, all but 2 had a patient inquire about it, with a higher proportion of prescribers than non-prescribers reporting patient PrEP inquiry (95% vs 21%, P < .01). Over half (53%) of all non-prescribers were willing to prescribe PrEP if a patient requested it (Supplemental Table 2). Almost half of respondents reporting taking sexual histories at Every or Most encounters (49%), with no difference by prescriber status. A higher proportion of prescribers reported Good or Excellent sexual history taking ability for MSM and heterosexual males (83% vs 58%, P = .01; 86% vs 62%, P = .01; respectively) compared to non-prescribers. Respondents most frequently reported Good or Excellent sexual history taking ability for younger patients (83%) and heterosexual female patients (81%).
A higher proportion of prescribers reported Good or Excellent comfort with taking sexual histories from MSM (92% vs 63%, P < .01), heterosexual males (92% vs 69%, P < .01), heterosexual females (95% vs 78%, P = .04), and younger patients (100% vs 82%, P < .01) compared to non-prescribers. Overall, respondents least frequently reported Good or Excellent ability (49%) and comfort (52%) when taking sexual histories from transgender patients (Supplemental Table 3, Figure 3). Respondents most often reported prescribing PrEP to MSM (40%), followed by the HIV-negative member of a serodiscordant couple (19%), commercial sex workers (4%), and PWID (2%).
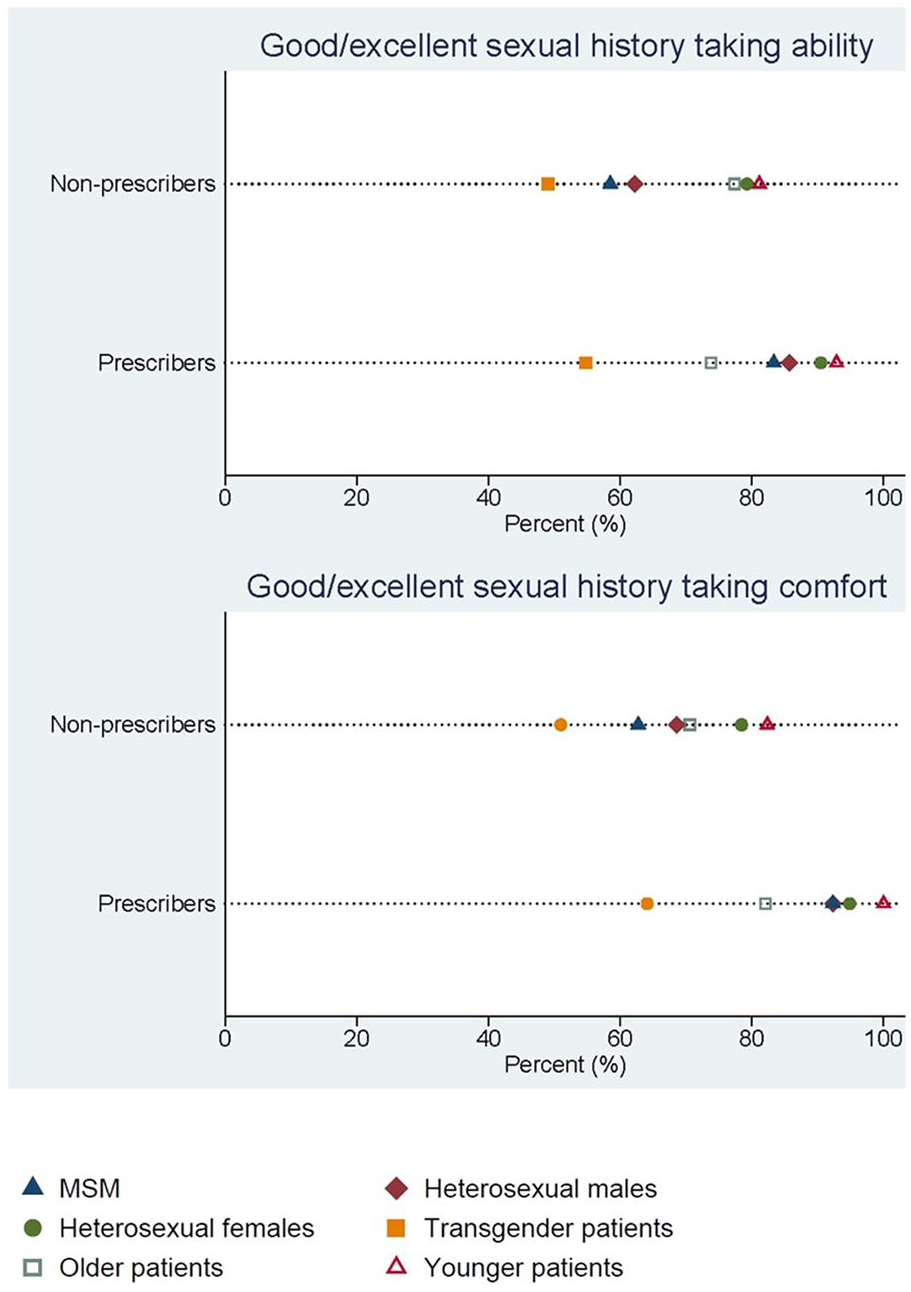
Sexual history ability and comfort by PrEP prescriber status for different patient populations.
Both prescribers and non-prescribers of PrEP cited PrEP costs (26% and 51%, respectively) and need for administrative support (26% and 49%, respectively) as predominant barriers to PrEP provision. Non-prescribers most frequently reported that PrEP online trainings (57%), educational events (53%), and knowledgeable providers within their practice (49%) could increase PrEP provision, and most frequently wanted training in PrEP contraindications (69%) and adverse effects (57%) (Supplemental Table 4).
Discussion
Though less than half (43%) of survey respondents had prescribed PrEP in the previous 12 months, this proportion is greater than previously reported in the literature (4%-39%),26,27,32-35 excluding one convenience sample of Philadelphia HIV/ID and non-HIV providers with an unusually high rate of PrEP prescription (77%). 36 Our finding may reflect the trend of increasing PrEP provision over time. 14 Provider surveys that included both PCPs and HIV/ID specialists have consistently reported that PCPs prescribed PrEP less often than HIV/ID specialists;26,27,32,36 given that our results were primarily gathered from PCPs with very few responses from ID specialists (n = 3), this increased proportion of PrEP prescribers may be reflective of TN PCPs in general.
The majority of survey respondents felt that all PCPs should provide PrEP rather than just a subset (63%), and felt obligated to provide PrEP (65%). This is in contrast to the previously described “purview paradox” denoting disagreement about whether PCPs or HIV/ID specialists should provide PrEP.37,38 Perhaps as data regarding PrEP usage and adverse events become more prevalent 39 providers are more open to prescribing it,26,27 but a clear disconnect remains between willingness to prescribe PrEP and actual prescription.
In our survey, PrEP knowledge scores were significantly associated with PrEP prescription, and prescribers had higher knowledge scores than non-prescribers across multiple respondent categories, analogous to prior literature demonstrating lack of knowledge as a barrier to PrEP provision.22,26,40 The calculated Cronbach’s alpha value was less than the often-cited ideal value of 0.7, but reflects the fact that we assessed multiple domains of PrEP knowledge (e.g., patient eligibility, lab monitoring, medication specifics) and knowledge of each domain varies within each respondent; there were too few questions to assess the alpha of each domain individually. Further refinements of the knowledge tool (i.e., increasing the length) are needed to improve internal consistency.
Our findings support literature demonstrating that patient request of PrEP may play an important role in PrEP prescription.26,37,41 In our sample, over half of non-prescribers reported willingness to prescribe PrEP if a patient requested it, and almost every prescriber reported patient inquiry. A study of Veterans Affairs patients who received PrEP showed that 94% of PrEP conversations were patient-initiated and recipients were often already educated about PrEP at the time of request, 42 overall indicating that an undue burden may be being placed on patients to initiate conversations around PrEP.
PrEP provision ideally belongs in the primary care setting, and effectively integrating PrEP into clinical practice will require routinizing patient screening for HIV risk and PrEP eligibility.43,44 This is reinforced by the fact that only 27% of all respondents, and 23% of PrEP prescribers, were able to identify patient groups who are eligible for PrEP with complete accuracy. This process necessarily must be directed by the provider rather than the patient, given that patients may not volunteer information about their sexual practices45,46 or accurately self-assess their need for PrEP. 47 In our survey, only about half of both prescriber and non-prescriber groups reported taking a sexual history at every/most encounters, similar to prior observational studies.48-50 While the frequency of sexual history taking did not differ significantly between PrEP prescribers and non-prescribers, it is broadly relevant given that patients’ need for PrEP evolves with their behavior and therefore necessitates frequent provider assessment.
A higher proportion of PrEP prescribers reported greater ability and comfort when taking a sexual history for several patient populations including MSM, a group at high risk of acquiring HIV. 51 Both prescribers and non-prescribers in our sample felt the least comfortable and skilled when taking sexual histories from transgender patients, which is concerning given that this group is at particularly high risk of acquiring HIV. 52 Prior qualitative literature has noted low ability to assess HIV risk as a barrier to PrEP provision,37,53 and deficits in provider sexual history taking may contribute to disparities in PrEP awareness and use among high risk populations.44,54,55
Selection bias is one study limitation. TN does not have a readily-accessible database of provider contact information, resulting in our use of multiple avenues for survey dissemination. Given difficulty identifying who viewed the survey link, we also could not accurately report a response rate. The cross-sectional nature of the data limits our ability to draw conclusions about the temporality of associations connecting behaviors with PrEP prescription. Respondents were most frequently physicians (70%), practiced primarily in an academic medical center (44%), and practiced primarily in Davidson County (37%), which is not representative of all TN PCPs and limits the generalizability of our findings. Respondents may be more likely to complete the survey if they had already prescribed PrEP, but as sample proportions of prescribers and non-prescribers were similar it is likely that both groups were adequately represented. Respondents may be more likely to respond favorably about PrEP due to social desirability bias, but this was minimized through the anonymous nature of the survey. Lastly, we did not assess provider skills when taking a substance use history. The HIV care continuum for PWID in TN is not known, 56 and given that only 2% of respondents had prescribed PrEP to PWID, this represents an important opportunity for future research on barriers to PrEP provision to patients with non-sexual risk behaviors.
Conclusion
PrEP prescription by TN PCPs is associated with many potentially modifiable factors, such as patient inquiry about PrEP, PCP PrEP knowledge, and PCP sexual health skills. There is a need for prospective studies evaluating temporal relationships between these associations and PrEP provision, and evaluating barriers to PrEP provision for PWID, given their potential for informing public health interventions to increase PrEP prescription and reduce the incidence of HIV infection in TN.
Supplemental Material
sj-pdf-1-jpc-10.1177_2150132720984416 – Supplemental material for Tennessee Healthcare Provider Practices, Attitudes, and Knowledge Around HIV Pre-Exposure Prophylaxis
Supplemental material, sj-pdf-1-jpc-10.1177_2150132720984416 for Tennessee Healthcare Provider Practices, Attitudes, and Knowledge Around HIV Pre-Exposure Prophylaxis by Emily Moore, Sean G. Kelly, Leah Alexander, Patrick Luther, Robert Cooper, Peter F. Rebeiro, Autumn D. Zuckerman, Margaret Hargreaves, Kassem Bourgi, David Schlundt, Kemberlee Bonnet and April C. Pettit in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
This study was granted exemption by Vanderbilt University’s Institutional Review Board. Input from the TN MSM Task Force made this project possible. Preliminary results were presented at IDWeek, October, 2019.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: One author reports grant and advisory board member payments from Gilead Sciences and Theratechnologies. All authors have no other conflicts of interest to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health [R01 MH113438], the Vanderbilt Institute for Clinical and Translational Research [UL1 TR000445], the TN Center for AIDS Research [P30 AI110527] and the Infectious Diseases Society of America Grants for Emerging Researchers/Clinician Mentorship (G.E.R.M.) Award.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.