
Abstract
Keywords
Introduction
According to the Centers for Disease Control and Prevention (CDC), the number of adults with opioid use disorder (OUD) has increased from 1.0 per 100 000 adults in 1999 to 4.4 per 100 000 in 2016. 1 OUD and drug overdose are escalating in the United States and the opioid epidemic continues to claim lives. Since 1999, the number of opioid related deaths increased nearly six fold and at an estimated cost of $78.5 billion per year. 2 While medication-assisted treatment (MAT) is available for OUD, few receive treatment in primary care underutilizing a setting ideal for privacy and comprehensive care.3-5 Implementing an office-based opioid treatment (OBOT) requires organizational transformation to meet the needs of patients, providers and learners. Addiction illness is becoming an integral component of chronic disease management in primary care where patients already have a trusting relationship with a provider. 6
MAT education and training in primary care can successfully position residents to gain experience and obtain a waiver to prescribe buprenorphine after graduation.6,7 Models for implementing OBOT indicate that several platforms exist to deliver care. Key components needed for an OBOT include pharmacotherapy, education, an integrated care model, psychosocial services, and criteria for effectiveness, innovation, and addressing special populations. 8 Substantive education of all providers and staff may facilitate a culture shift to recognize and treat OUD as a chronic disease.
Our focus is to reduce the barrier of providers’ limited time available to discuss opiate use with patients and provide training to improve the likelihood of referring a patient for evaluation and/or MAT. We discuss necessary steps to build an OBOT infrastructure in primary care to transform practice. The pivotal relevance to practice includes application of strategies to reduce the number of patients taking chronic opioids (with and without benzodiazepines) by initiating MAT with buprenorphine. This process is transferrable to primary care sites.
Setting
The setting includes an outpatient practice consisting of four-modules (10 exam rooms per module) and serving approximately 22 500 unique patients annually. The embedded MAT is within a busy primary care practice with integrated behavioral health providers (BHPs). The clinic is a level 3 National Committee for Quality Assurance (NCQA) Recognized Patient Centered Medical Home. The practice MAT team includes physicians, pharmacists, licensed clinical addiction specialists (LCAS), office staff, coordinator, and nurses.
Participants
Participants included residents and primary care providers.
Program Description
Objectives
Our goal is to describe a comprehensive, outpatient MAT clinic implementation. The first important step is to use the electronic health record (EHR) system to identify patients with risk factors, including a history of overdose or substance use disorder (SUD), opioid dosages ≥50 morphine milligram equivalents (MME) per day, or the concurrent use of benzodiazepine (Table 1). It is also useful to gather and share the prescription data from the EHR with providers to demonstrate prescribing practices and to help identify risky prescribing practices. 9 For residency programs, prescription data of prescribing under a supervising physician is also useful to review.
MAT Clinic Implementation Processes.
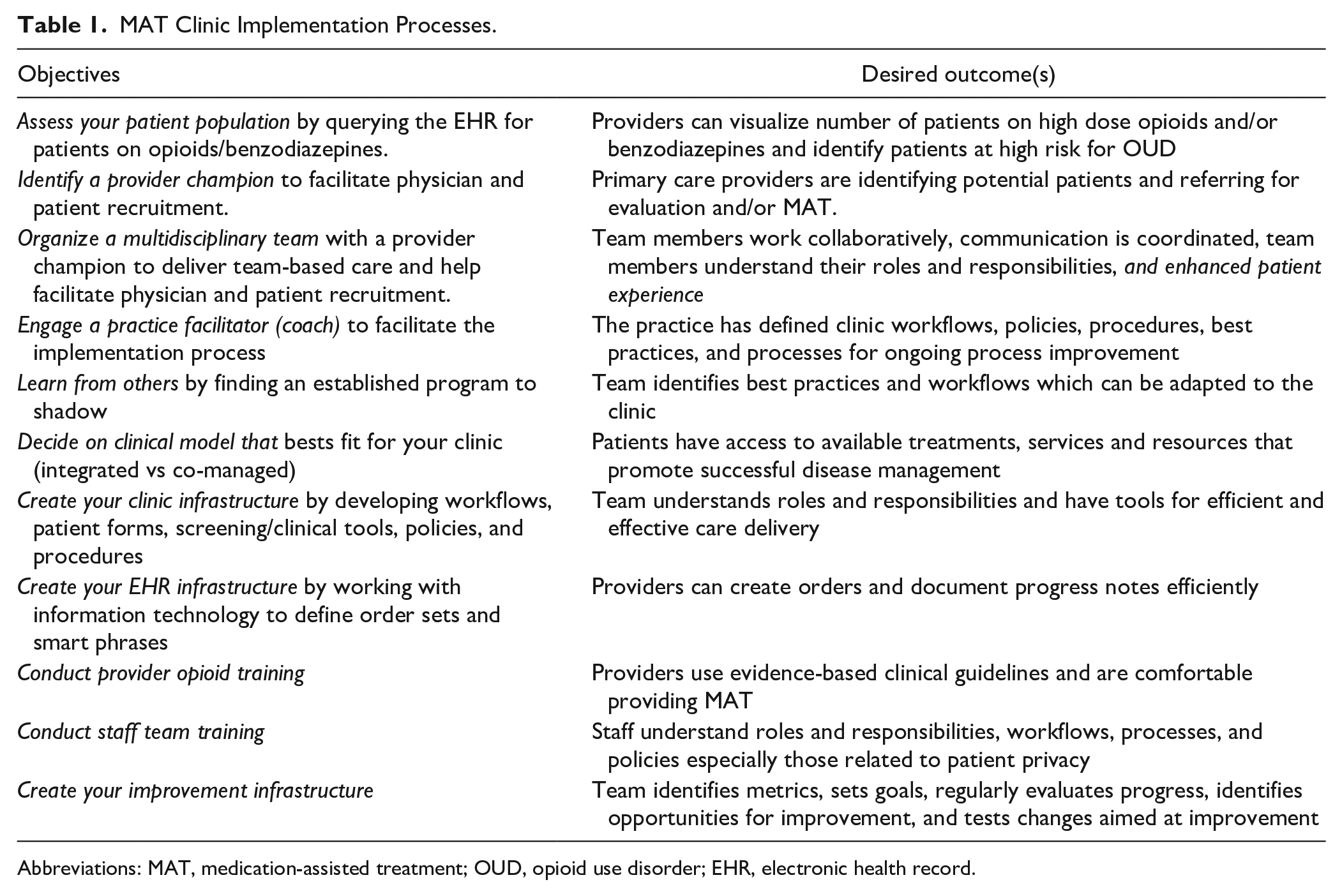
Abbreviations: MAT, medication-assisted treatment; OUD, opioid use disorder; EHR, electronic health record.
Multidisciplinary Team
It is essential to organize a multidisciplinary team that includes a project coordinator, a provider, a staff member and a clinic champion at the very least. 10 A practice facilitation coach can serve as resource for clinic flow design and support best practices adoption. 11 Evaluating the implementation, ongoing processes and metrics is essential to bringing necessary items for discussion and identifying opportunities for improvement. Programs should evaluate and solicit feedback from the team, providers, staff, and patients.
Existing Programs
Provider training for MAT can be done at no charge through the Provider Clinical Support System. 12 Observing an established program is imperative for success as viewing a clinic workflow on site can add clarity to the processes such as rooming patients, obtaining urine drug screens (UDS) and patient scheduling.
Patient Forms
A patient agreement is useful to establish commitment and expectations. Many institutions have established agreements that adhere to institutional criteria and formatting. A form for monitoring patient withdrawal symptoms is necessary such as the Subjective Opiate Withdrawal Scale. 13 Another form to consider is a checklist of team member tasks to help with organizing necessary steps for MAT.
MAT Pool in EHR
Creating a MAT provider pool in the EHR to refer patients for evaluation is an efficient process. In our clinic, this avenue is most common for established patients, but many new patients seeking primary care and MAT are also routed through the referral pool for assessment. This allows the clinical coordinator and pharmacist to review eligibility and patient history prior to the MAT initial appointment.
Lab Testing
Understanding the available UDS in a practice is necessary in choosing the standing lab orders for MAT patients. In the standard UDS at our facility, the opiate test shows that the urine is negative even if patients are positive for buprenorphine. We identified the appropriate UDS order that tested for buprenorphine, as well as a lab order that we ultimately decided to use, which is a full qualitative screening. This included opiate medications and their metabolites, amphetamines, barbiturates, benzodiazepines, cocaine and its metabolites, tetrahydrocannabinol and methadone, in addition to a quantitative reflex screening on opiate and benzodiazepine metabolites. A separate test is required to test for fentanyl in urine. Dip urine drug tests are ideal, but not available in our facility.
EHR Order Sets
It is essential to connect with an information technology specialist within the institution to create order sets to use throughout the health care system. Order sets designed for MAT induction, stabilization, and maintenance cover all of the phases for treatment. Consideration for lab tests needed for routine orders (such as urine pregnancy test) or those that will need periodic testing can be part of the order sets.
Staff Training
Staff training is an essential component for any successful MAT program. We recommend finding a system that offers on-site training of staff. Training for how to appropriately arrive and check out MAT patients is essential. The use of nonjudgmental language is especially important.
Screening
The use of a screening tool, such as the drug abuse-screening test (DAST-10), is needed to assess a patient’s level of SUD quantitatively along with measuring drug involvement and problems associated with the drugs. 14 Providers or BHPs may use the DAST-10 (at our site this is located in all outpatient exam room drawers) to screen patients. Patients are eligible for screening if they are currently prescribed opioids or benzodiazepines and/or when the medical provider or BHP has concern for opioid use or misuse (on either prescribed, diverted, or illicit opioids/opiates). For moderate (3-5) or severe (6-10) DAST-10 scores, providers and BHPs work together to complete assessment and provide counsel. This may involve a warm handoff to the BHP to augment medical provider’s assessment, or in the case of the BHP patient identification, a looping in of the provider to assist with MAT assessment and referral process. At the point that MAT-specific treatment begins, only a BHP who is an LCAS provides the requisite specialized MAT counseling. If a practice does not have BHPs on site, referral of patients to community resource is an option.
Patient Identification
Our “Patient Identification Workflow” (Figure 1) involves both provider and BHP identification and triage of MAT patients. Utilizing an integrated care model, BHPs can provide coverage for the outpatient primary care practice during clinic hours and/or when a provider identifies a patient who may benefit from MAT. One option for patient referral is through a warm handoff (process by which a medical provider introduces a patient to a BHP at point of care). After this handoff, the BHP conducts an encounter with the patient to assess for MAT, followed by debrief and development of treatment plan with the MAT team.
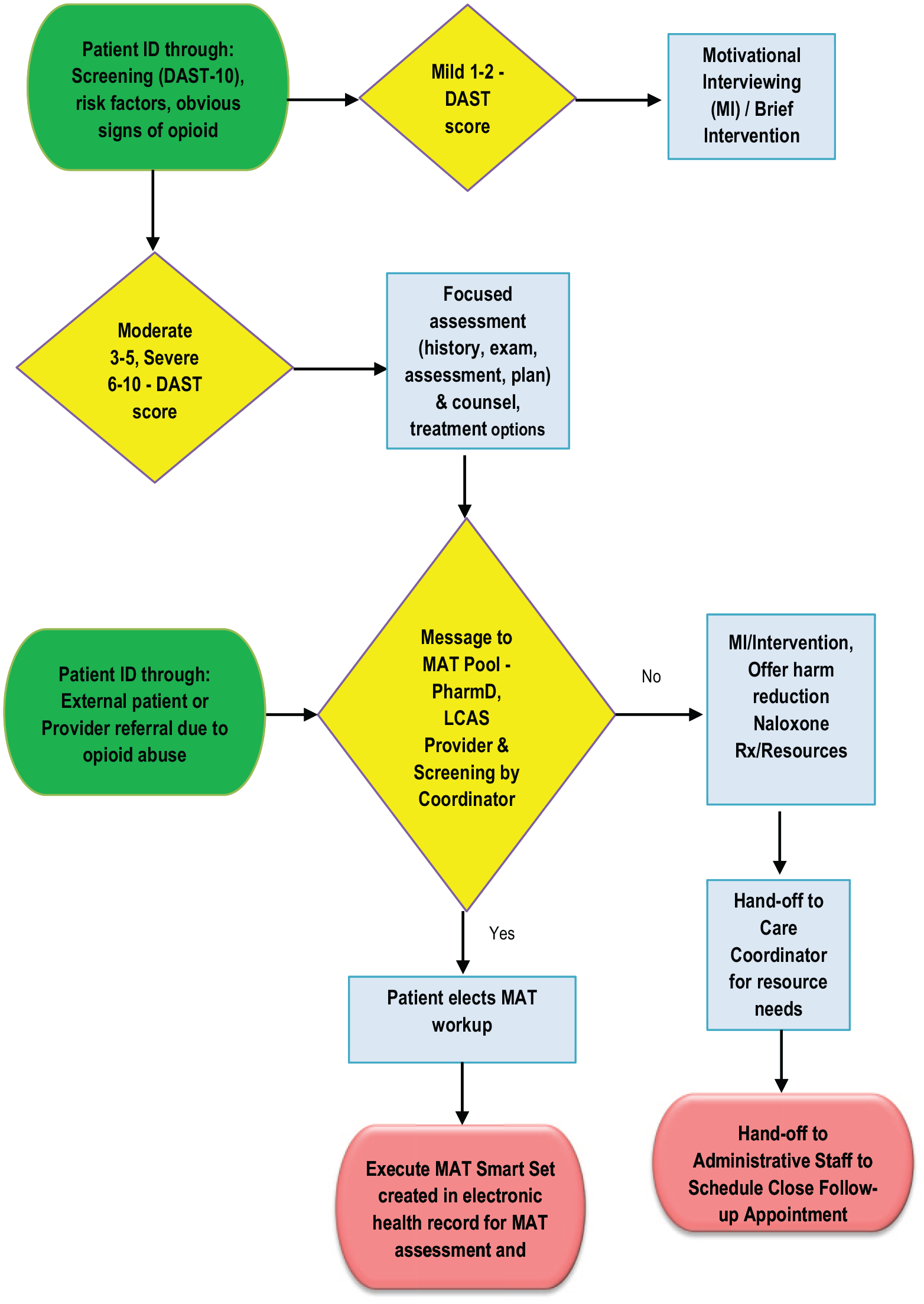
Sample patient identification workflow for medication-assisted treatment (MAT) provider.
Program Evaluation
For our MAT program, we started with the viewpoints of the providers. Using a survey, faculty and residents responded with brief feedback regarding comfort level in 3 domains. During 6-month follow-up from starting the MAT clinic, 36 out of 52 providers (residents and faculty) answered several brief questions to determine comfort level and practice patterns with opioids in high-risk patients. Seventy-two percent of respondents reported participating in MAT training. When asked about ordering urine drug screens in patients taking opioids and/or benzodiazepine medications, 78% indicated they participated in this practice. Sixty-nine percent of providers indicated they perform screening for high-risk opioid use. Only 8% of providers reported conducting crucial conversations about risky opioid use with patients and MAT options. The majority (88%) reported they would refer their patient to MAT clinic for evaluation and/or treatment.
Outcomes
At 6 months of MAT implementation, we have enrolled 15 patients. There are 2 chronic pain patients with one totally off all narcotic medications and one is stable on low-dose Suboxone and no other pain medications. The remaining patients have misused a variety of prescription and nonprescription medications, including heroin, benzodiazepines, stimulants, fentanyl, tramadol, and opioid derivatives.
Discussion
The MAT patients are coming in at least weekly to start and with the expectation to discontinue the use of opioids and illegal drugs. Most are stable on Suboxone. Primary care providers are in a strategic position to assess patients for MAT. Screening patients and conducting difficult conversations with patients about addiction and therapy is necessary in any successful OBOT. 15 Our providers noted the need for more education regarding opioid prescribing and lack of time to have necessary conversations with patients. These barriers exist in the literature along with lack of referral options, limited information regarding diagnostic workup and ancillary support of physicians. 16 One way to address these barriers is by training, which is slowly becoming more common during residency training. One study of US residency programs (internal medicine, family medicine, and psychiatry) reported 476/962 (49.5%) manage patients with OUD but only 23.5% have a curriculum during residency for OBOT. 17 In our program, we have noticed an increased enthusiasm for more education around MAT and OUD, presentations at scientific meetings by residents and requests for elective rotations. We have also seen a boost in residency applicants who ask about MAT training during the interview process.
Several programs have had success with implementing MAT within a primary care setting.16,17 The components of a program for opioid addiction treatment should include preparing the office and clinical team. Some advocate a practice champion who has waiver training with the intent to train others. 17 At our practice site, we had an experienced waiver trained physician, residency director and pharmacist who embraced the process of implementing an OBOT and also became MAT trainers so that second year residents will receive MAT waiver training as part of their curriculum. Our intention is to make MAT part of our residency training and to have the resident obtain waiver at the same time of the DEA license.
Although warm handoffs are an enrollment process, many providers refer patients to MAT after they have left our clinic from an appointment. Frequently, referral of patients is from other departments, outside practices or by patient self-referral, particularly from word of mouth and by online resources. These patients go through the same process as internal referrals, but additionally are required to become a patient of our clinic establishing with a primary care provider in order to receive continuity of care. Patients referred to MAT by one of our providers through the EHR pool undergo a telephone screen with scheduling for an MAT appointment where an LCAS and prescribing provider see the patient in tandem. The team then discusses the patient’s appropriateness for the program and develops a treatment plan for the patient.
Implementing MAT into primary care practice enhances access to treatment for patients with OUD or opioid dependence, while reducing barriers of limited time and experience of primary care providers as well as providing training opportunities and exposure for residents. Developing an invested MAT team, educating faculty, residents, and staff, and establishing adaptable workflows is essential in the successful implementation of any MAT program. Primary care MAT is an integral component in filling the gap of addiction illness management.
Footnotes
Acknowledgements
We would like to thank Rosalinda Bennett Thomas, MEd., LCAS; Linda Perkins McRae, PsyD, LCSW, LCAS; and Katherine Moore, PharmD, who are instrumental in guiding and counseling our patients. We also would like to acknowledge Gail S. Marion, PA, PhD, who supported this process with her leadership to integrate our clinic.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Primary Care Training and Enhancement grant through Health Resources and Services Administration (HRSA) Grant TOBHP28568.