
Abstract
Introduction
Insufficient physical activity (PA) is a leading risk factor for obesity and related comorbidities, including type 2 diabetes, coronary heart disease, and stroke.1-3 Current guidelines for PA, defined as bodily movement that raises energy expenditure and enhances health, recommend 150 minutes of moderate PA or 75 minutes of vigorous PA, in addition to muscle strengthening activities, each week. 4 Yet currently, two-thirds of adults in the United States are insufficiently active. 5 Low-income adults and those without health insurance are least likely to adhere to PA guidelines. 6 Marked differences by socioeconomic status suggest continued efforts are needed to support PA among underserved populations.
Health care settings provide a unique opportunity to support and facilitate PA. Healthy People 2020 objectives recommend that health care professionals provide PA education to patients, particularly those with chronic disease, 7 because consultation and planning with a health care provider may increase PA. The American College of Sports Medicine encourages primary care physicians to include PA within an integrative treatment plan using an “Exercise Is Medicine” (EIM) framework. 8 Tenets of EIM include consideration of PA as a vital sign, measuring PA at every health care encounter, and then using this information to administer exercise “prescriptions” or referrals. 8 Exercise referral schemes generally involve patient referral by a health care provider to a tailored PA program, with initial assessment and ongoing monitoring and supervision. 9 Referral from the health care system may be directed to independent patient resources (eg, walking programs, mobile apps), internal resources (eg, physical therapy, wellness programs), or external networks (eg, community centers or gyms). 10 Heterogeneity in implementation and program components is common, and it is unclear based on the current body of literature whether independent, internal, or external referrals support sustained PA behavior changes.
The past 2 decades have seen a rapid expansion of exercise referral programs across the United Kingdom, 11 and in 2019, a multicountry European randomized controlled trial was designed to enhance exercise referral schemes with PA-related behavior change theory. 12 A large body of empirical and theoretical evidence supports the important role of theory and personal PA-related psychosocial factors. For example, the social cognitive theory (SCT) posits that learning occurs within a dynamic and reciprocal interaction of the individual, environment, and behavior. Individual psychosocial factors, such as self-efficacy (ie, confidence in ability to perform behavior) and use of self-regulation strategies (eg, goal setting and self-monitoring), are important correlates and determinates of PA behavior in many populations, suggesting that these factors may also mediate engagement with external resources like an exercise referral program.13-15 However, the role of PA-related psychosocial factors in exercise referral program utilization patterns is not well understood. Furthermore, as much of the research on exercise referral schemes has occurred in the United Kingdom, determinants of program engagement are unknown among underserved, low-income adults in the United States who are disproportionately affected by structural PA barriers and chronic disease risk. Understanding exercise referral uptake and sociodemographic and psychosocial determinants of utilization will offer evidence to guide implementation efforts among at-risk adults in safety-net clinics across the United States.
Thus, the purpose of this study was to assess an exercise referral program at a community health center. Specifically, we described patients who received a referral to the program, compared referred patients who did and did not utilize the program, assessed the association of patient characteristics and PA-related psychosocial factors with attendance rate among those who utilized the program, and evaluated follow-up PA behavior among those who utilized the program. We hypothesized that PA-related psychosocial factors would be positively associated with program attendance rate and follow-up PA.
Methods
Setting and Design
Our study was conducted at a large, multisite federally qualified health center (FQHC) in central Texas. The Heart of Texas Community Health Center has operated as an FQHC since 1999 and is closely aligned with the McLennan County Medical Education and Research Foundation Residency Program. The Center provides medical, dental, and behavioral health care for almost 60 000 unique patients, or approximately 1 in every 5 county residents, over 90% of whom live at or below 200% of the federal poverty guidelines. Approximately one-quarter (24%) of patients are non-Hispanic Black/African American, 43% are Hispanic/Latino, and 28% are non-Hispanic White. Approximately 1 in 6 patients do not have health insurance and are afforded care through a sliding scale discounted fee program that expands coverage to approximately one-quarter of self-pay patients. In 2018, 183,795 primary care clinical encounters were provided by 87 physicians (40 family physicians, 38 resident/fellow family physicians, 2 pediatricians, 3 internists, 4 obstetrician/gynecologists), 15 nurse practitioners, and 7 physician assistants.
To address limitations in accessible and affordable PA opportunities, the Community Health Center established the Wellness Center, an on-site, 6000-square foot exercise facility. The Wellness Center operates as an academic-practice partnership with support from multiple academic units of Baylor University. The primary goal of the Wellness Center is to support and facilitate PA opportunities among low-income patients and area residents as part of a community-centered health home approach to wellness and health equity. 16 Specifically, the Wellness Center was designed as a short-term transitional facility to build confidence and teach strategies to support patient PA; then, patients would “graduate” or transition to other gym or exercise facilities in the community to continue PA in multiple life spaces.
An observational design was used to enumerate and assess patients ≥18 years of age who received an exercise referral to the Wellness Center from their health care providers between October 1, 2017 and December 31, 2018. Study investigators observed the natural conditions of the program initiation and rollout; thus, the sample size of this study is also a reflection of the natural conditions within the health center. Health care providers were not given instructions or clinical criteria to restrict the eligibility of potential program participants. Patients with referrals were instructed to initiate an intake visit to meet one-on-one with a personal fitness advisor. Personal fitness advisors have, at a minimum, a 4-year degree in exercise physiology, CPR (cardiopulmonary resuscitation) certification, and first aid certification. The initial intake visit included an assessment of the patient’s functional capacity and a baseline survey. Subsequent visits included individualized fitness curriculum for exercise sessions, based on the patient’s medical conditions and goals. Participants were encouraged by fitness advisors to continue attending exercise sessions until the fitness advisor deemed the patient “independent” and able to exercise at the facility without supervision. Patients who initiated exercise at the Wellness Center were invited via telephone to participate in a follow-up survey from June 15 to July 15, 2019, even if they were no longer actively exercising at the Wellness Center. Baseline and follow-up survey responses were merged with electronic health records and Wellness Center attendance data to evaluate the Wellness Center program and participants. Participation in the follow-up survey was incentivized with $10 grocery store gift cards but no other incentives for program participation were provided. Procedures and protocols were submitted to the Baylor University Institutional Review Board in accordance with the ethical standards of the institution. This project was determined to not meet the definition of human subject research under the purview of the Institutional Review Board; however, informed consent to participate in the program surveys was obtained from all participants.
Measures
Patient sociodemographic and basic health characteristics were obtained from the electronic health record. Sex was defined as female or male. Race/ethnicity was defined as Hispanic or Latino, non-Hispanic White, non-Hispanic Black, or non-Hispanic other. Patient insurance status was described as private insurance, public insurance, nonprofit, or uninsured/self-pay. Private insurance included commercial options (Blue Cross Blue Shield, Humana, United, and Medicare Advantage), public insurance included Medicare (nonmanaged) and Medicaid, and nonprofit included a sliding-scale discount fee program. Body mass index (BMI) was calculated using weight in kilograms (kg) and height in meters (m) and categorized as underweight or normal (<25 kg/m2), overweight (≥25 and <30 kg/m2), or obese (≥30 kg/m2). Diabetes, hypertension, and coronary artery disease were dichotomous (yes/no) variables obtained from the health record.
Baseline and follow-up survey data included self-reported PA behavior and related theoretical constructs. Moderate and vigorous PA was measured using the International Physical Activity Questionnaire–Short Form (IPAQ-s). 17 Compared with accelerometry, the IPAQ-s has moderate validity (Spearman correlation coefficient = 0.30) and strong same day test-retest reliability (Spearman correlation coefficient = 0.76), and is recommended for regional, national, and international use. 17 We converted the self-reported responses to metabolic equivalents (METs) by assigning moderate activities a 4.0 MET value and vigorous activities a 8.0 MET value. 18 Participants were defined as having met PA guidelines if they reported at least 600 moderate-to-vigorous PA (MVPA) MET-minutes for the previous 7 days. 4
The Wellness Center was designed to build confidence for exercise and teach strategies to support physically active lifestyles. Accordingly, SCT was used as a framework to measure 2 PA-related psychosocial constructs: self-efficacy and self-regulation strategies.19,20 Self-efficacy for exercise was measured using a validated, six-item scale. 21 Participants indicated how confident they were, on a scale of 1 (not at all confident) to 5 (extremely confident), to do PA under different circumstances such as when being tired, in a bad mood, or having limited time. Responses were summed and summary scores could range from 6 to 30, with higher scores indicating higher self-efficacy. Self-regulation strategies for exercise behavior change were measured using a validated 15-item scale. 21 Participants rated the frequency of strategies or activities commonly used during behavior change, such as planning, keeping track of the behavior, or setting goals. Each item was rated on a scale of 1 (never) to 5 (many times over the past month). Responses were summed and summary scores could range from 15 to 75, with higher scores indicating more frequent use of self-regulation strategies. 21
Attendance data included the date of exercise referral, the date of the initial intake visit, and a count of the total number of visits to the Wellness Center. Date of initial intake visit less the date of exercise referral was used to calculate number of days from referral to initiation. The observation period was defined as the number of days between the date of exercise referral and the date of the follow-up survey.
Statistical Analysis
Statistical analyses were performed using SAS v9.4 (SAS Institute Inc). Statistical significance was 2-sided and defined at the α = .05 level. First, descriptive statistics, including frequencies, means, and proportions, were generated for all study variables in the total sample. Student t tests and chi-square statistics were used to compare patients with a referral who did and did not initiate a baseline visit to the Wellness Center. We determined the correlation of baseline PA behavior, PA-related self-efficacy, and PA-related self-regulation strategies among patients with a referral who initiated a baseline visit and completed a baseline survey. Next, bivariable and multivariable incident rate ratios for the relationship of patient characteristics and PA-related factors with number of Wellness Center visits were estimated using negative binomial regression (PROC GENMOD), given the overdispersion of the visit counts. Because the individual patient’s time between baseline and the follow-up survey could range from 6 to 21 months, the OFFSET option was used in the regression models to adjust for the varied observation (ie, “exposure”) period. Predicted probabilities from these models were output and used to graph predicted Wellness Center visits by baseline PA status and age. Finally, we evaluated the relationship of baseline characteristics and program participation with follow-up PA behavior. Generalized linear models were used to model the relationship of visits to the Wellness Center, time from referral to initiation, baseline PA, baseline self-efficacy, and baseline self-regulation with follow-up PA.
Results
From October 1, 2017 to December 31, 2018, 1136 patients ≥18 years received an exercise referral to the Wellness Center during a clinic visit to the community health center, as shown in Figure 1. On average, patients were 45.6 years (±14.0) and mostly female (78.8%). Approximately one-third (35.5%) were Hispanic/Latino and 42.5% were non-Hispanic Black. Almost all patients were overweight or obese and 39.6% had diagnosed diabetes. Approximately half (n = 543; 47.8%) of patients with a referral never initiated an intake visit with the Wellness Center and approximately half (n = 593; 52.2%) of patients with a referral initiated ≥1 visit. Compared to non-initiators, initiators were slightly older (46.9 vs 44.1 years; P = .001) but were otherwise similar in terms of sex, race/ethnicity, payor type, BMI, and chronic disease status (see Table 1).
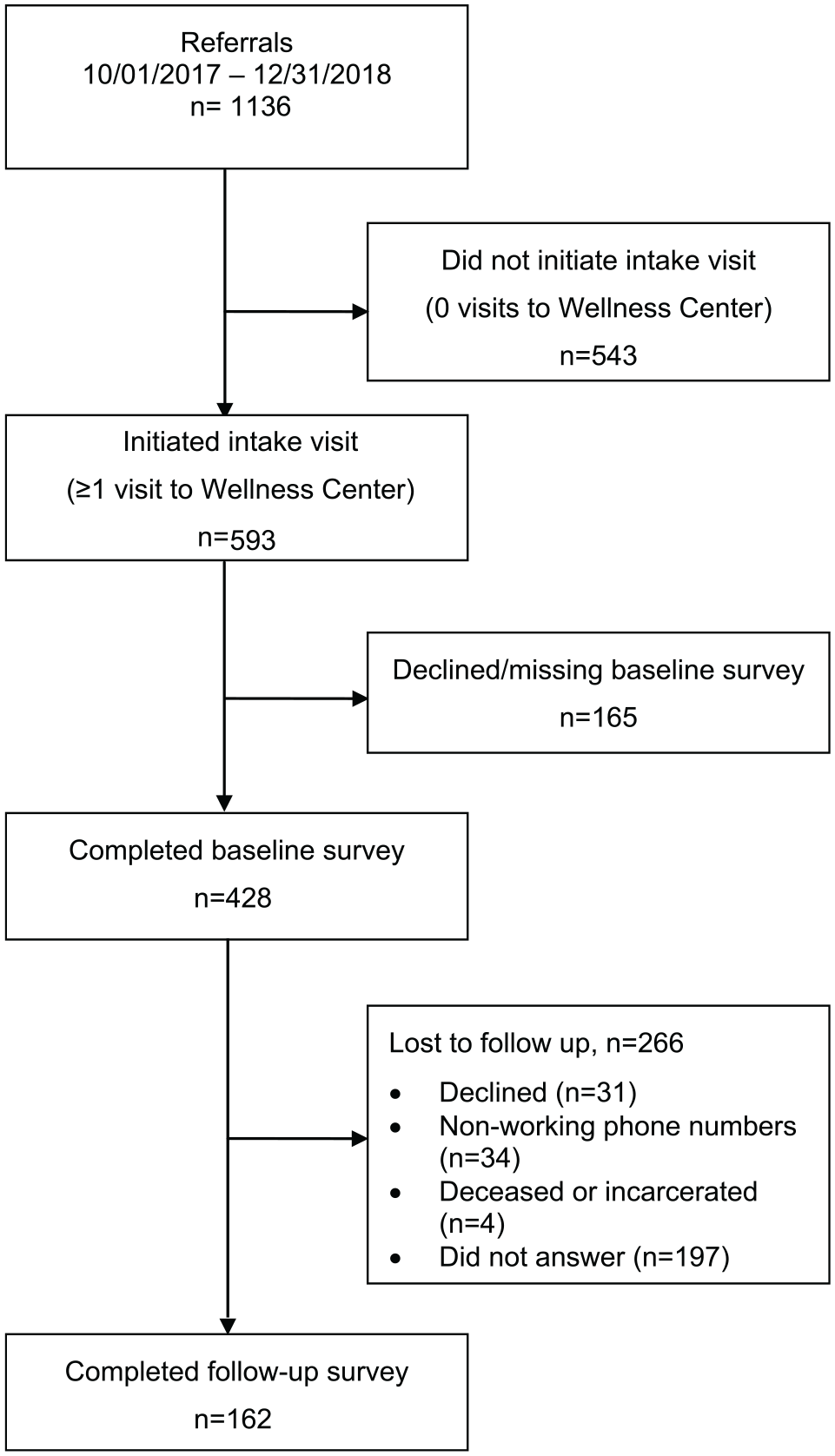
Enrollment in the exercise referral program.
Characteristics of Patients With a Wellness Center Referral, by Initiation Status.

Among patients who initiated a visit and completed a baseline survey (n = 428; 72.2% of patients who initiated ≥1 visit), the mean number of days between referral and initiation was 23.3 days (±43.1). During the observation period, total number of visits to the Wellness Center ranged from 1 to 136 (mean ± SD = 8.8 ±12.4 visits). At baseline, the mean MVPA MET-minutes per week was 247.6 (±677.1); approximately 12% of patients met current PA guidelines. A statistically significant correlation was observed between baseline MVPA, self-efficacy, and self-regulation, but not with number of days from referral to initiation (see Table 2).
Mean (SD) and Correlation of Baseline Physical Activity Behavior and Related Characteristics, n = 428. a
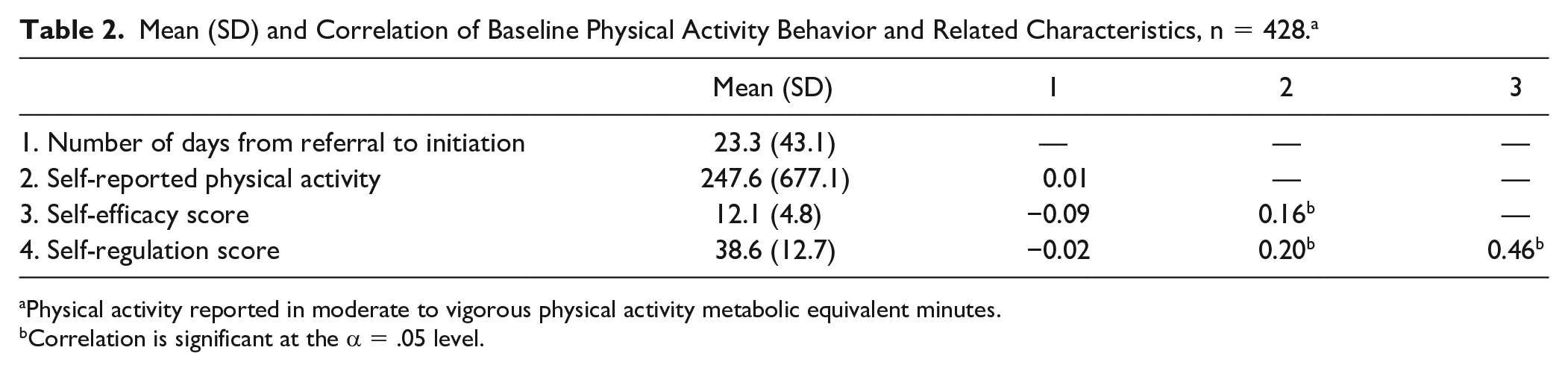
Physical activity reported in moderate to vigorous physical activity metabolic equivalent minutes.
Correlation is significant at the α = .05 level.
Table 3 shows the incident rate ratios (IRRs) for total number of Wellness Center visits, adjusted for individual observation times. There was a 1% increase in the incident rate of total Wellness Center visits for every 1-year increase in age (IRR = 1.01, 95% CI 1.00-1.02; P = .05), holding all other variables constant. In the unadjusted model, the incident rate of Wellness Center visits for patients meeting PA recommendations at baseline was significantly lower than the incident rate for patients not meeting PA recommendations (IRR = 0.72, 95% CI 0.53-0.97; P = .03). Other patient demographic factors (eg, sex, race/ethnicity, insurance status), health factors (eg, BMI, diabetes, hypertension), or PA-related theoretical factors (eg, self-efficacy, self-regulation) were not significantly associated with total Wellness Center visits. As shown in Figure 2, the Wellness Center visits increased with age and was higher, on average, for patients who did not meet PA recommendations at baseline.
Bivariable and Multivariable Incident Rate Ratios (IRRs) for Wellness Center Visits, n = 426. a

Bivariable models show the relationships between each independent variable and Wellness Center visits. Model 1 mutually adjusts for all independent variables with P < .20 in the bivariable models. Model 2 mutually adjusts for all independent variables.

Predicted value of Wellness Center visits by baseline physical activity (PA) status and age.
Among the subset of patients who initiated exercise at the Wellness Center, completed a baseline survey, and completed a follow-up survey (n = 162; 37.9% of the 428 patients with a baseline survey), the mean increase in MVPA MET-minutes was 380.3 (±1076.4; P < .001). Baseline PA-related factors were significantly associated with self-reported PA at follow-up. Baseline self-efficacy (b (SE) = 77.5 (21.6); P < .001) and self-regulation (b = 18.9 (8.8); P = .03) were positively associated with self-reported MVPA MET-minutes. Self-reported baseline PA was also significantly associated with self-reported follow-up PA. However, total visits to the Wellness Center and referral to initiation time were not associated with self-reported follow-up PA (see Table 4).
Association of Baseline Characteristics and Program Utilization With Self-Reported Physical Activity at Follow-up, n = 162.

Abbreviation: MET, metabolic equivalent.
Discussion
Overall, approximately half of patients at a FQHC engaged in ≥1 visit to an on-site exercise facility after receipt of a referral from their health care provider. Mid-life and older patients, and those who were less active at baseline, had higher Wellness Center utilization. Our finding that increasing age was positively associated with uptake of an exercise referral scheme is consistent with other work.22-24 Increasing PA among insufficiently active mid-life adults is a particularly important public health goal, because higher activity promotes maintenance of physical function and healthy aging trajectories throughout the life course. 25
Work from exercise referral programs within the UK National Health Service demonstrates that approximately one-third of patients with an exercise referral do not attend the first appointment of a structured 10- to 14-week program. 11 Of those, fewer than half adhere to the full 14-week program; adherence increases with age. 11 The shorter duration of UK exercise referral interventions is different from our program, where we observed patients for 6 to 21 months. Although we observed fewer initial attenders (approximately half vs approximately two-thirds) compared with the UK program, we observed similar adherence (defined by participation in our follow-up survey). Both shorter-duration, structured programs and longer-duration, unstructured programs appear to support PA for older adult females. Globally, lower-than-desired program uptake may be partially explained by the exercise paradox: that many people avoid exercise even though it is beneficial for health. 26 In the United States, most adults are insufficiently active and do not achieve the recommended weekly amount of aerobic and muscle-strengthening activity. 5 Furthermore, although exercise programs like the Wellness Center can ameliorate commonly cited barriers to PA such as lack of facilities or resources, other barriers to PA such as lack of childcare or work schedule conflicts may still remain.
To our knowledge, this is the largest investigation of exercise referrals to an on-site facility at a FQHC in the United States. In our study, more than three-fourths of patients who utilized the Wellness Center were Hispanic/Latino or non-Hispanic Black. The Wellness Center clinic system serves a low-income patient population, over 90% of whom live at or below 200% of the federal poverty guidelines. Because this study was an observation of natural conditions, patients who were referred to and used the Wellness Center were similar to the patients served by the clinic system as a whole, and we did not exclude patients from referral based on previous health conditions. Many communities served by FQHCs are exercise deserts—similar to food deserts with limited affordable healthy food options—because the built environment is characterized by limited walkability, green space, and/or affordable fitness facilities.27-29 Limited access to safe outdoor spaces or facilities, coupled with greater life demands, negatively influence PA in low-income populations.29-31 A particular focus on environmental facilitators is warranted in underserved populations, as adults who may benefit most are at high risk for inactivity and difficult to reach through health promotion activities. 32 For example, in 2 studies conducted in predominantly African American communities, researchers found that competing demands of time, the high cost of gym membership, and neighborhood safety were all barriers to PA.30,31 In our study, patients who did not meet PA recommendations at baseline had a higher rate of Wellness Center utilization than those meeting PA recommendations, suggesting that the Wellness Center may ameliorate some barriers to PA for those who are insufficiently active in this community.
As a theoretical basis for behavioral interventions, the SCT provides a framework through which PA initiation and maintenance can be understood. 19 Self-efficacy focuses on an individual’s perception of their ability or confidence to perform PA in a specific situation. Self-regulation focuses on skills that control PA behavior. Self-efficacy may predict exercise adoption, while self-regulation strategies may predict exercise adherence. 20 Previous work confirmed that self-regulation strategies mediate the relationship between self-efficacy and PA, 13 and that cognitive-behavioral interventions such as the promotion of self-regulation strategies are feasible and efficacious for PA maintenance.14,15 Understanding the role of these psychosocial constructs for an exercise referral program within a primary care setting will inform continued program development and identify factors that primary care physicians can target for behavior change interventions.
We observed a statistically significant increase in self-reported MVPA MET-minutes among patients who completed the follow-up survey, which may suggest a role for the exercise referral process in behavior change. Although we cannot establish causality, our findings are consistent with results from other exercise referral programs, predominately from the United Kingdom, that demonstrate small to moderate increases in PA.22,33,34 Notably, we also observed that self-efficacy and self-regulation strategies were significantly and positively associated with follow-up PA but were not associated with an increased rate of Wellness Center visits. We hypothesize that this could be due to a spillover effect, 35 such that patients who initiated exercise at the Wellness Center and had high self-efficacy and self-regulation were primed for PA in other life spaces and increased PA participation outside of visits to the Wellness Center. We also hypothesized that we would observe a shorter referral to initiation time for patients with higher self-efficacy and self-regulation strategy scores, and that this timing variable may be an indicator of program engagement. However, we did not observe an association between referral to initiation time with either PA-related psychosocial variables, Wellness Center visits, or with follow-up PA. We suspect that infrastructure barriers—now resolved—may have created delays for some patients during the initial program rollout that contributed to the 23-day mean time between referral and initiation. More work is needed to understand the referral to initiation time.
There are several limitations of our study. We may have unmeasured program components or confounders. We do not have access to data for patients who did not receive a referral to the Wellness Center so we cannot compare characteristics between those who did and did not receive a referral. Approximately half of patients did not initiate an initial visit to the Wellness Center, so we do not have baseline survey data—including PA-related psychosocial factors—for these patients. Selection bias may have occurred, such that patients who received a referral, initiated exercise, or completed the follow-up survey may have had higher self-efficacy and self-regulation than nonparticipating patients. Among patients with a baseline survey, 37.9% (162 out of 428) participated in a follow-up survey via telephone recruitment. While only 31 patients refused participation in the follow-up survey, most patients without follow-up surveys had inaccurate or out of service telephone numbers in their electronic health records despite protocol to update this information at every health care encounter. Although we achieved a lower response rate for the follow-up survey than we desired, national response rates for telephone surveys have plateaued at approximately 9%. 36 A supplemental analysis (results not shown) demonstrated that patients who participated in the follow-up survey were older and more likely to have diabetes and hypertension compared with patients who did not participate but were otherwise similar at baseline. Finally, self-reported PA data from the IPAQ-s questionnaire may be overestimated, so future work should consider device-based measurement for more objective PA data.
The purpose of this study was to assess the uptake and utilization of an exercise referral program in the primary care setting. This study demonstrated the feasibility of an exercise referral program using an on-site facility at a FQHC for an underserved patient population and demonstrated the role of self-efficacy and self-regulation in PA behavior among referral users. Notably, patients who were less physically active at baseline demonstrated higher Wellness Center utilization, suggesting that the program could serve as a conduit to PA engagement for a public health priority population. Community health centers have a unique opportunity to facilitate PA and health through exercise referral programs because the advice of a physician, coupled with increased access to health-promoting resources, can be an important component of patient behavior change. On-site exercise facilities and referral programs are one way that community health centers can enhance their support of patient health and community health equity by ameliorating persistent PA barriers in exercise deserts.
Footnotes
Author Contributions
K.R.Y. designed the evaluation, analyzed the data, and wrote the manuscript. W.C., M.G., G.B., M.R.U.M., B.N., and J.O.G. provided logistical support for data collection, helped with data interpretation, and edited and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: K.R.Y. is supported by the National Institute on Aging of the National Institutes of Health under Award Number K01AG058754. The Wellness Center operations are supported, in part, by the Episcopal Health Foundation. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies. The study sponsors had no role in study design; collection, analysis, and interpretation of data; writing the report; nor the decision to submit the report for publication.