
Abstract
The American Patient Activation Measure–22 questionnaire (PAM-22) quantifies the knowledge, skills, and confidence essential to manage own health and health care. It is a central concept in chronic illness care models, but studied sparsely in homeopathic hospitals. PAM-22 was translated into Bengali and a cross-sectional study was undertaken in chronically ill 417 patients visiting the outpatient clinic of Mahesh Bhattacharyya Homeopathic Medical College and Hospital, India. Response rate was 90.41%. Data were analyzed using Rasch rating scale model with Winsteps. Activation score was 54.7 ± 8.04 or 62.13% of maximum score. PAM scores differed significantly by age, education, income, and health status (P < .05). The items had good data quality fit statistics and good range of difficulty. The construct unidimensionality was confirmed by good model fits for Rasch model and principal component analysis of residuals found no meaning structure. The questionnaire showed acceptable psychometrics. Patient activation was moderate and needs to be improved.
Introduction
The chronic illness care model emphasizes patient-oriented care, with patients and their families integrated as members of the care team. It summarizes the basic elements for improving care in health systems at the community, organization, practice, and patient levels and characterizes the ongoing adjustments by the affected person and interactions with the health care system. 1,2 A critical element in the model is “activated” patients, with the skills, knowledge, and motivation to participate as effective members of the care team. Activation of patients actually refers to the confidence, knowledge, and behaviors that enables patients to become actively engaged in their health. Patient activation also remains the central concept in consumer driven health care approach. In this framework, improvement of self-management strategies strengthens the patients’ activation levels in the course of the treatment. Self-management of chronic diseases refers to aspects such as medication use, lifestyle changes, and health behavior changes to prevent long-term complications or increase adherence to treatment regimens and prevention of long-term complications. Success of self-management is likely to depend on self-management skills and patient activation. 2 If activation is increased, a variety of improved self-management behaviors will follow. Therefore, it is important to identify patients lacking these skills, to develop and evaluate interventions to enhance the skills necessary for activation and to tailor support for self-management by adjusting the intervention to the individual patients’ level of activation. To attain these goals, it is crucial to have valid and reliable assessment methods for the individual level of activation. A process for conceptualizing and operationalizing what it means to be “activated” and delineate the process, a measure was developed for assessing “activation,” namely the Patient Activation Measure (PAM), 3 a valid, highly reliable, unidimensional, probabilistic questionnaire consisting of 22 items that reflects a developmental model of activation. Another 13-item reliable and valid short version of the PAM 4 is also available in English, Danish, Dutch, Norwegian, and German languages. The measure has good psychometric properties indicating that it can be used at the individual patient level to tailor intervention and assess changes.
Research has repeatedly shown that a higher score on the PAM is positively associated with various health related behaviors, such as preventive care and lifestyle behaviors, information seeking and use of health information, health outcomes and health care use, monitoring and medication adherence, conduct in the patient-provider encounter and self-management. 5 Because the measure is developmental, interventions could be tailored to the individual’s stage of activation. The approach is economical because it is targeted rather than omnibus. Employers could also use the measure to assess interventions designed to increase engagement and activation among their employees.
Despite far-reaching consequences, to the best of the authors’ knowledge, the PAM has not been studied adequately in India in hospital settings. Furthermore, though a considerable amount of homeopathic research has concentrated on chronic illnesses, 6 patient activation remained relatively unevaluated. Since many of the patients present with problems regarding the management of health and chronic diseases in India in homeopathic hospital settings, 7 there is a definite clinical and scientific need for an instrument that can examine patient activation, formulate strategies in health support, information and communication. Authors intend to use the measure to assess individual patient activation and to develop care plans tailored to that patient and integrated into the processes of their care in Mahesh Bhattacharyya Homeopathic Medical College and Hospital, West Bengal, India. An official, validated Bengali version of the PAM would be suitable and relevant for this purpose. Therefore, a research project was undertaken in order to translate the American PAM-22 into a Bengali version, establish the psychometric properties, validate it in a panel of chronically ill patients, and thereafter measure the activation level of the patients.
Methods
All participants were provided with the self-administered questionnaire along with patient information sheets in local vernacular Bengali and informed consents were obtained. The survey matter and question items were also explained verbally to the participants by the research assistant to facilitate easy understanding. To ensure anonymized protection of patient’s privacy, all the patient identifiable information was concealed. The 22 questions were provided with a 4-point disagree/agree response format (strongly agree = 4, agree = 3, disagree = 2, strongly disagree = 1). Another section in the questionnaire sought information regarding patients’ gender, age, residence, chronic conditions, self-rated health status, level of education, and monthly family income to test for any putative associations and differences. The filled-in questionnaires were put inside opaque envelops and sealed at the survey site. All these were sent for data extraction in a specially designed MS Excel master chart that was subjected to statistical analysis in different statistical computational websites.
The 6 different stages used for the development of the questionnaire are seen in Figure 1.

Translation and cross-cultural adaptation sequence of the used Bengali Patient Activation Measure–22 (PAM-22) questionnaire.
Stage 1 (forward translation): An expert committee consisting of methodologists, health professionals, translators, and a language professional was set up. For the forward translation from English into Bengali, 2 independent native Bengali speaking translators translated the English version of PAM into the target language Bengali (T1 and T2). One of the translators was a clinician and therefore aware of the concepts that were being measured with the PAM and the other translator was a language specialist with no medical background.
Stage 2 (synthesis of T1 and T2 into T1,2): The 2 translators had to then agree on 1 new consensus version of the translation (T1,2). This consensus version was overseen by the expert committee overseeing the project.
Stage 3 (back translation): For the back translation from Bengali into English, 2 English language translators (BT1 and BT2) were required. Though born in India, they both have been residing in the United States for more than 15 years. They both independently translated T1,2 back into English. They were blinded to the original English version of the PAM during this process.
Stage 4 (committee review): The committee reviewed all the translations (T1 and T2, T1,2, B1 and B2) and the written report comparing the back translations with the forward translation T1,2. Based on those translations, the prefinal version was developed.
Stage 5 (face validity): The prefinal version of the questionnaire was tested on randomly (simple random sampling) chosen 15 patients visiting outpatient clinics of Mahesh Bhattacharyya Homeopathic Medical College and Hospital. Each completed the questionnaire and was then asked the meaning of each questionnaire item as well as whether or not they had problems with the questionnaire format, layout, content, clarity, language, instructions, or response scales. Any difficulties were noted and included in the final report. A detailed report written by the interviewing person, including proposed changes of the prefinal version based on the results of the face validity test was then submitted to the expert committee.
Stage 6 (committee appraisal): The final version of the Bengali PAM was developed by the committee based on the results of the face validity testing and the written report. Thus, all stages 1 to 6 were successfully completed. The final version of the PAM for patients can be found as an additional file (available online).
Validation
The purpose of cross-cultural adaptation is to try and ensure consistency in the content and face validity between the original and the translated versions of a questionnaire. Content validity of the PAM questionnaire was previously evaluated on the original English version, and was therefore not tested in this study. Additional testing was done to evaluate construct validity. Thus, in a cross-sectional study in January 2014, 417 patients from different outpatient clinics of Mahesh Bhattacharyya Homeopathic Medical College and Hospital were asked to fill in the new Bengali version of the PAM-22. The questionnaires were given to them to fill in immediately. Of 417 patients approached, 377 (response rate 90.41%) returned the questionnaire.
Statistical Analysis
The Rasch measurement model is a mathematical model of fundamental measurement; the kind of measurement used in the natural and physical sciences. When the data fit the model the result is an equal interval scale. As with a yardstick, the people being measured and the questions doing the measurement are both located on this scale. Data quality fit statistics are used to assess the degree to which each person’s responses, each item’s performance, and each response category fit model expectations. 8 Since the analysis is an iterative procedure in which responses of people, difficulty of items, and performance of response categories all work in a conjoint manner, retaining respondents having answers that do not make sense in terms of model expectations can seriously distort the estimation of person scale location, item scale location, and response category performance. The initial analysis identified 24 respondents who provided seriously misfitting data. These respondents were deleted and the final analysis performed with the 353 better fitting respondents.
One of the advantages of the Rasch model is that it builds a hypothetical unidimensional line along which items and persons are located according to their difficulty and ability measures. The items that fall close enough to the hypothetical line contribute to the measurement of the single dimension defined in the construct theory. Those that fall far from it are measuring another dimension which is irrelevant to the main Rasch dimension. Long distances between the items on the line indicate that there are big differences between item difficulties, so people who fall in ability close to this part of the line are not as precisely measured by means of the test. It is argued here that misfitting items are indications of construct-irrelevant variance and gaps along the unidimensional continuum are indications of construct underrepresentation. 8
Results
Response Category Performance
Response categories are categories, not points. As such, they function as buckets into which respondents place themselves when answering a question. Fit statistics for person, items, and response categories are in two forms. Infit is most sensitive when the person and the item are close together on the measurement scale/yardstick. Outfit is most sensitive when the person and the item are located far apart on the measurement scale. A fit value of 1.0 is perfect fit to the model. Perfect fit is never expected, but fit values between 0.5 and 1.5 indicate good model fit. The response categories had good fit (the value of 1.68 for disagree strongly is perfectly acceptable given the low frequency of use.) There was some overuse of “agree” and underuse of “disagree.” This reflects respondents avoiding the “disagree” category and selecting “agree” instead. This avoidance is not sufficient to disrupt the measurement. Missing responses do not have an effect on the results since the Rasch model is stochastic rather than deterministic (Table 1).
Response Category Performance.

Item Performance
To have a useful measure items must not only have good fit to the model, but must cover a large enough range on the scale/yardstick to provide precise measurement of people. Items thus must have good model fit as well as sufficient variability in difficulty. Items 22, 9, 3, 11, and 15 were the most difficult ones, whereas items 7, 2, 1, 4, and 10 were easy to score. The items have good variation in difficulty, ranging from 61.3 to 38.3. Several items are located at the easy end of the scale. Items 16, 6, 7, 2, 1, 4, 10 all calibrate below 40 on the 0 to 100 scale. These items occupy a location on the measurement scale where there are very few people. These items could be eliminated without decreasing the measurement precision, and may be considered as an indication to use PAM-13 instead. All items have acceptable fit to the model. The apparent misfit of item 22 is because of it being the most difficult item (Table 2).
Item Difficulty and Fit.

Person Measurement
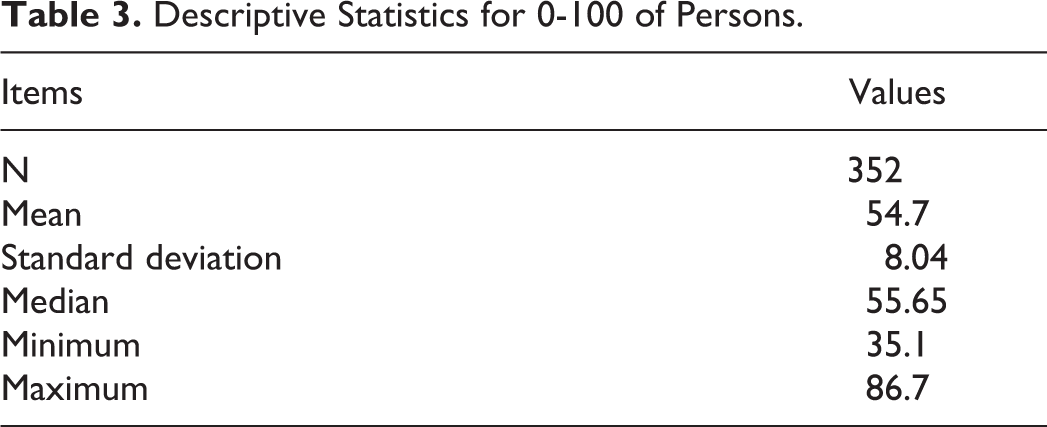
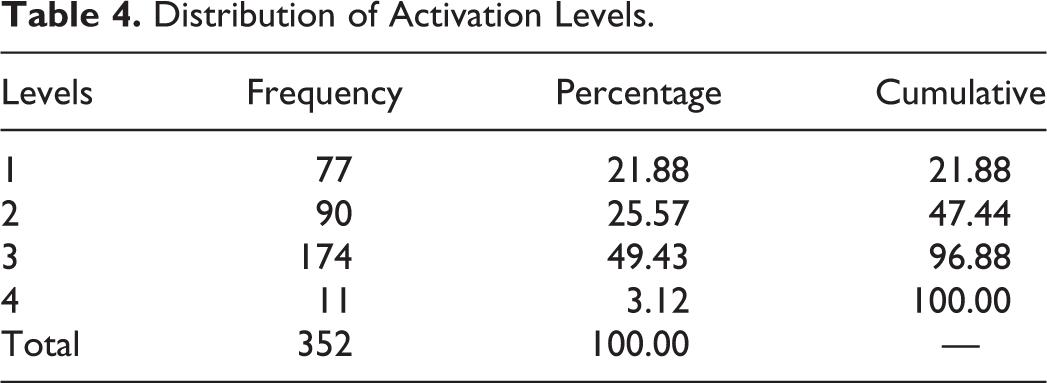
The distribution of 0-100 activation scores is shown in Figure 2. One person had an extreme high score by answering all questions with “strongly agree” and was deleted because the quality of their data cannot be evaluated. The descriptive statistics of the distribution in Figure 2 are shown in Table 3. Average PAM 0-100 scores are 54.7 ± 8.04 or 62.13% of the maximum score. The distribution of 0-100 scores is clearly bimodal. These 2 modes reflect 2 clusters of scores that are best described as low and moderate activation. 0-100 activation scores are generally collapsed into the 4 levels. The higher is the level, the greater is the activation. The distribution of levels is shown in Table 4. Respondents were relatively equally divided between low activation (levels 1 and 2) and moderate activation (level 3). Only 3% are in the highest level of activation (level 4).
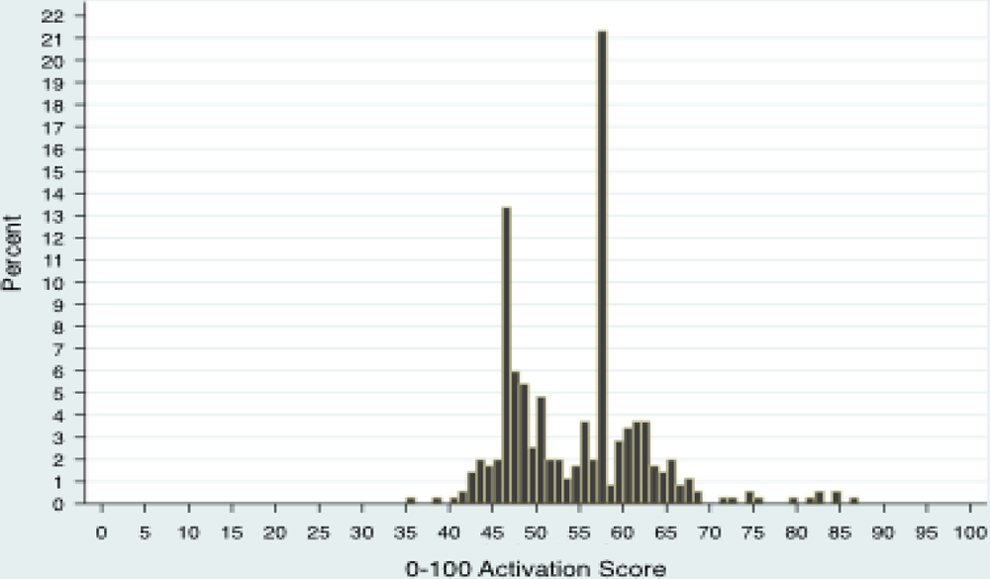
Percentage distribution of 0-100 activation scores.
Descriptive Statistics for 0-100 of Persons.
Distribution of Activation Levels.
Person Fit Statistics
Infit and outfit are generally classified into four categories based on the fit value. A fit value of 1.0 is perfect fit to the model. Values between 0.5 and 1.5 are indicative of very good quality data. Fit values less than 0.5 indicate muted responses in which people gave the same answer to questions that varied in difficulty when at least some of their answers should have been different. Respondents in this category show varying degrees of response set. Fit values greater than 1.5 indicate more than expected variability in responses. This is the case when a person gives a more negative or positive response than was expected given the activation score and the difficulty of the question. Fit values greater than 2.0 are considered potentially problematic in that at least some of the person’s responses were very unexpected relative to the model. Table 5 shows the distribution of persons in these fit categories for both infit and outfit statistics. Since we initially removed the most misfitting respondents none of those in the “answers do not make sense” category have extreme misfit. For the low- and high-variability categories the issue being identified is that of noise in responses. The 2 variability categories indicate that some other construct than activation is influencing how people answered questions. Experience with activation measurement finds that people in the low- and high-variability categories are perfectly useable, but the relationship between their activation scores and outcomes and behaviors may be slightly lower than in the case of respondents providing very good quality data. True score reliability in measuring people cannot be known since it depends on the assumption one makes about the source of the measurement error. The Rasch approach is therefore to calculate the reliability of person measurement (how much measurement error exists) under 2 different assumptions about the source of the measurement error. Real person reliability assumes that all of the measurement error is random error. Model person reliability assumes that all of the measurement error is actual misfit with the model. True score reliability (if it could be known) is somewhere between real and model person reliability. Real person reliability is .85 and model person reliability is .89. These values are consistent with what is normally observed for the PAM-22.
Distribution of Person Fit.

Sociodemographics
PAM-22 scores differed significantly by age (F = 3.195; P = .024), education (F = 7.835; df = 376; P < .001), income (F = 12.029; df = 376; P < .001), and health status (F = 7.313; df = 376; P = .001); however, gender (t = 0.45; P = .653), residence (F = 2.566; df = 376; P = .078), and types of chronic condition (F < 1) did not seem to influence the activation scores significantly. When the analysis of variance detected that not all groups had the same mean PAM scores, the Scheffe multiple comparisons test results are reported for what group means are significantly different. In education, Scheffe tests revealed that groups 1 and 2 (10th class/below and high school, respectively; P = .006) and groups 2 and 3 (high school and graduate/above, respectively; P = .005) were significantly different. In income, Scheffe tests revealed that all 3 groups (group 1 monthly household income in Indian rupees <10 000; group 2 Indian rupees 10 000-30 000; group 3 Indian rupees >30 000) differed significantly from each other (groups 1 and 2 P = .019; groups 1 and 3 P = .001; groups 2 and 3 P < .0001). In health status, Scheffe test revealed that groups 1 and 2 (P = .006) and 1 and 3 (P = .014) were significantly different. Though cross-sectional design of the study does not allow drawing of any causative conclusions, higher mean PAM scores were found to be associated with age-group of 18 to 30 years (56.50 ± 8.70), education status of graduate or above (57.78 ± 9.55), income status of Indian rupees >30 000 (64.63 ± 9.70), and health status very good to excellent (62.76 ± 11.00; Table 6).
Sociodemographic Features and Patient Activation Measure (PAM) 0-100 Score Differences.
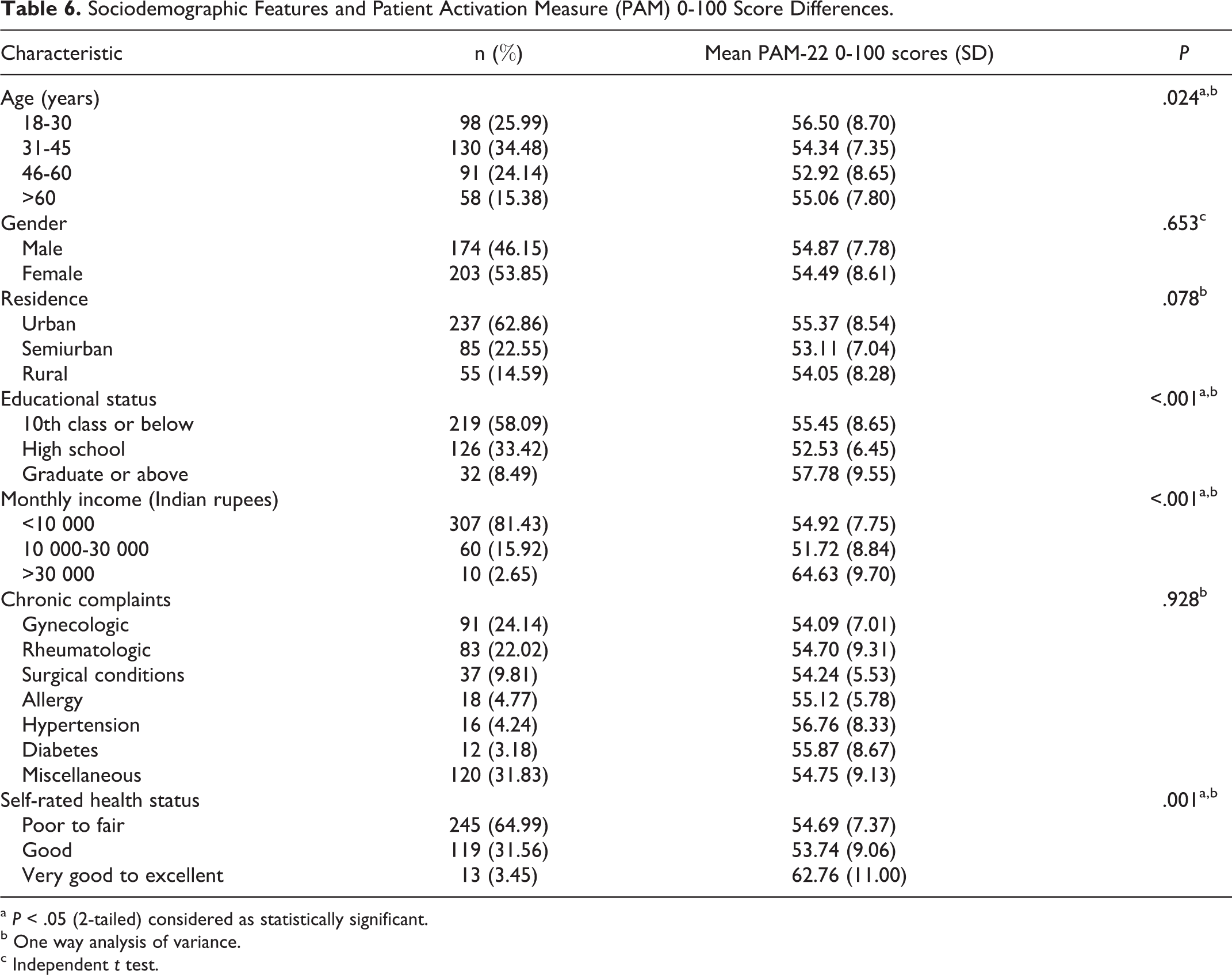
a P < .05 (2-tailed) considered as statistically significant.
b One way analysis of variance.
c Independent t test.
Discussion
The Bengali PAM-22 appears to be a promising instrument to measure patient activation. The 22 items had good data quality fit statistics and a good range of difficulty. The unidimensionality of the construct was confirmed by good model fits for the Rasch model and principal component analysis of the residuals found no meaningful structure. Activation of the patients visiting the homeopathic hospital was moderate, may be attributable to cultural differences and needs to be examined in future studies. Activation differed significantly by age, education, income, and health status. The bias of obtaining socially desirable overstated responses from the respondents to please the clinician was apparent in the psychometric results. Despite these limitations, this study also has several strengths. First, it is the first ever conducted study that captures information on this context. Second, to reduce bias, the respondents were sampled systematically. Third, the homeopathic care provided by the homeopathic hospital was similar to the average Indian homeopathic care, and thus our study appears to be generalizable to India.
Improving the activation levels of patient populations, being strongly associated with upgradation of self-management behavior, 2 can be used as an indicator of the performance of providers or delivery systems and can be employed for quality assessment and public accountability purposes. Consumers will likely want to know which providers and systems are performing well in this area and comparative data could drive purchaser and consumer choices. Knowing a person’s activation level is relevant because it can help providers to effectively communicate with their patients and to tailor health messages and self-management goals. 9 Compared with the regular patient approach, an intervention with tailored messages has proven to lead to greater improvement in the patients’ biometrical clinical indicators, in their adherence to prescribed medication regimens and to a reduction in hospitalizations and use of the emergency department. 10 Furthermore, patient activation has proven to be a changeable characteristic. 11,12 This makes the concept even more relevant since it can not only be used for categorizing patients and consumers and tailoring support and education but also for actual improvement of consumer participation with respect to health and health care, both on an individual and on a population level.
In some studies, the relative contribution of health literacy and patient activation was examined in relation to a number of health-related behaviors and choices. Two studies showed that the association between patient activation and measures of health literacy was weak, indicating that these are 2 distinct concepts. 13,14 The other study distinguished between numeracy, literacy and activation. 15 A recently conducted study suspected the role of language and culture on patient activation and emphasized the need to examine it in future studies. 16 Since American studies have demonstrated that a higher score on the PAM positively influences various health-related behaviors, 9,17 one can expect a positive influence on health by improving the patient activation and by helping professionals tailor their care to the specific needs and possibilities of their patients, which may vary by their activation status. Supporting patients in their role as self-managers is an essential element of high quality chronic illness care. As with other dimensions of quality, the ability to measure is a prerequisite to improvement. It can be used at the aggregate level to evaluate and compare the efficacy of interventions and health care delivery systems. It is not unreasonable to expect that providers delivering high-quality care would have, over time, more activated patients.
Finally, this is the very first step in understanding patient activation and its role in health care quality, outcomes, and cost containment and ultimately to more effective and efficient delivery systems in India, especially in any homeopathic hospital setting. Further validation in other Indian samples will have to confirm whether the sequence of the original American scale will require readjustment in India.
Footnotes
Acknowledgments
The authors are grateful to Insignia Health, LLC, for the license (not associated with money) to translate the PAM-22 into Bengali. The authors would like to acknowledge Dr Nikhil Saha, Principal in-Charge, Mahesh Bhattacharyya Homeopathic Medical College and Hospital, for allowing us to carry out the study successfully in his institution. The authors would like to thank Mr Kohinoor Chakraborty, MA, and Dr Achintya Kumar Datta, MD, for doing the English to Bengali translations as well as Dr Sankar Sengupta, PhD, and Mr Indrajit Mitra, MBA, for back-translations. Additionally, the authors wish to thank Prof Malay Mundle, MD, Prof Satadal Das, MD, Dr Mahua Pal, PhD, Mr Kohinoor Chakraborty, MA, for serving on the expert committee and providing input in the final version of the questionnaire. The authors will also remain grateful to Mr Arunabha Bhowmick for technical support and to the patients for their participation in the study.
Author Contributions
SS, MK, ERM, JH: Concept and design of study, analysis and interpretation of data, drafting and revising manuscript. SG, GN: Concept and design of study, data acquisition. RP, RM, MK, SP, SSA: data acquisition. JSA, GC: Concept and design of study, drafting and revising article. All authors read and approved the final article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics approval for this study was obtained from the Institutional Ethics Committee of Mahesh Bhattacharyya Homeopathic Medical College and Hospital.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.