
Abstract
Keywords
Introduction
Of the 30.3 million afflicted by the diabetes epidemic in the United States, Latinos are among the most affected. More recently, with the COVID-19 (coronavirus disease 2019) pandemic, being Latino and having diabetes has been associated with a higher mortality rate.1,2 Despite nationwide interest in reducing type 2 diabetes through nationwide promotion of the Centers for Disease Control and Prevention (CDC) approved National Diabetes Prevention Program (NDPP), Latinos, especially low-income Latino women (“Latinas”), continue to experience diabetes health disparities.3,4 The NDPP promotes the adoption of “preventive behaviors” (healthy eating, moderate physical activity) through weekly classes held for 16 weeks followed by bimonthly or monthly meetings for the remainder of a year. The program has been culturally adapted and translated for low income individuals and those with minimal formal education, but in most cases, enrollment and results among Latinos continue to lag behind those of non-Hispanic Whites. 5 Even when attending at no cost, only 30.8% of Latinos achieve the weight loss goal (losing 5% of initial weight) compared to 43.2% of non-Hispanic Whites, and their attendance is minimal. 6 Based on this success gap between Latinos and non-Hispanic Whites, reducing the diabetes health disparity and the subsequent COVID-19 disproportionate mortality affecting Latinos seems elusive.
Several studies have partially attributed unhealthy behaviors and the resulting health disparities among low-income Latinos to lack of access to healthy food, transportation, and childcare,7,8 while recent studies indicate “food deserts” (areas with reduced access to affordable healthy food, if any) have little impact on eating behaviors of low-income communities. 9 Still other studies have credited successful adoption of preventive behaviors to readiness to change (RTC) behaviors.10-12 Assessing RTC is important enough that healthcare providers are strongly advised to assess RTC before recommending behavior modification to their patients. 13 In the context of diabetes prevention, participants in the landmark Diabetes Prevention Program (DPP)—after which NDPP programs are modeled—were highly screened for RTC and for their ability to adopt and maintain healthy behaviors. 14
The concept of RTC stems from the transtheoretical model (TTM) of behavior change, which posits that individuals gradually progress through mental and emotional stages before engaging in any behavior. 15 According to the TTM, individuals weigh pros and cons—“decisional balance”—before adopting new behaviors, and changes only happen once the perceived benefits outweigh the perceived disadvantages of retaining the current behaviors.16-18 To apply this concept to Latinas enrolled in a program, they would have to arrive at a “decisional balance” whereby the perceived advantages of engaging in “preventive behaviors” outweigh the disadvantages of retaining the current behaviors.
The RTC of participants in the NDPP and translations of the DPP is seldom reported, and studies addressing readiness among Latinas at risk of diabetes have been far and few in between. 14 Instead, DPPs enroll individuals based on referrals and mostly biometric criteria, and impart knowledge and skills, expecting behavior modification to follow soon after enrollment, as if all individuals enrolled are “ready” to immediately adopt recommended behaviors.19,20 Indeed, limited research is available on RTC of Latinas enrolling in prevention programs and even less on factors associated with their readiness to adopt and retain the “preventive behaviors.”8,19 However, there is reason to believe that this information could help predict the success of interventions in this population. 21
The objective of this study is to first explore readiness to adopt preventive behaviors of low-income Latinas who enroll in a DPP, and then to identify factors associated with adoption of, and adherence to, recommended preventive behaviors.
Methods
Research Design and Sample
This qualitative study was completed with forty Latinas residing in San Bernardino County, California, an area with the third highest rate of diabetes-related mortality in California and one of the largest Hispanic populations in the nation.22,23 The county is also largely considered a “food desert.” 24 Besides self-identifying as Latina, eligibility criteria included (1) attending and completing the Vida Vibrante DPP (see Supplement 1 for program overview); or (2) being a peer educator (promotora) who taught Vida Vibrante. Immediately following program completion, all program participants (3 separate cohorts) were invited to the focus group discussions (FGDs) (n = 37). Key informants (n = 3) completed interviews within 10 days of course completion.
The authors felt that using FGDs would be the most effective method to elicit honest feedback from all participants because it would allow them to express their lived experiences without the constraint of writing, and allow the research team to better capture their perspectives.7,25 Key informant interviews (KIIs) with the promotoras were included for triangulation reasons.
Prior to the FGDs and KIIs, all participants were asked to read and sign an informed consent form in Spanish reviewed and approved by the Loma Linda University Institutional Review Board (Ethics Committee reference #5150145). A $10 gift certificate to a local supermarket was given as compensation for participation.
Data Collection
On program completion, 9 FGDs, each consisting of 3 to 7 participants, and 3 KIIs—all lasting between 15 and 55 minutes—were held in Spanish by 3 bilingual interviewers at the 2 community centers where the interventions had been held, using the consecutive sampling method. Interviewers were trained in qualitative research methods and were familiar with all participants. The interview guide for the semistructured KIIs and FGDs was based on a grounded theory approach by Charmaz informed by the TTM.15,26,27 Probes were used to expand the exploration and allow new issues to be identified. The FGDs and KIIs explored the following 2 topics: (1) baseline readiness level and (2) factors associated with readiness to adopt and adhere to lifestyle preventive behaviors (see Supplement 2 for FGDs and KIIs guides).
All interview questions and FGDs were digitally recorded and transcribed verbatim by bilingual students and faculty experienced with qualitative data analysis immediately after the recordings were obtained. Debriefing sessions were held and field notes recorded. Confidentiality was protected by neither identifying interviewees nor third parties mentioned in the interviews and by de-identifying the transcripts. After research completion, the then anonymous interviews were stored permanently for research purposes at the Institute of Community Partnership (ICP).
Data Analysis
FGDs and interviews transcripts were analyzed for emergent themes supported by critical quotes using the 2017 computer software program MaxQDA (version 12) 28 to code the transcript using an a priori code book. A team of 3 students developed the codebook, which was later expanded as emergent themes were identified and organized. All analyses were done in Spanish. Only quotes included in this article (Table 2) were translated from Spanish into English. Demographic and biometric data, and baseline readiness to change specific behaviors were accessed from Vida Vibrante program database.
Results
Participant Characteristics
Participants ranged in age from 37 to 59 years (mean age 48 ± 11 years), were of lower socioeconomic status, and most had no more than a high school education. Most lived with a spouse/partner and were overweight or obese. These Latinas lived in permanent housing (house, mobile homes, or apartment) and were neither migrant farm workers nor had worked in an agricultural setting. Culturally, all were first-generation immigrants and only 7 (4 from El Salvador and 2 from Guatemala) were not from Mexico. Although Latinas from Central America may not hold the same beliefs about the etiology of diabetes as do Mexicans, they hold similar family values. In most households, only Spanish was spoken (only 4 spoke both English and Spanish). In none of the homes was English the only language spoken. Key informants had some years of education beyond high school but only one had completed college (in her home country). Table 1 displays participants’ baseline characteristics (educational level of key informants not included).
Participants’ Baseline Characteristics (N = 37).

Four central themes emerged from the FGDs and KIIs: (1) readiness to enroll in program is associated with awareness of health deterioration (personal or family) and physician referral; (2) not everyone enrolling is ready to immediately adopt preventive behaviors; (3) factors associated with adoption of, and adherence to, preventive behaviors include family health concerns, better awareness of diabetes complications, and the presence of strong social support; and (4) most barriers to behavior modification were deemed nearly insurmountable. Themes are presented below, and corresponding quotations are included in Table 2.
Themes and Subthemes Derived From Focus Group Discussions and Key Informant Interviews. a
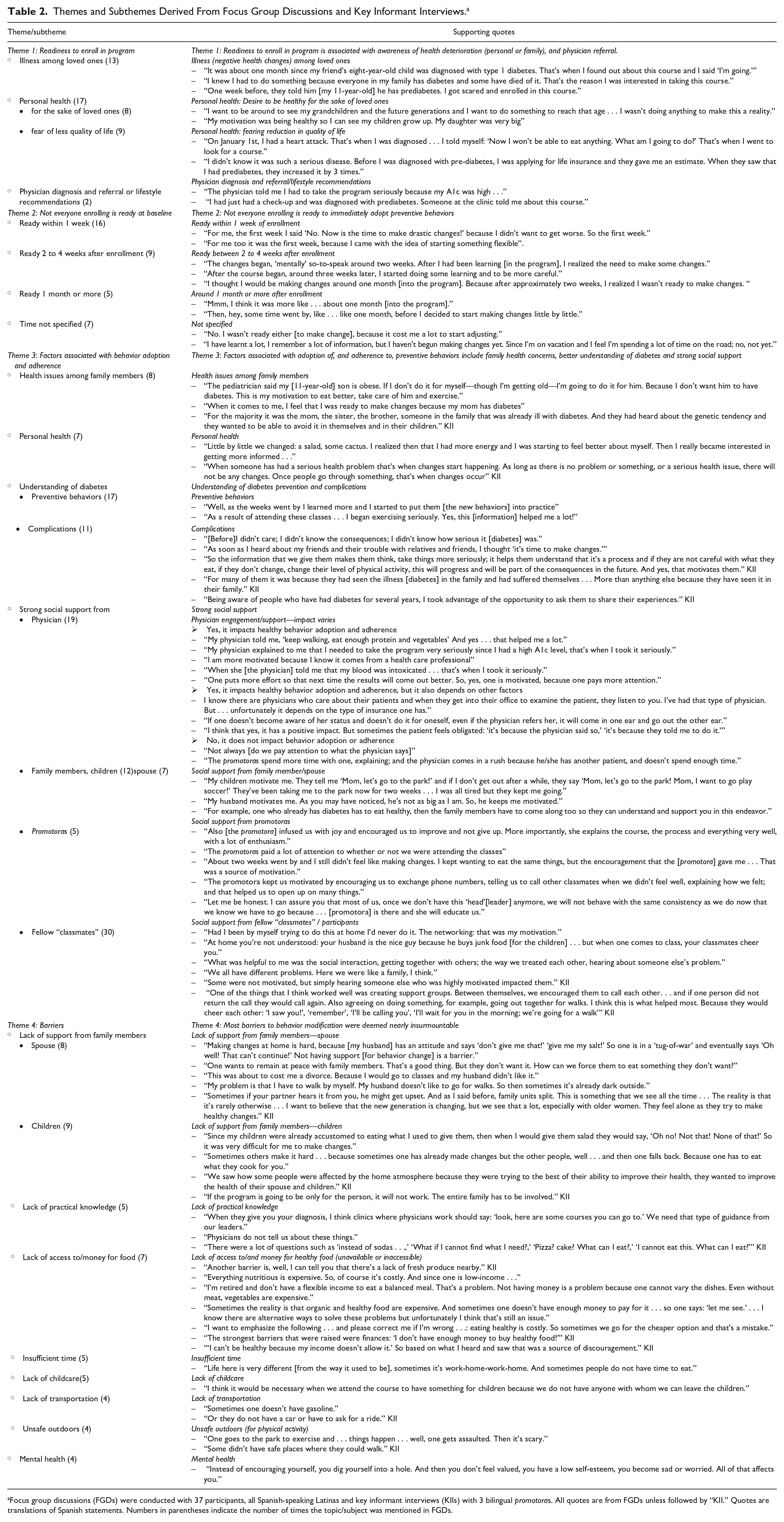
Focus group discussions (FGDs) were conducted with 37 participants, all Spanish-speaking Latinas and key informant interviews (KIIs) with 3 bilingual promotoras. All quotes are from FGDs unless followed by “KII.” Quotes are translations of Spanish statements. Numbers in parentheses indicate the number of times the topic/subject was mentioned in FGDs.
Theme 1: Readiness to enroll in program is associated with awareness of health deterioration (personal or family), and physician referral
Enrolling in the program was clearly associated with the timing of negative news about personal and family health, and the realization that the consequences would have an immediate negative impact on daily personal or family life. While many participants were at risk of developing diabetes due to their body mass index, laboratory results and family history, a frequently cited motivation for enrolling was having a family member, especially a younger family member, recently diagnosed with diabetes or at risk of diabetes. When personal health was mentioned as a reason for enrollment, it was often associated with a desire to make changes for the sake of loved ones and less for personal health concerns. Personal health concerns were usually associated with fear of losing quality of life. Last, a diagnosis leading to health concerns (as mentioned above) or specific lifestyle advice and referral to the prevention program from a physician, also triggered enrollment.
Theme 2: Not everyone enrolling is ready to immediately adopt preventive behaviors
For several participants there was a delay between enrollment, knowledge acquisition, and RTC. As enthusiastic as they may have been to enroll and participate, Latinas in our study were at different levels of readiness for adopting one or more behaviors at baseline. Sixteen (43.2%) of the participants were eager to engage in preventive behaviors within 1 week of enrollment, while another 9 (24%) stated that they did not feel ready to start making changes until 2 to 4 weeks following enrollment. All others except one were either ready after 1 month or could not specify the timing of the delay. One participant finally expressed being RTC at the end of the program. Readiness also varied based on behavior sought: all expressed high baseline readiness to engage in physical activity, but this was not the case with eating habits. Figure 1 depicts baseline readiness levels for moderate physical activity, fruits and vegetables consumption, and sugar-sweetened beverages reduction.

Participants’ baseline readiness to engage in select preventive behaviors.
Theme 3: Factors associated with adoption of, and adherence to, preventive behaviors include family health concerns, better awareness of diabetes complications, and the presence of a strong social support
The factors most associated with the adoption of, and adherence to preventive behaviors, were health concerns (personal and familial) coupled with understanding that behavior modification would deter diabetes complications. Awareness of those complications provided a powerful incentive to adopt new behaviors, and presumably accelerated the transition to action.
As the program progressed, adoption of, and adherence to, new behaviors became largely attributed to social support within and outside of the program setting. Support from fellow participants was the most frequently stated source of social support for behavior adoption and retention: for several, other participants at more advanced levels of readiness became role models and provided the quality of social support to compensate for the lack of family support. Next was the support and engagement of a physician. Being told by the physician about one’s diagnosis was considered key to behavior change. Those referred by a physician credited the adoption of, and adherence to, healthy behaviors, to their physician’s recommendation and support, while several of the women not referred by physicians lamented their physicians’ limited time and guidance, and attributed the impact of a health care provider more to the quality of the patient-physician relationship. Promotoras and some family members were also credited for important social support and encouragement.
Theme 4: Most barriers to behavior modification were deemed nearly insurmountable
Even after participants acknowledged the strong impact of learning about diabetes complications, and while still expressing concern for family members, circumstances beyond their control seemed to create insurmountable hindrances to behavior modification, thereby threatening to tilt their “decisional balance” away from behavior modification. These barriers consisted mostly of external factors such as the built environment, and lack of childcare, financial resources and family support.
Family conflicts resulting from husbands or children resisting changes at home were a common complaint. Indeed, close to half of the participants reported resistance from spouses/partners. Weighing decisional balance factors was expressed as a dilemma: adopting and promoting preventive behaviors or resigning themselves to peace at home. Expressions used to describe their realities included “tug-of-war,” “divorce,” and “family units split.” Eventually, the family tensions resulting from adopting preventive behaviors led several participants to abandon their initial efforts.
Last, for most participants, healthy food was too costly and not readily available. Although our participants admitted to previously serving themselves large portions of food, and liking high-fat, calorie-dense foods—a preference they attributed to the Latino culture—several participants described positive changes they had made in their food choices (content and portion size) during the intervention. These changes were corroborated by the quantitative data. Still many expressed frustration at not being able to afford healthy food due to the cost. Making a choice to eat “healthy” would mean redirecting critical resources (money, time) previously allocated to supplying the family’s basic needs (such as gasoline for transportation) and running the risk of being judged. Lack of time, childcare and information to make practical decisions, in addition to environmental factors such as living conditions, lack of safe walkable areas and of reliable sources of transportation compounded the difficulties.
Discussion
To our knowledge, this is one of few studies to explore readiness among low-income, low educational level Latinas enrolled in a free DPP led by promotoras. While several factors identified in this study have previously been mentioned and published, our findings provide perspectives from a variety of sources.
According to our findings, Latinas of low-income and low educational level enrolling in prevention programs are highly motivated to adopt and maintain preventive behaviors when confronted with a negative personal or family health event and when referred by a trusted physician. They may not necessarily be ready to engage in one or more recommended behaviors on enrollment but, eventually, most adopt and at least temporarily retain recommended behaviors, especially in the presence of strong social support. However, the “cost” of diabetes prevention may become too high as adoption and retention of preventive behaviors threaten family dynamics, a price many of these women are unwilling to pay in exchange for future health gain.
Our results confirm the findings from others researchers showing an association between negative life events (such as the diagnosis of a medical condition) and an increased readiness to adopt healthy behaviors. 29 For health educators and healthcare providers this is an indication that positive blood glucose screening results, dramatic changes in Latinas’ health status and/or in the health of their family members should be viewed as a cue to refer them to prevention programs, since this may well be the best time for them to benefit from an intervention. Furthermore, because the health of family members is a high priority and motivator among Latinas, assessing key family relationships and engaging relatives should be explored at time of diagnosis. 7
While knowing the benefits of preventive behaviors may influence willingness to adopt a behavior in some, it is not sufficient.30,31 In one study, increased knowledge positively affected the behavior of Whites, but not that of Latinos. 32 In our study, specifically experiential knowledge of the devastating effects of diabetes on family and friends seemed a strong motivator to engage in preventive behaviors. Experiencing the seriousness of the disease, albeit vicariously, by hearing or seeing its effects on an acquaintance with diabetes seems to have helped intensify the process leading to “action”. It is as if exposure to (hearing about, or seeing) diabetes complications (blindness, kidney disease, and amputations) created a previously absent clear cause-to-effect mental association between behavior and complications. Elsewhere, emphasis on complications of certain behaviors has been shown to discourage unhealthy behaviors. 33 This strategy may be worth implementing more in this population.
It is clear that physician referral and engagement were instrumental in promoting program enrollment, motivating adherence to recommended behaviors and improving program retention. The role of clinicians has been a powerful motivator to action within and outside the Latino culture, with some reporting a 50% enrollment with physician referral compared to 10% without.32,34 For this reason, referrals, especially those targeting enrollment within 2 months would be ideal. 35 Ironically, the NDPP reports less referrals of monolingual Spanish-speaking Latinos compared with those who are English-speaking, 36 although a preference for “expert-driven” health guidance among monolingual Spanish patients has been reported. 37 However, according to our study participants, the quality of physician-patient connection determines the impact of physician referral. Trust and connection have been shown to affect success of lifestyle modification programs.38,39 Therefore, for best results, a positive connection between healthcare providers and Latinas seems essential. This may require a better matching of patient to healthcare providers as well as cultural-sensitivity training for providers assigned to Latino communities. Moreover, physicians labeling the patient’s condition (eg, “prediabetes, “high risk”) and offering a prescription may convey a sense of seriousness and urgency which is more likely to be interpreted as a “call to action,” and to help garner more family support.40-42
Healthcare providers and health educators cannot ignore the important dilemma—“decisional balance”—many Latinas face when weighing the impact of adopting preventive behaviors (avoidance of future harm) against the cost of sacrificing family stability/unity now. Some questions could help identify the extent of their dilemma at referral or on enrollment: “Is the patient’s support system (spouse, family, relatives, friends) on board?” If not, “is there an alternative support group available to her if she were to lose her family’s support?” “Are we (healthcare professionals, program directors or health educators) providing enough support and resources to mitigate the emotional and/or financial “burden” she may have to bear as she engages in preventive behaviors?” The answers to these questions may help determine the emotional “cost” she may incur if she enrolls in a prevention program and may suggest a different approach or the allocation of additional resources to increase the likelihood of success.
Social support has been shown to improve adoption of healthy behavior, independently of cultural background, but this is even more so in collectivistic cultures such as the Latino culture.37,43,44 In collectivism, group harmony and cooperation with group activities supersedes individual decisions. Along with collectivism is the Latino core value of familismo, which highly regards loyalty to family, including reciprocity with other family members, engaging in similar activities together, a strong dependence on family for material and emotional support, and often living in the same house. 45 Indeed, family support has been shown to be protective against diabetes among Latinos (not so among non-Hispanic Whites). 46 Another concept closely related with familismo is marianismo, which assumes the role of women to be that of caretakers willing to sacrifice for their families. Examples of practical application for the ideal wife and mother would be to eat the same food as her family and wait for her family before starting to eat. 47
Yet, our data show that more than half of the participants received little to no encouragement from family members for healthy eating, and more than two-thirds reported family and friends never or rarely engaging in physical activity with them.
This is where other sources of support seem to have been useful in closing the gap. Besides family members, fellow participants, community health workers, and physicians played an important role in the initiation and maintenance of newly acquired behaviors. According to our study, one of the most powerful determinants of readiness to adopt and maintain behavior was a strong social support network within the program, especially for those lacking support at home. Still, participants felt that enrollment of husbands and children in the same program could improve program success by reducing the resistance to changes at home, and increasing the critical support needed to sustain behavior modification. Thus, a parallel program for family members is worth considering if more success is desired.
Because community health workers share similar cultural background and circumstances, live in the same community as program participants, and have earned the trust of community members, they are more likely to be considered a reliable source of information. Participants tend to confide in them and share their emotional and health concerns without feeling intimidated, rushed, or rejected. This provides the promotoras a level of influence among Latinas that few other health professionals can attain. 48 At the same time, it is relatively easy for them to identify and connect well with these individuals. In fact, because of their special insights, the promotoras in our study were instrumental in assessing and relaying participants’ thought processes and challenges. This type of connection with their community is even more important because the women in our study are less likely to receive health information from a health care provider (many lack health insurance), and also less likely to receive information from the media (written or otherwise, including from a mobile device) due to their educational level and income. Instead they tend to listen more to family and trusted friends. 49 Program participants and promotoras’ statements confirmed findings that report a strong reliance among this population on family and trusted “friends” for health information and decisions.
Several studies on behavioral modification factors among Latinas have revealed barriers at individual, family and community levels.14,50-52 However most studies do not report participants’ current built environment, access to healthy food, transportation and neighborhood safety. 8 Among our participants, we found a high level of food insecurity, an independent factor associated with prediabetes.24,53 As a “food desert,” the intervention area has one of the highest proportions of fast-food restaurants to produce and grocery stores in California.54,55 Higher cost of healthy foods in “food deserts” and more access to fast foods in Latino neighborhoods have been reported elsewhere.56,57 Thus, the challenge of finding healthy food would be expected. Although a case could be made for the sale of certain foods in these neighborhoods based on cultural food preferences (applying the law of supply and demand), our study shows that when Latinas chose to eat healthy, their food choices were limited.
Regarding the built environment, the small cities where participants live have limited public transportation and—being that summer days can get extremely hot in this part of the country—it can be unsafe for individuals to engage in outdoor physical activity during most daylight hours. Lack of access to neighborhood safe spaces to walk is a risk factor for diabetes and an inverse correlation between neighborhood walkability and development of diabetes exists. 58 Safety is also a concern in this region where violence is a daily occurrence, reducing the opportunities for women to safely engage in outdoor physical activity.
It’s easy to understand how a sense of helplessness among individuals attempting to implement healthy behaviors can eventually give way to discouragement. 59 Unless the above-mentioned hindrances to behavior modification are reduced or eliminated, offering lifestyle prevention programs to these Latinas may be setting them up for failure. Of note, top barriers for our study participants differed from the most common barriers cited by Latino participants in the original DPP (who had higher income and educational levels), 14 an indication that suggests different living conditions /circumstances between the groups.
Several studies have compared the health of Mexican immigrants with that of other groups of immigrants in the United States: one study analyzing data from more than 34,000 immigrants from various countries and continents reported that Mexican immigrants tended to have a higher risk of diabetes and obesity compared with immigrants from Central America, the Caribbean Islands, and Asian countries. 60 Furthermore, a higher risk of diabetes has been associated with lower socioeconomic status. 61 Indeed a study among Latino immigrants in Northern California found that low-income Latino immigrants were more likely to experience diabetes. This phenomenon was attributed to lifestyle-related consequences of poverty. 62 Other studies mentioned residing in an obesogenic environment as a factor that increased even further the risk of diabetes among low-income individuals. 63
When considering immigrants living outside the United States, income and sociopolitical factors influence health outcomes: in countries with low social and political tolerance toward immigrants, these were more likely to experience worst health outcomes compared to natives and to immigrants living in less “exclusionist” countries. 64 In countries such as Sweden, where health care is universal, but immigrants earn less than Swedes, low-income and lower “occupational class” consistently increased the risk of disease within every immigrant group, independently of birth country. 65 Since our participants live in a county where 54% of the population is Latino, 66 social and political tolerance may or may not be factors influencing their health outcomes, but low-income status and employment type may play a role.
Thus, our findings have policy-making ramifications. While free DPPs are needed, several conditions must be met to ensure their relevance and success among low-income Latinas: increased access to trusted health care providers—Latinos having the highest uninsured rates, 67 incentives to health care providers prescribing prevention programs to Latinas and supporting their behavior, and year-round vetted programs for participants and family members. Increasing access to healthy food and to safe walkable areas, and providing efficient transportation in low income Latino neighborhoods should also be seriously considered. Investment in these policies has the most potential of dramatically changing outcomes and would go a long way, especially in view of the large potential health care savings for each year of delay in a person’s diabetes onset. 68 Figure 2 depicts behavior modification considerations among Latinas enrolled in a DPP.
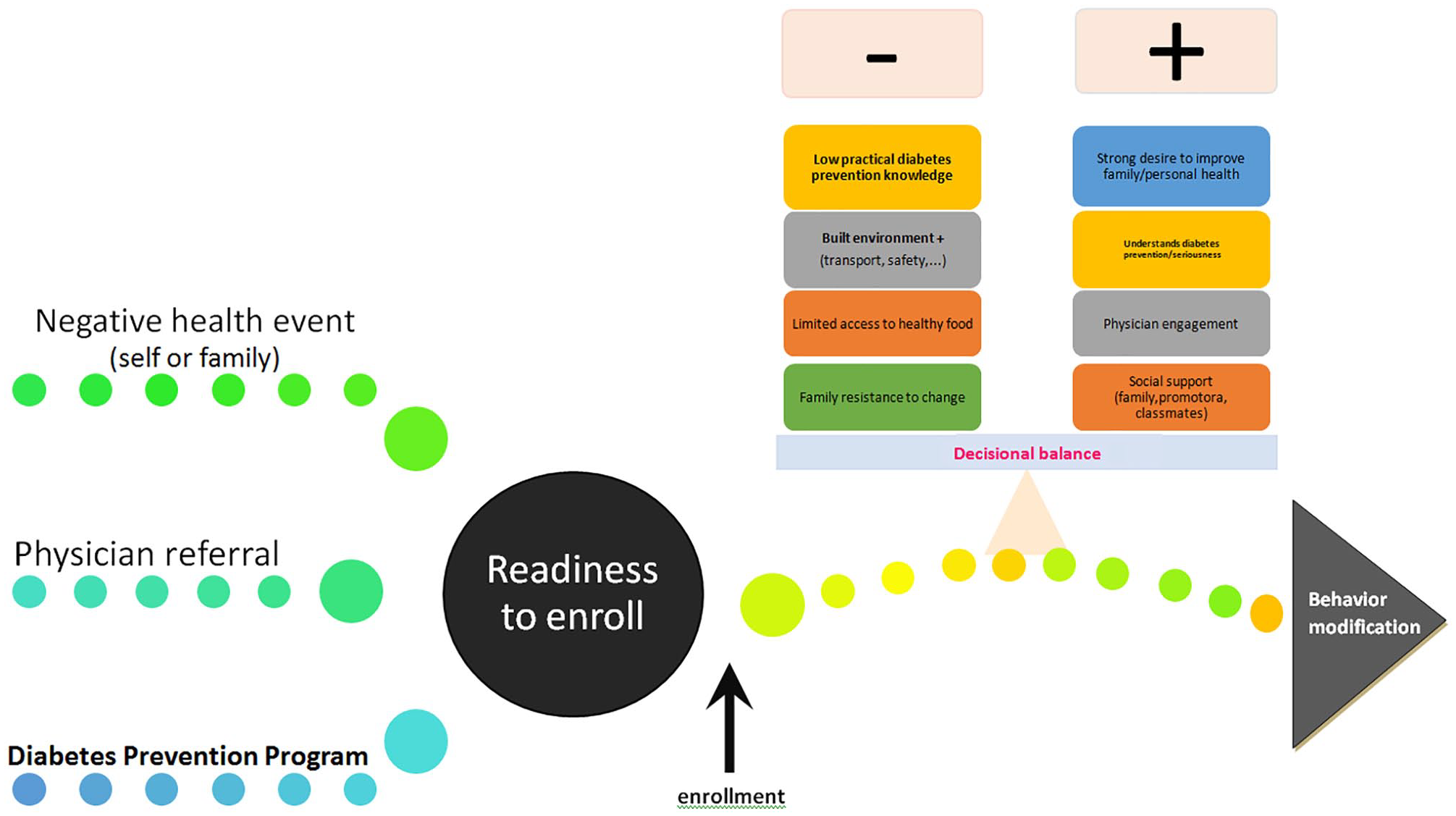
Behavior modification considerations among Latinas enrolled in a promotora-led diabetes prevention program.
Several limitations of our study need to be acknowledged. Our study group was composed of Latinas from Southern California, mostly of Mexican descent and the program was led by promotoras. Therefore, results cannot be generalized to other Latino subcultures and programs taught in other settings. Also—besides asking about language spoken at home—we did not fully assess acculturation neither did we enquire about household size, medical mistrust, or perceived discrimination. We had hoped to obtain “food recall measurements” to corroborate the qualitative data, but it was not possible due to the need to limit questions. However, we did ask one question to collect general information on food type and portion size, and participants freely shared changes they made in their eating pattern. Since interviews were conducted at the end of the program, there may also have been selection and memory biases.
One of the strengths of our study is that we were able to gather information from a variety of perspectives (several promotoras and FGDs) and were able to analyze results in context (timing, family-life, food availability, other life circumstances surrounding participants), something that is often lacking when program results are reported. Also, having some participants referred by a trusted Latino healthcare provider allowed us to assess the potential impact of collaboration between clinicians, promotoras and program development specialists. Last, our study sheds light on factors currently affecting low-income Latinas’ response to DPPs, a reality which may have been assumed of the past, especially after the implementation of the Affordable Care Act and the availability of the NDPP.
Conclusions and Implications for Practice
The emergence of DPPs throughout the country has provided options—including online alternatives—for low-income communities to learn about, and apply diabetes preventive behaviors. However, our study suggests that these programs will only accomplish their goal among populations that need it most within the scope of a multipronged approach, especially one that includes continuous program availability, informed healthcare providers, and the implementation of additional policy and research priorities.
First, year-long culturally tailored “family-style” programs should be offered to Latinos recently diagnosed with diabetes, fully engaging spouses and children in the process. It is important that these programs contextualize environmental factors, emphasize the connection between behavior modification and diabetes complications, and teach coping skills to help preserve family cohesiveness while the participants adopt the new healthier behaviors. Second, health care providers should be proactive and aim to refer at-risk Latino families once a diagnosis is established in one of the family members. They should also remain engaged and alert to possible family tensions resulting from attempts at behavior modification and strive to promote supportive policies. Thirdly, policies should reward healthcare providers prescribing prevention programs to Latinas, ensure insurance coverage for at-risk Latinas, and improve social determinants of health in these communities (safe parks, access to healthy foods, transportation, neighborhood safety, childcare, etc). Such concerted efforts may tilt Latinas’ “decisional balance” more favorably toward preventive behaviors, and thus increase the success rates of DPPs.
Last, it is not enough to report the results of DPPs. Research among Latinos should assess and report participants’ family dynamics, physician-patient rapport, and other social determinants of health, especially the built environment. This would create a consistent reference for replication and true program comparison between prevention programs. Replicating this study on a larger scale and in a variety of settings may also shed more light on factors associated with successful diabetes prevention among Latinas’ and help reduce the diabetes health disparities and mortality rates in the United States.
Supplemental Material
Supplement_#1.Overview_of_Vida_Vibrante_Intervention_-_revised – Supplemental material for A Qualitative Study on the Perspectives of Latinas Enrolled in a Diabetes Prevention Program: Is the Cost of Prevention Too High?
Supplemental material, Supplement_#1.Overview_of_Vida_Vibrante_Intervention_-_revised for A Qualitative Study on the Perspectives of Latinas Enrolled in a Diabetes Prevention Program: Is the Cost of Prevention Too High? by Maud Joachim-Célestin, Thelma Gamboa-Maldonado, Hildemar Dos Santos and Susanne B. Montgomery in Journal of Primary Care & Community Health
Supplemental Material
Supplement_#2._Focus_Group_Discussion_and_Key_Informant_Interview_guides – Supplemental material for A Qualitative Study on the Perspectives of Latinas Enrolled in a Diabetes Prevention Program: Is the Cost of Prevention Too High?
Supplemental material, Supplement_#2._Focus_Group_Discussion_and_Key_Informant_Interview_guides for A Qualitative Study on the Perspectives of Latinas Enrolled in a Diabetes Prevention Program: Is the Cost of Prevention Too High? by Maud Joachim-Célestin, Thelma Gamboa-Maldonado, Hildemar Dos Santos and Susanne B. Montgomery in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We are grateful to promotoras Vanessa Rivera, Miriam Valero, and Beatriz Castro for sharing their honest insights and – together with Monica Acevedo y Erika Marroquin – for going beyond the call of duty as they led the Vida Vibrante program.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was partially funded by the National Institute on Minority Health and Health Disparities of the National Institutes of Health under award number P20MD006988, Loma Linda University Behavioral Institute, and El Sol Neighborhood Educational Center. Thanks to Dr Toni Fernandez of Hesperia Clínica Médica Familiar (Hesperia, CA) for providing in-kind support to our research project.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.