
Abstract
Introduction
Unhealthy lifestyle has led to an escalating number of people affected by noncommunicable diseases (NCD) such as the metabolic syndrome (MetS).1,2 The NCD burden is rapidly increasing worldwide, contributing to approximately 41 million deaths (71%) of the 56 million total reported deaths annually. 1 Of these, 17.9 million deaths were caused by cardiovascular diseases (CVD). 1 MetS is a condition that describes the clustering of CVD risk factors, namely, obesity, diabetes, hypertension, and dyslipidemia. 2 In Malaysia, the prevalence of MetS was 43.3% as defined by the Joint Interim Statement (JIS) definition. 3 The growing prevalence of obesity and sedentary lifestyle contributes to the high prevalence of MetS. 2 This has caused a huge strain to the primary health care system as the majority of patients with MetS are being managed in primary care. 4
The concept of self-management support leading to an “informed, activated patient” to improve outcomes for chronic conditions was first proposed by the chronic care model.5,6 Activated patients who are prepared to take on a key role as a collaborative partner in managing their health is a critical element needed for the successful implementation of this model. However, the inability to measure activation has been a limiting factor in its implementation. Therefore, Hibbard et al 7 later introduced the term “patient activation,” which is defined as “the state in which an individual possesses the knowledge, skills, and confidence to take independent actions to manage their health and care.” They conceptualized patient activation on a continuum in which patients can be categorized by their levels of activation. 7 The same group of researchers has also proven that positive change in activation level is related to positive change in a variety of self-management behaviors. 8 Therefore, individuals with MetS need to be empowered with knowledge, skills, and confidence to increase their activation level and subsequently improve their self-management behaviors. Patient activation has also been shown to improve quality of life and health outcomes; and reduce the utilization of health care services and costs.9-11
Several tools to measure patient activation and empowerment have been developed by various researchers. 12 These include the Patient Activation Measure® (PAM®),7,13,14 Patient Empowerment in Long-Term Conditions, 15 Patient Enablement Instrument (PEI), 16 and Self-Efficacy in Long-Term Conditions. 17 Various tools have also been developed to specifically measure self-management behaviors especially for patients with diabetes. 18 These tools are not suitable to be used in individuals with MetS as there is a subset of patients with MetS who do not have diabetes. Therefore, measuring specific self-management behaviors is beyond the scope of this study. The PAM® was chosen for this study because it covers the measurement of knowledge, skills, and confidence to carry out general self-management behaviors suitable for various chronic conditions including MetS. It was originally developed by Hibbard et al 7 as a 22-item questionnaire in the English language using the Rasch model. It identifies 4 domains of patient activation (knowledge, skills, confidence, and behaviors) and suggests 4 levels of activation that patients reach to become fully engaged in managing their own health.7,13 The PAM® 13-item short version (PAM®-13) was subsequently developed and it was proven to have similar psychometric properties as the 22-item. 13 The PAM®-13 was chosen for this study as it has the optimum number of items with good validity and reliability to measure patient activation and empowerment. 13 It has also been widely translated and validated into various languages, including the Malay language.19-26 The PAM®-13 Malay version is valid and reliable with a Cronbach’s α value of 0.79 (Bahrom NH, et al, unpublished data). It is also fairly stable over time with an overall intraclass correlation coefficient value of 0.45 and ranged from 0.26 to 0.59 (Bahrom NH, et al, unpublished data).
Many studies have explored the factors associated with varying levels of activation in self-management of various chronic conditions.27-29 Factors that have been shown to be associated with low activation level include having low education, low socioeconomic status, high body mass index (BMI), and poor self-reported health status. 27 Whereas, high activation level has been associated with higher education background, better self-rated health status and having adequate health literacy. 30 However, there is a gap in the literature regarding the level of activation and the factors associated with it among patients with multiple CVD risk factors such as MetS. This evidence is also severely lacking in the Malaysian primary care setting. Therefore, the objectives of this study were to determine the levels of activation and the factors associated with high activation level among patients with MetS in the Malaysian primary care setting.
Methods
Study Design and Population
We conducted a cross-sectional study among patients with MetS attending a university primary care clinic in Selangor, Malaysia. The conduct of the study is outlined in the flowchart presented in Figure 1. Patients were selected according to the inclusion and exclusion criteria.
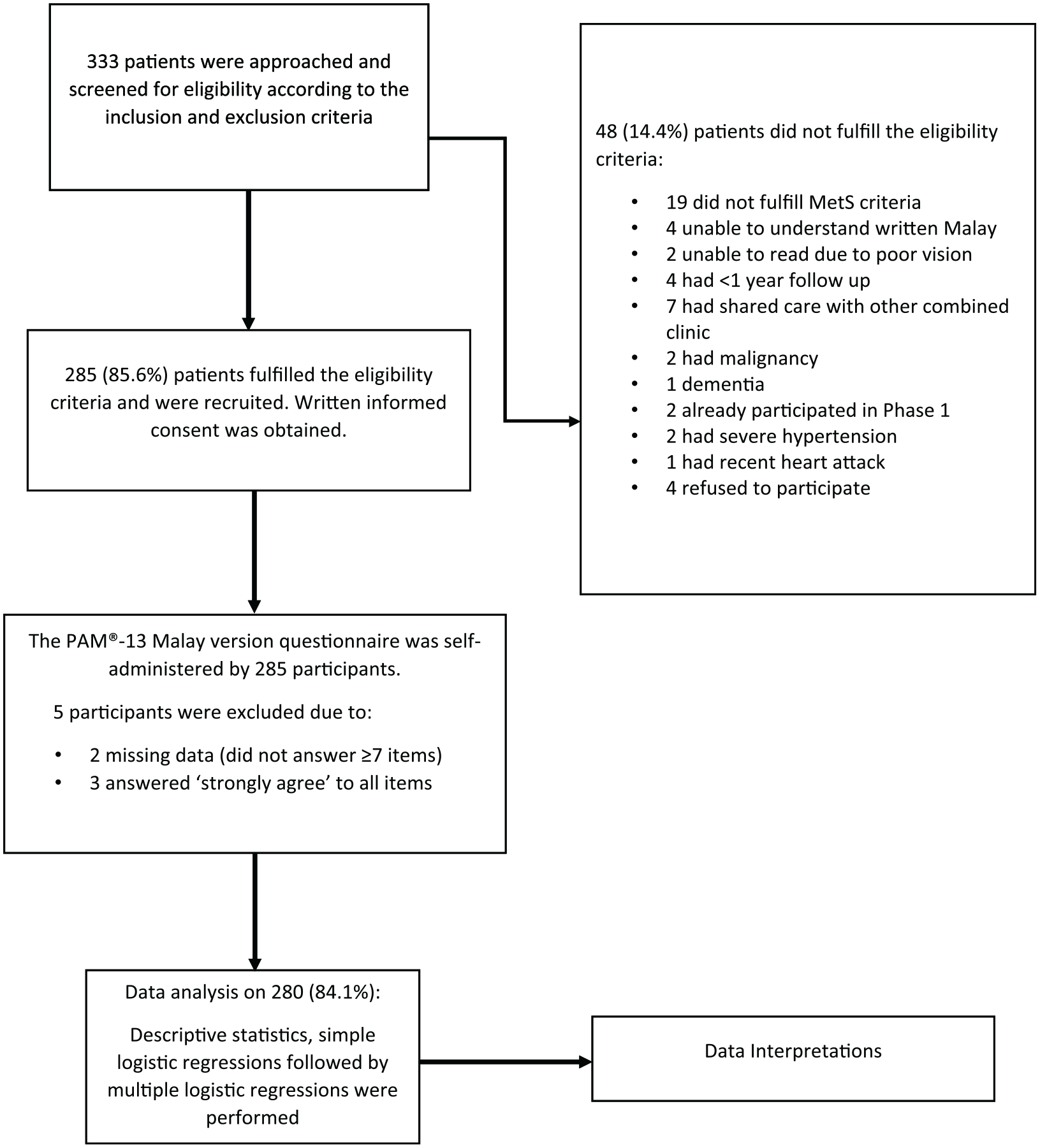
The conduct of the study.
The inclusion criteria were (a) aged between 18 and 80 years; (b) attended the primary care clinic for at least 1 year (to ensure that the patients included were our regular patients under follow-up at our clinic) 31 ; (c) had blood investigations (fasting plasma glucose [FPG], fasting serum lipid [FSL] and hemoglobin A1c [HbA1c]) done in the past 3 months; (d) able to read and understand the Malay language; (e) fulfilled at least 3 out of 5 diagnostic criteria for MetS based on the JIS definition 2009, 32 that is waist circumference (WC) South Asian cut-points: male ≥90 cm, female ≥80 cm; systolic blood pressure (BP) ≥130 mm Hg and/or diastolic BP ≥85 mm Hg or on treatment for hypertension (HPT); FPG ≥5.6 mmol/L or on treatment for elevated glucose; triglycerides (TG) ≥1.7 mmol/L or on treatment for dyslipidemia; high-density lipoprotein cholesterol (HDL-C): male <1.0 mmol/L, female <1.3 mmol/L or on treatment for dyslipidemia; and (f) willingness to participate in this study.
The exclusion criteria were factors that could alter the metabolic environment, that is (a) on renal dialysis; (b) presented with severe HPT (systolic BP >180 mm Hg and/or diastolic BP >110 mm Hg); (c) had secondary HPT; (d) diagnosed with circulatory disorders requiring secondary care over the past 1 year (eg, unstable angina, heart attack, stroke, transient ischemic attacks, peripheral vascular disease); (e) received shared care at primary and secondary care centers for complications of type 2 diabetes mellitus (T2DM) and/or CVD; (f) pregnant; (g) enrolled in another intervention study; (h) diagnosed with malignancy; (i) had any form of mental disorders or cognitive impairments that would affect the ability to answer the questionnaire, for example, dementia and mental retardation; and (j) unable to give informed consent.
Study Tool
The previously translated and validated PAM®-13 Malay version questionnaire was used in this study (Bahrom NH, et al, unpublished data). It consists of 13 items, framed within 2 domains, namely (a) passive and building knowledge and (b) taking action and maintaining behavior (Bahrom NH, et al, unpublished data). The PAM®-13 Malay version has an overall Cronbach’s α of 0.79 and an intraclass correlation coefficient of 0.45 (Bahrom NH, et al, unpublished data). These values indicate that the PAM®-13 Malay version is reliable and fairly stable over time. 33
Each item is answered based on a 4-point Likert-type scale, ranging from “strongly disagree” to “strongly agree” and “nonapplicable.” The responses were entered into the PAM® score sheet to generate the activation scores and levels, based on a theoretical range of 0 to 100 with higher PAM® scores indicating higher patient activation levels.7,13,14 Level 1 (not believing activation is important) reflects raw scores of 0 to 47.0. Level 2 (lack of knowledge and confidence to take action) reflects raw scores of 47.1 to 55.1. Level 3 (beginning to take action) reflects raw scores of 55.2 to 72.4, while level 4 (taking action) reflects raw scores of 72.5 to 100.7,13 For the purpose of this study, levels 1 and 2 were recategorized as low activation level (0-55.1); and levels 3 and 4 were recategorized as high activation level (55.2-100).
A research license was obtained from Insignia Health®, University of Oregon 26 to validate and utilize the PAM®-13 Malay version for research and educational purposes (License Number 1539265175-1570801175).
Sample Size Determination
A study by Hibbard et al 34 found that the prevalence for each of the activation levels were as follows; level 1 7%, level 2 14%, level 3 33%, level 4 46%. In our study, levels 1 and 2 were recategorized as low activation level, and levels 3 and 4 were recategorized as high activation level. Therefore, the sample size for our study was determined based on the prevalence of high activation level (levels 3 and 4), which was 79%. 35 By taking an α value of 0.05, with absolute precision of 5% and expected prevalence of 79%, the minimum sample size needed for our study was 254 using the following formula:

where n = sample size, Z = Z statistic for a level of confidence, P = expected prevalence (if the expected prevalence is 79%, then P = 0.79), and d = precision (if the precision is 5%, then d = 0.05). After considering a 20% attrition rate, our study aimed to approach approximately 330 patients in order to recruit at least 254 participants.
Patient Recruitment, Sampling Method, and Data Collection
Patients were recruited over 4 weeks at a university primary care clinic from August to September 2019. Three days per week were designated as data collection days. To ensure a standardized data collection method, data was collected by a trained research assistant. On the data collection days, patients were approached consecutively in the nurse’s assessment room and invited to participate. The study information sheet containing important information pertaining to the study, which included background, purpose, benefit, information regarding participation, study procedure, confidentiality status, and contact information, were given to those who were interested. Patients were then screened for eligibility according to the inclusion and exclusion criteria. Screening for the eligibility criteria were made through a self-administered questionnaire and review of the medical records. Patients’ medical history and blood investigations were required to make the diagnosis of MetS. FPG, TG, and HDL-C; as well as HbA1c (for those with diabetes) that were done in the past 3 months were retrieved from the electronic medical record. All the blood samples were analyzed at the Centre for Pathology and Diagnostic Research Laboratory (CPDRL), Universiti Teknologi MARA, which is an ISO 15189:2007 accredited laboratory (SAMM 688). FPG, TG and HDL-C were analyzed using enzymatic colorimetric reference methods on an automated analyzer (Roche® COBAS Integra 400). HbA1c was determined using the turbidimetric inhibition immunoassay analyzed on the same automated analyzer. These methods have been standardized against the approved International Federation of Clinical Chemistry reference method.
Study Procedure
During the eligibility screening, WC, height, weight, and BP were measured using standardized equipment and methods. WC was measured in centimeters (cm) using a nonstretchable measuring tape with the participants standing in a relaxed position and arms by their side. The measurement was taken at the midpoint between the inferior margin of the lowest palpable rib and the top of the iliac crest in horizontal plane. Measurement for each patient was repeated twice. If the measurements were within 1 cm of one another, the average was calculated. If the difference between the 2 measurements exceeded 1 cm, another 2 measurements were repeated.
Weight in kilograms and height in centimeters were measured using digital column stadiometer (Seca® GmbH & Co KG). The body weight was measured with the participant wearing minimal clothing and without shoes. The weight was recorded to the nearest 0.01 kg. Participants were asked to stand at the center of the scale, without support and with the weight being evenly distributed on both feet. Two measurements were taken and the mean of the readings was calculated. The height was measured using the stretch stature. Participants were requested to remove their shoes, and stand with their back, buttocks, and heels against the stadiometer holding their feet together. The height measurement was recorded to the nearest 0.1 cm. Two measurements were performed and the mean height was calculated. BMI was calculated as weight (in kilograms) divided by the square of the height (in meters) to the nearest 2 decimal points.
BP was measured using an automated digital BP monitor (Dinamap V100®, GE Healthcare), twice, at 2 minutes apart, on the right arm and in a sitting position. Participants were seated for at least 5 minutes and were not allowed to eat, drink caffeinated beverages, exercise, smoke cigarettes, or climb stairs 30 minutes before the measurements were taken. The average of 2 BP readings was taken for the analysis if the difference were within 5 mm Hg. If the readings differed by more than 5 mm Hg, the measurements were repeated.
Questionnaire Administration
Those who fulfilled the eligibility criteria and agreed to participate were recruited. Written informed consent was obtained. The previously validated PAM®-13 Malay version was given to the participants to be self-administered. Sociodemographic data, which included age, gender, marital status, education level, employment status, household income, and clinical factors such medications, self-reported health status, and smoking status, were collected. Participants were given approximately 15 minutes to complete the questionnaire, without referring to notes or family members. They were encouraged to ask for clarification from the researcher at any time should any query arise. Once the questionnaire was completed, participants were requested to return it directly to the researcher and the questionnaire was checked for completeness.
Definition of Terms
The cutoff points for the clinical factors, namely, WC, BP, FBS, TG, and HDL were defined according to the JIS criteria. 32 BMI (kg/m2) was categorized according to the recommended cutoff points for the Asian populations, that is, underweight <18.5, normal weight 18.5 to 23, overweight 23 to 27.5, and obese ≥27.5. 36
With regard to the definitions of sociodemographic variables, education levels were categorized according to the Malaysia education system, that is, no formal education, primary school education (standard 1, age 7 to standard 6, age 12), secondary school education (form 1, age 13 to form 5, age 17), and tertiary education (preuniversity course, eg, A levels, diploma, degree, masters, PhD). Household incomes were categorized into 3 categories, that is, the top 20% (T20) of the population with monthly household income of ≥RM 13 148, the middle 40% (M40) with monthly household income between RM 3001 and RM 13 147, and the bottom 40% (B40) with monthly household income of ≤RM 3000. 37 Self-reported health status was based on patient’s perception regarding their own health and overall well-being. It was categorized into 4 categories: poor, fair, good, and very good/excellent. 38
Data Entry and Statistical Analysis
Those who answered “strongly agree” or “strongly disagree” to all the items, those who answered ≥3 “nonapplicable” answers, and those who did not answer ≥7 items of the questionnaire were excluded from the analysis as these were the requirements to be able to compute a valid PAM®-score as stipulated by the Insignia Health®. 26 Data were then entered and analyzed using IBM® SPSS Statistics Version 24. Categorical variables were described in numbers and percentages whereas continuous variables were expressed as mean with standard deviation (SD) for normally distributed data or median with interquartile range (IQR) for nonnormally distributed data. Responses from the PAM®-13 Malay version were entered into the online PAM® Score Sheet to obtain the activation score (1-100) and activation level (1-4) for each patient. High activation level was defined as activation scores of 55.2 to 100 and low activation level was defined as activation scores of 0 to 55.1.
To determine the factors associated with high level of activation as the dependent variable, simple logistic regressions (SLogR) followed by multiple logistic regressions (MLogR) were performed. Purposeful selection of the independent variables began with SLogR. 39 Variables with a P value <.25 from the SLogR were included in the MLogR. The P value cutoff point of .25 was chosen because the more traditional levels such as .05 may not be able to identify clinically relevant variables.40,41 For the MLogR, forward and backward binary logistic regressions were performed because this study has only 1 dependent variable (DV), namely, “high activation level.” 42 Confounders were adjusted and model fitness was checked using Hosmer-Lemeshow goodness-of-fit test. Interactions, multicollinearity, and assumptions were also checked. A P value <.05 was considered significant.
Ethical Consideration
This study was conducted in accordance with the Declaration of Helsinki, the code of ethics of the World Medical Association. 43 Ethical approval was obtained from the Research Ethics Committee of Universiti Teknologi MARA [600-IRMI (5/1/6)/REC/61/19] prior to the conduct of the study.
Results
Participants Recruitment
Of the 333 patients who were approached and invited into the study, 285 (85.6%) fulfilled the eligibility criteria and were recruited. However, 5 participants were excluded from the analysis: Two were excluded due to missing data as they did not answer ≥7 items of the questionnaire and 3 were excluded as they answered “strongly agree” to all items. Therefore, the total number of participants included in the final analysis was 280 (84.1%).
Sociodemographic and Clinical Characteristics
The sociodemographic and clinical characteristics of the participants are shown in Table 1. The mean age was 60 years (SD ±8.61) with a range between 18 and 80 years. The majority of the participants were Malays (90.4%), married (87.5%), and had completed secondary school education (46.8%). More than half of the participants were pensioners (56.4%). Regarding household income, more than half (61.8%) belonged to the middle-income group (M 40). With regard to the clinical factors, the majority of the participants were obese (66.1%), had abnormal WC (95.4%), abnormal systolic BP (80.7%), and abnormal FPG (71.4%).
Sociodemographic and Clinical Characteristics of the Participants (n = 280).

Missing values.
Mean Activation Score and Distribution of Activation Levels
The mean PAM® score was 59.4 (SD ±10.2). Table 2 shows the distributions of participants in each of the activation level. Figure 2 shows the distribution of participants in the low (levels 1 and 2) and high (levels 3 and 4) activation levels. More than half of the participants were in the high activation level (61.8%).
Levels of Activation among Patients with Metabolic Syndrome (n = 280).


Distribution of the participants in the high and low activation levels.
Factors Associated With High Activation Level
Table 3 shows the results of the SLogR. Eleven variables were found to have P values <.25. These were being female (P = .159), having high education level (P = .025), being employed (P = .005) and pensioner (P = .172), having fair (P = .143), good (P = .0043), very good/excellent (P = .236) self-reported health, had abnormal TG (P = .157), HDL (P = .156), and had HbA1c of 6.5% to 10% (P = .203) and HbA1c of >10% (P = .198).
Simple Logistic Regressions on the Factors Associated with High Activation Level among Patients with Metabolic Syndrome. a

Variables with a P value <.25 (given in boldface) from SLogR were included in the MLogR.
The MLogR model contained 11 independent variables with P < .25 from the SLogR. The full model containing all these predictors was statistically significant, X′ (5, N ~ 280) ~ 22.196, P < .001, indicating that the model was able to distinguish between participants who reported high and low activation levels. The model as a whole explained between 7.6% (Cox and Snell’s R2) and 10.4% (Nagelkerke’s R2) of the variance in high activation, and correctly classified 65.0% of cases. Table 4 shows the results of the MLogR analysis. Two variables, namely, being employed and having good self-reported health status were found to be significantly associated with high level of activation. For those who were employed, the odds of having high activation level was 3.135 (95% CI 1.442-6.816) compared with those who were unemployed. For those who reported to have good health status, the odds of having high activation level was 6.482 (95% CI 1.243-33.792) compared to those with poor self-reported health status. The other variables i.e. being female, having high education level, abnormal TG, HDL, and HbA1c were adjusted as confounders.
Multiple Logistic Regressions on the Factors Associated with High Activation Level among Patients with Metabolic Syndrome. a
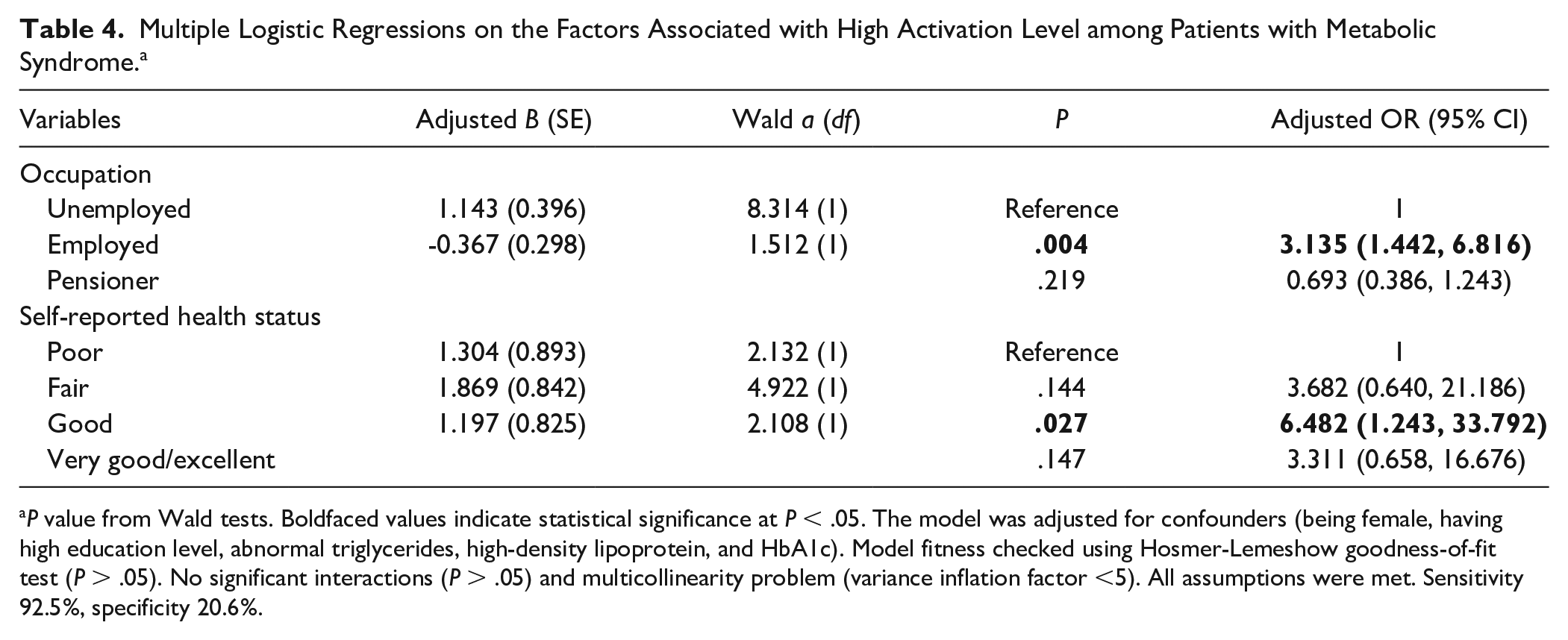
P value from Wald tests. Boldfaced values indicate statistical significance at P < .05. The model was adjusted for confounders (being female, having high education level, abnormal triglycerides, high-density lipoprotein, and HbA1c). Model fitness checked using Hosmer-Lemeshow goodness-of-fit test (P > .05). No significant interactions (P > .05) and multicollinearity problem (variance inflation factor <5). All assumptions were met. Sensitivity 92.5%, specificity 20.6%.
Discussion
To the best of our knowledge, patient activation has not been specifically reported in patients with MetS. The majority of studies on patient activation were conducted among patients with various chronic conditions in high income countries. This study is among the few conducted in a developing country that determined the levels of patient activation and the factors associated with it among individuals with MetS in a primary care setting. The mean activation score among our study population was 59.4 (SD±10.2). We initially expected to find a lower mean activation score among patients with MetS as it is a combination of at least 3 cardiovascular risk factors compared with other chronic conditions such as diabetes. However, the mean activation score in patients with MetS in our study was higher than the mean activation score of 57.4 (SD ±14.3) found in patients with diabetes alone in the Netherlands. 28 The mean activation score in our study was also higher in comparison to those with comorbid diabetes and chronic kidney disease in Australia where the mean activation score was 57.6 (SD ±15.5) 27 and among patients with multiple chronic conditions in the Netherlands where the mean activation score was lower at 54.1 (SD ±10.8). 29 In contrast to our study, the mean activation score was found to be higher at 67.8 (SD ±19.2) among patients with atrial fibrillation in America. 44 Patient-centered care and patient activation is being emphasized in America, and this could explain the higher mean score. Our finding is comparable to the Western populations such as those in Australia and the Netherlands, and this may be attributed to the focus on empowering patients to self-manage their cardiovascular risk factors in our academic primary care center. However, further studies are needed to confirm this observation.
In this study, 61.8% of individuals with MetS were found to have high activation level (levels 3 and 4). This is comparable to a study done among patients with diabetes mellitus in primary care where 58.6% were found to have high activation level. 45 However, the proportions of patients with high activation level were relatively lower at 54.4% among those with comorbid diabetes and chronic kidney disease in Australia 27 and also among patients with diabetes in the Netherlands (55%). 27 The proportion with high activation level among patients with diabetes in Ethiopia was even lower at 24.4%. 46 Comparatively, the percentage of patients with high activation level was higher at 65.1% among frequent users of primary health care services in Canada. 47 Variations in the activation levels in the various populations could be explained by the differences in the comorbidities, cultural background, and the health care system. The findings of this study are comparable to the Western population, where patient-centered care to increase patient empowerment and activation is being emphasized. However, more studies on patient activation should be carried out in the low- and middle-income countries to address the gap in the literature.
Only 2 factors were found to be significantly associated with high activation level in this study, namely, being employed and having good self-reported health status. First, this study found that those who were employed had the odds of 3.135 (95% CI 1.442-6.816) of having high activation level compared with those who were unemployed. However, similar finding from previous studies using multivariate analysis has not been described. Using univariate analysis, a similar finding was found by Aung et al 48 where the proportion of those who were employed was significantly higher (38%) in the high activation group (levels 3 and 4) compared with those in the low activation group (levels 1 and 2) (36.7%, P < .001) among patients with diabetes in Australia. Similar finding was also described among patients with atrial fibrillation in America where being in full-time employment was significantly associated with high activation level. 44 Individuals who are employed may have better education and health literacy. 38 This could explain its association with higher activation level as various studies reported a positive association between health literacy and patient activation.49,50 Second, our study also shows that those who reported to have good health status, had the odds of 6.482 (95% CI 1.243-33.792) of having high activation level compared to those with poor self-reported health status. This is comparable to the study among patients with diabetes in the Netherlands, which showed a 4.37 increase in patient activation scores for a 1-point increase in generic health status (P = .014). 51 Similarly, a study among older adult population with functional difficulties in America shows that patient activation was significantly associated with self-rated overall health status. 52 Individuals with good self-reported health status were more likely to be activated because they perceive that their health is important, therefore, they may have better knowledge, skills and confidence to self-manage their problems. 7 Various other factors such as social support, patient-physician relationship and health literacy have been associated with patient activation levels.46,51-53 However, these were beyond the scope of our study. Analyzing the complex paradigm of human behaviors and the interaction of different mediators of self-management is also beyond the scope of this study.
Strengths and Limitations
This study addresses the gap in the literature where studies on patient activation in developing countries are scarce. Moreover, it specifically involved patients with MetS in a primary care setting, where no such study has previously been conducted. However, this study has several limitations. First, the cross-sectional study design would not be able to draw a causal relationship between the various factors associated with patient activation. Second, the convenience sampling method used in this study may contribute toward sampling bias. However, measures were taken to reduce the sampling bias by ensuring that all patients who attended the clinics on the data collection days were consecutively approached and invited to participate. Third, this study was conducted in one primary care clinic where the majority of the participants were Malays. Therefore, the findings may not be generalizable to other primary care clinics in Malaysia with multiethnic population, as the Chinese and Indian ethnic groups were underrepresented in our sample. Finally, this study did not explore other potential factors that may affect patient activation levels, such as patient-physician relationship, family support, health literacy, and quality of life. Therefore, the interpretation of the multiple logistic regression results is limited to the variables included in this study. We appreciate that structural equation modeling or path analysis would be more robust to analyze the structural relationship between measured variables and latent constructs. However, these are beyond the scope of our study.
Practice Implications and Future Research
Findings of this study suggest the importance to measure patient activation levels among individuals with MetS in daily primary care practice. Assessment of patient activation levels is an important first step to guide the development of individually tailored interventions to improve their knowledge, skills, and confidence in self-management of their health. Patient Activation Interventions (PAI) may include problem solving support, audit and feedback, individualized care plans, financial incentive, peer/family support, lay health advisor/community health worker, psychological counseling, theory-based counseling, and skill building. 54 Those with high activation level can be coached to support their peers who have low activation level. Multidisciplinary management by physicians, nurses, dieticians, and/or pharmacists should also be integrated in the delivery of PAI. 55 A systematic review and meta-analysis on the effectiveness and safety of PAI for adults with type 2 diabetes showed that PAI modestly reduced intermediate outcomes such as HbA1c, systolic blood pressure, body weight, and LDL-cholesterol. 54 However, more evidence is needed to show that PAI reduce complications and long-term mortality. 54
Further research using systematic random sampling of patients with MetS involving other primary care clinics in Malaysia with multiethnic population is recommended to confirm the findings of this study. Additionally, further research should also explore facilitators and barriers influencing patient activation levels and self-management behavior. Further research is also needed to develop PAI for the Malaysian population and evaluate the effectiveness of such intervention in improving patient activation level and clinical outcomes, and eventually reduce cardiovascular complications and mortality.
Conclusion
In conclusion, this study has found that the majority of patients with MetS (61.8%) had high activation level. Being employed and having good self-reported health status were identified as significant predictors of high activation level. Despite its limitations, this study is the only study that determined such association among patients with MetS in the Malaysian primary care setting. Findings of this study could be used to develop PAI to improve self-management skills among patients with MetS in primary care. PAI may include problem solving support, individualized care plans, peer/family support, psychological counseling, theory-based counseling, and skill building delivered by multidisciplinary team in primary care. Those in high activation group can be trained to become mentors to support their peers who have low activation level. Further research is needed to evaluate the effectiveness of such intervention in improving patient activation level and clinical outcomes, as well as in reducing complications and cardiovascular mortality. Such evidence is necessary to guide policy and resource allocations in the Malaysian primary care setting.
Footnotes
Author Contributions
ASR, HAH, and NHB conceptualized and designed the study. ASR acquired the funding. ASR, MRI, and HAH supervised and coordinated the study. NHB acquired the data. NHB, MRI, and ASR analyzed and interpreted the data. NHB and ASR drafted the manuscript. NB, SFB, MSM, and HAH revised the manuscript critically for important intellectual content. All authors have read and given approval of the final manuscript. Each author has participated sufficiently in the work to take public responsibility for appropriate portions of the content as described above. All authors agreed to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work would be appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Ministry of Higher Education (MOHE), Malaysia: Prototype Research Grant Scheme (PRGS) No.: PRGS/1/2018/SKK05/UiTM/01/2 or 600-IRMI/PRGS 5/3 (003/2019). The funding body did not play any role in the design of the study, data collection, analysis, interpretation, or in the writing of the manuscript.