
Abstract
Introduction
Pregnancy and the first 6 months postpartum (perinatal period) can be inherently challenging, often leading to lack of sleep, relationship tensions, and feelings of isolation. 1 These challenges result in the development of mood disorders for many women. For example, the prevalence of prenatal and postpartum depression is estimated at 12% and 17%, respectively.2-4 Exposure to environmental stressors, such as natural disasters, can amplify perinatal mood disorders and even have intergenerational impacts on child health and development outcomes.5-8
Health care providers are often the primary source of mental health resources and care for women during the perinatal period, 9 indicating a significant role of providers in helping to identify and manage (eg, treat/refer) perinatal mood disorders.10,11 However, a prior study found that maternal depression is assessed in primary care settings less than 50% of the time, and the use of screening tools is even lower (22%-46%). 12 National guidelines underscore the need for improvement in the detection and treatment of mood disorders in the perinatal period, particularly among those vulnerable to environmental stressors.10,11
Many studies have explored the impacts of disasters, or events that cause disruption exceeding the adjustment capacity of the affected community, 13 on mental health and have found that prenatal and postpartum women may experience significantly higher rates of mood disorders during disasters compared with the general population.14,15 In January 2020, the World Health Organization (WHO) declared the outbreak of a new coronavirus disease, COVID-19, to be a public health emergency of international concern. According to similar epidemics and pandemics, stress coupled with feelings of loneliness and anger can develop among people who are quarantined. 16 Additionally, social isolation during environmental disasters, such as COVID-19, may lead to decreased social connections, which can further exacerbate feelings of isolation and perinatal mood disorders. 17
Although current studies are exploring the specific impacts of COVID-19 on population mental health, 18 less is known about the mental health implications specifically related to perinatal mental health during COVID-19. Additionally, better understanding of potential factors that may be protective for perinatal women during a pandemic, such as social supports and/or coping strategies is warranted. 14 Resilience in the face of disasters is likely to result from a combination of resources that foster the ability to cope well despite extraordinarily severe demands. 19 The primary aim of this pilot study was to use mixed-methods to better understand mental health and well-being, as well as sources of resilience, for women in the perinatal period during the COVID-19 pandemic. These findings have implications related to prenatal and postpartum health care among women exposed to disasters and large-scale traumatic events.
Methods
Procedure
Ethical approval for this pilot study was obtained from the Colorado Multiple Institutional Review Board (#20-0840). Rolling recruitment for this study occurred between March and April 2020 using a purposive, nonprobabilistic sampling method. The targeted audience for this study included mothers who met the following criteria: (1) over the age of 18 years, (2) English-speaking, (3) currently living in Colorado, and (4) being pregnant or within the first 6-months postpartum. Women were recruited through advertisements posted on social media outlets (eg, Facebook, mom listservs). Women who met the eligibility criteria and who were interested in participating in the study completed an online consent form. Women were contacted by a member of the study team to schedule a time for a phone interview within 48 hours of completing the online consent form.
Data Collection
The study team used a simultaneous exploratory mixed-methods design to investigate the primary objective. 20
Qualitative Methods
Prior to the interview, participants were provided information about how the interview would be conducted. Two members of the research team conducted the phone interviews (first, CVF, and last author, JAL); interviews averaged 24 minutes, ranging from 17 to 43 minutes. The interview protocol consisted of a semistructured tool including a combination of open-ended questions related to sources of stress, sources of support and coping, self-care and well-being, beliefs around COVID risks, and impacts on care plans. Example questions included, “In general, how has the COVID-19 pandemic impacted your pregnancy experience thus far?” and “How has the pandemic changed your expectations around parenting?” Participants were provided mental health resources at the conclusion of interviews.
Qualitative Analysis
The 2 interviewers took extensive notes throughout the phone interviews. Qualitative data analysis followed best practice methods for qualitative research, including a deductive, theory-driven approach, and an inductive, data-driven approach.21,22 One of the interviewers (first author, CVF) coded the interviews using NVIVO software and constant comparison analysis. 23 The codebook contained a priori codes that aligned with sources of stress (eg, social isolation) and resilience (eg, social supports) from the literature. Inductive coding was also used to allow for discovery of unique sources of risk and resilience. A second coder (JAL) reviewed all transcripts, summarized themes and subthemes and compared findings with the first coder. If disconcordance on the meaning of the codes and themes were present, a discussion occurred between the coders to reach consensus on the coding structure.
Quantitative Methods
After completing the interview, participants were sent an electronic link to a 70-item online survey. The survey took approximately 15 minutes to complete. The survey included measures of sociodemographic factors, coping behaviors, and several validated measures for mental health and well-being, including: the Patient Health Questionnaire–2 (PHQ-2), which is a brief measure of depression with a range of 0 to 6 and a cutoff score of ≥3; 24 the Generalized Anxiety Disorder–7 (GAD-7) scale, which is a brief measure of anxiety with a range of 0 to 21 and a cutoff score of ≥10; 25 the Brief Resilience Scale (BRS), which measures resilience and ranges from 1 to 5 with higher scores indicating more resilience; 26 the Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS), which measures subjective well-being and ranges from 14 to 70 with higher scores indicating higher well-being; 27 and the 3-item Loneliness Scale, which measures loneliness and has a cutoff of ≥6 and a range of 3 to 9. 28 After completion of both the phone interview and online survey, participants were randomly selected to receive 1 of 2 USD50 gift cards.
Quantitative Analysis
Descriptive statistics were conducted to investigate the primary variables of interest in the quantitative data, including demographics, mental health and well-being measures and reported coping behaviors.
Results
Thirty-one interviews were conducted and 27 of the 31 participants completed the online survey. Approximately half of the interview participants were pregnant (52%) and half were within 6 months postpartum (48%). Fifty percent of the pregnant sample were primigravid and 38% of the postpartum sample had only one child. Table 1 displays sample characteristics of the participants who completed the survey and descriptives related to the primary variables of interest. Approximately 12% of the sample reported high depressive symptomology and 60% reported moderate or severe anxiety symptomatology. About two-thirds of the sample (68%) reported experiencing at least moderate stress, and participants scored an average of 46 on the well-being scale (range = 34-61) and an average of 3.0 on the resilience scale (range = 2.3-3.7). Forty percent of the sample reported being lonely. Participants reported that the most common ways they were coping included texting with friends (79%), video/phone calls with friends (68%) and sleeping (61%).
Sample Characteristics and Mental Health and Well-Being Variables Among Perinatal Women During COVID-19 (n = 27).
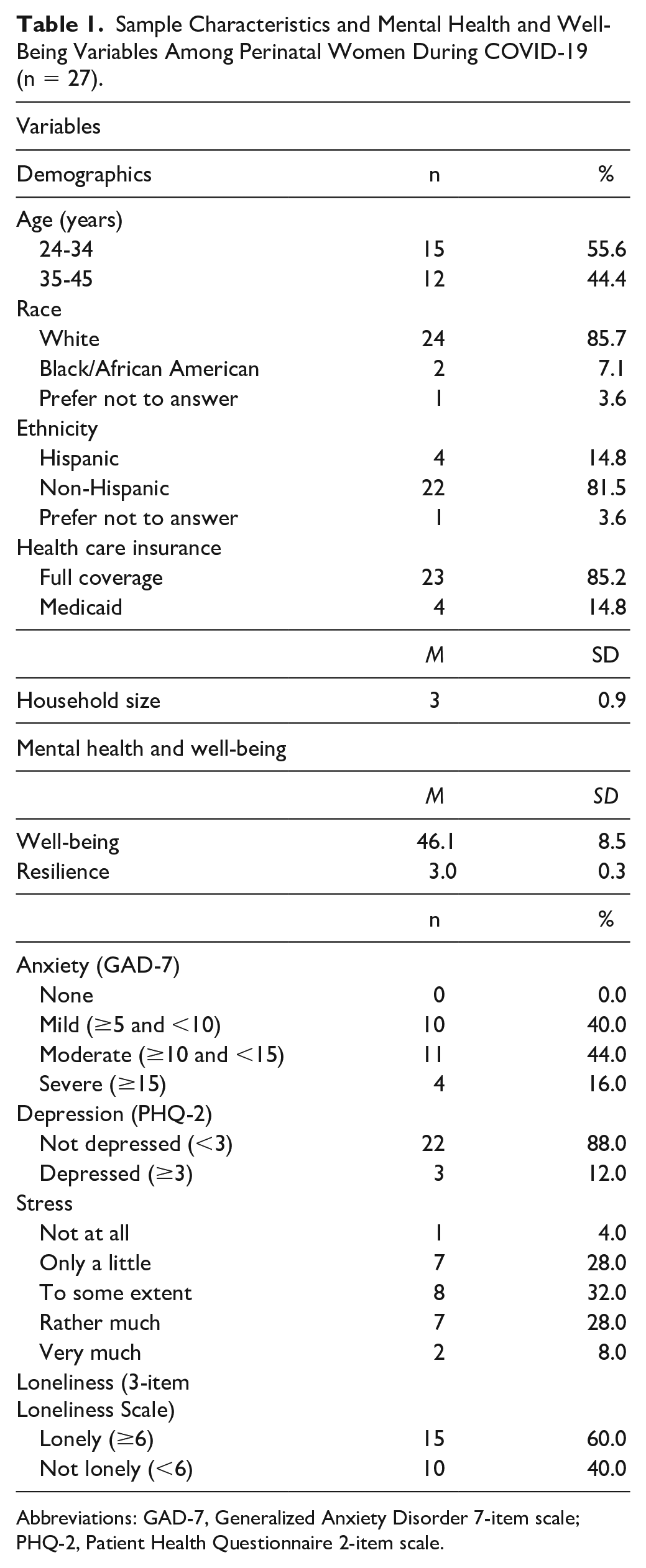
Abbreviations: GAD-7, Generalized Anxiety Disorder 7-item scale; PHQ-2, Patient Health Questionnaire 2-item scale.
The primary themes, subthemes, and illustrative quotes from the qualitative data are summarized in Table 2.
Themes, Subthemes, and Representative Quotes Related to the Impacts of COVID-19 on Perinatal Mental Health and Well-Being.
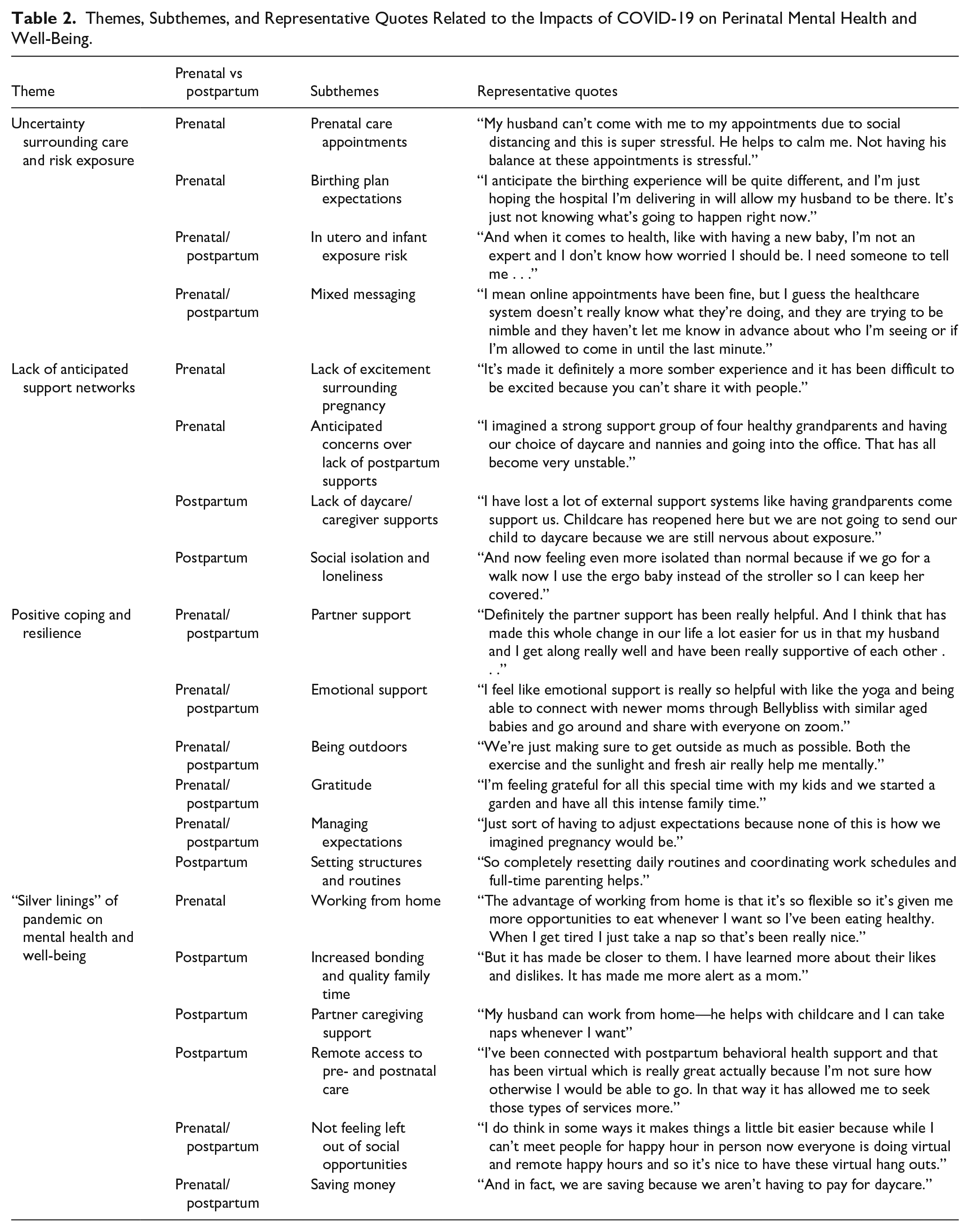
Theme 1: Uncertainty Surrounding Care and Risk Exposure
Pregnant women most commonly expressed stress surrounding “unknowns” related to prenatal care appointment rules, birth plan expectations, and prenatal exposure risk. For example, one woman shared, “I anticipate the birthing experience will be quite different, and I’m just hoping the hospital I’m delivering in will allow my husband to be there. It’s just not knowing what’s going to happen right now.” Among new mothers, uncertainty and stress were related to newborn risk exposure. One mother said, “and when it comes to health, like with having a new baby, I’m not an expert and I don’t know how worried I should be. I need someone to tell me . . .”
Lack of consistent messaging and clear guidance surrounding recommendations and care appointments from providers was a concern shared by both pregnant women and new mothers. One pregnant woman said, “I feel like we get all these mixed-messages about it.” Another pregnant woman said, “I mean online appointments have been fine, but I guess the healthcare system doesn’t really know what they’re doing, and they are trying to be nimble and they haven’t let me know in advance about who I’m seeing or if I’m allowed to come in until the last minute.”
Theme 2: Lack of Anticipated Support Networks and Loneliness
Pregnant women reported feelings of isolation and loneliness as well as lack of postpartum support networks. Women shared that being pregnant during COVID-19 resulted in less excitement surrounding the pregnancy because of social isolation. One woman said, “It’s made it definitely a more somber experience and it has been difficult to be excited because you can’t share it with people.” Pregnant women also talked about concerns over postpartum supports. One woman shared, “Well, we were counting on support from grandparents on both sides and we can’t anymore.”
New moms frequently cited stressors related to lack of daycare and caregiver supports, and social isolation. One mother said, “It has made it a lot harder, mainly that I don’t have childcare and I was planning on going back to work but now I can’t.” New moms shared that social isolation was significantly affecting their postpartum mental health. A mother said, “And now feeling even more isolated than normal because if we go for a walk now I use the ergobaby instead of the stroller so I can keep her covered.”
Theme 3: Factors That Support Positive Coping and Resilience
Pregnant women and new moms shared that partner support was the primary factor that helped them cope. One new mom shared, “we [partners] are alternating like some days he’s stressed and anxious and sometimes I will be. And we’re like we need to get through this together.” Emotional support was cited as the most helpful source of support among all mothers. One mom said, “being able to connect with newer moms with similar aged babies and go around and share with everyone on Zoom.”
All women shared that getting outdoors and being in nature was helping them cope. One pregnant woman said, “Just being outside. I always go to the park and just breathe.” Women also said that focusing on gratitude promoted their mental health. For example, one new mom said, “feeling grateful for all this special time with my kids and to have all this intense family time.” Finally, women in both the prenatal and postpartum periods shared that managing expectations was protective. One pregnant woman shared, “just sort of having to adjust expectations because none of this is how we imagined pregnancy would be.”
Among new mothers, structures and routines were cited as a factor that helped them cope. One mom said, “So completely resetting daily routines and coordinating work schedules and full-time parenting” and “staying on schedule has helped with staying mentally well too.”
Theme 4: Positive Impacts of COVID-19 Pandemic on Perinatal Mental Health and Well-Being
Participants shared a variety of positive impacts related to the COVID-19 pandemic. Pregnant woman said that being able to work from home allowed for more time to prioritize self-care, which improved their mental and physical health. New mothers highlighted numerous positive benefits including increased connection and bonding with their immediate family unit, partner supports in the home to share caregiving responsibilities, and increased access to remote postnatal and postpartum care. One mom said, “My husband is home full-time and that has been so helpful just to not be alone. I can really focus on her and my husband and our family time.” Another mother shared, I’ve been connected with postpartum behavioral health support and that has been virtual which is really great actually because I’m not sure how otherwise I would be able to go. In that way it has allowed me to seek those types of services more.
Both pregnant women and new mothers shared additional positive impacts of the COVID-19 pandemic including not missing out on social activities and spending less money. One mom said, “I think the biggest positive is that I didn’t have that feeling of missing out . . . my friends weren’t posting cool things that I was missing out on,” and a pregnant woman said, “We are spending less because we aren’t going out.”
Discussion
These findings highlight the additional toll of the COVID-19 pandemic on perinatal mental health in the United States. The quantitative findings suggest that the pandemic has resulted in elevated rates of mood disorders for this sample of pregnant and postpartum women. Perinatal anxiety rates were approximately six times higher in this sample compared to pre-pandemic perinatal rates in Colorado. 29 Additionally, participants reported lower well-being 30 and lower levels of resilience compared to pre-pandemic scores. 26 The qualitative component of this study illustrated sources of stress that further explain these quantitative findings. The burden of uncertainty related to health care services and risk exposure for all women was a salient theme. Harville et al 31 similarly found that after Hurricane Katrina, stressors experienced by perinatal women included the interruption of health care services, clinical infrastructure and referrals and the lack of knowledge surrounding early term exposure. Alternative studies found that uncertainties lead to heightened fears of contracting or transmitting infection 32 and fears surrounding separation from the infant at birth. 33
Almost half of the sample reported feeling lonely, and this social isolation may explain the high rates of anxiety and poor well-being and resilience reported in this sample of pregnant and postpartum women. 34 Social isolation was a common theme shared by both pregnant and postpartum women in the qualitative data and align with the prevalence of loneliness reported in the sample. Social distancing and isolation during disasters, coupled with lack of access to health care professionals, can lead to heightened intimate partner violence,35,36 which can affect maternal mood disorders and adverse pregnancy and birth outcomes. 37 Additionally, lack of caregiver social supports in the postpartum period are linked to poor maternal psychological well-being. 38
Sources of resilience were identified in these data and are supported by past research that has explored resilience among perinatal women during disasters. Virtual media platforms (texting, video calls),39,40 and engaging in self-care behaviors such as getting recommended sleep and exercise 41 were identified as protective coping behaviors in the quantitative data. Qualitative data suggested that social support, and specifically partner and emotional support, 42 gratitude and optimism,43,44 and the management or shifting of expectations 45 were significant protective factors for pregnant and postpartum women, particularly during exposure to significant environmental stressors. 42 However, the high rates of depression, anxiety, and stress identified in this sample suggest that quarantine and social isolation regulations may increase need for supports and protective coping behaviors. 32
Limitations of this pilot study include the small sample size, minimal diversity, lack of consideration of pregnancy and birth complications, and the recruitment strategy, which relied solely on social media platforms and may limit the generalizability of these findings. Additionally, approximately half of the pregnant sample were pregnant with their first baby and over a third of the postpartum sample were first-time moms. Mental health and associated factors may vary by primigravid and multigravida women.46-48 Larger studies are needed to increase generalizability and to compare the unique experiences of stress during COVID-19 among these 2 different groups. However, this study may have implications for health care providers who are providing care for pregnant and postpartum women during the COVID-19 pandemic. Table 3 displays provider recommendations to help mitigate perinatal mood disorders and promote resilience based on these preliminary findings. Examples include screening all perinatal women for depression and anxiety during healthcare visits and providing positive coping behavior recommendations via hand-outs during prenatal and postpartum care visits. Collectively, these data suggest that COVID-19 has amplified the rates of perinatal mood disorders among this sample of perinatal women.
Implications for Perinatal Health Care Supports to Promote Perinatal Mental Health and Well-Being During COVID-19 Pandemic.

Footnotes
Acknowledgements
We acknowledge all pregnant and postpartum women who participated in this study and shared their experiences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.