
Abstract
Introduction
One of the major causes of mortality in children younger than 5 years is the simultaneous occurrence of more than 1 disease. 1 Diarrhea and acute respiratory infection (ARI) are the main causes of child mortality and morbidity in low- and middle-income countries. 1 ARIs are caused by virus or bacteria that affect the upper respiratory tract (nose, vocal cords, and ears) and lower respiratory tract (trachea, bronchi, bronchioles, and alveoli). Diarrhea is caused by parasites, bacteria, and viruses that are found in feces and can be spread through water, flies, food, and improper washing of the hands. Comorbidity is defined as the concurrent occurrence of more than 1 disorder in the same child or adolescent either at the same time or in some causal sequence. 2
For instance, occurrence of diarrhea leads to susceptibility of pneumonia in malnourished children 3 ; and malnourished children have a higher susceptibility of developing diarrhea, thereby creating a vicious cycle. 4 Diarrhea increases the chances of ARI by causing significant loss of micronutrient and dehydration, it and weakens the immune system therefore predisposing the child to a substantial risk of infection. Comorbidity of diarrhea and ARI can either be simultaneous (both occurring at the same time) or sequential (where the occurrence of one leads to the occurrence of the other). 4 Walker et al 5 found out that diarrhea and ARI in children <5 years was present as simultaneous comorbidity and the relationship became stronger with the severity of the disease.
ARI is classified into upper respiratory infection and lower respiratory infection. Pneumonia is the most common type of lower respiratory infection and the leading infectious cause of mortality in children <5 years. Globally, pneumonia (14%) and diarrhea (14%) account for more deaths in children under 5 years as compared with HIV/AIDS (4%), malaria (16%), and measles (1%) combined. A systematic analysis conducted by Liu et al 6 revealed that approximately 4.4 million children under 5 years of age will succumb to infectious diseases such as diarrhea and ARI by 2030 and 60% of these deaths will occur in sub-Saharan Africa.
Kenya is among 15 countries that account for three-quarter of mortality due to pneumonia and diarrhea. 7 Pneumonia has a mortality rate of 50.3 deaths per 10 000 children under 5 years of age in Kenya. 8 Diarrhea is the second leading cause of under-5 mortality. 9 According to the Kenya Demographic Health Survey (KDHS) 2014 report, 15% of the children under the age of 5 years had diarrhea and 9% had ARI within 2 weeks preceding the survey.
A study conducted by Walker et al 7 revealed that diarrhea and ARI have overlapping epidemiology, which is partly due to shared risk factors such as inadequate breastfeeding, malnutrition (includes undernutrition, which is categorized as underweight, stunting, and wasting) and insufficient zinc. Stunting is defined as low height for age—a measure indicative of a chronic restriction of a child’s potential growth. Wasting is a measure of acute undernutrition while underweight is defined as low weight for age. 10 Findings by Bbaale 11 showed that children who were exclusively breastfed for the first 6 months, socioeconomic status, type of house the child lived in, maternal occupation, age of child, and nutritional status were significant factors associated with both pneumonia and diarrhea. In a study carried out by Leung et al 12 in under-5 children in Dhaka, Bangladesh showed that younger age of child, male gender, undernutrition, lower maternal education, low wealth quintile, and poor breastfeeding practices were associated with concurrent occurrence of diarrhea and pneumonia.
Most of the risk factors associated with ARI and diarrhea are modifiable, 13 and because the 2 outcomes also share some major risk factors, they can be tackled through integrated interventions. Kenya is a signatory of the Global Action Plan for Prevention of Pneumonia and Diarrhoea (GAPPD), which is a framework of key interventions that aims to end deaths due to diarrhea and pneumonia by 2025. 14 The government has taken up the Kenya Action Plan for Prevention of Pneumonia and Diarrhoea (KAPPPD), which is an outline on reducing child mortality due to pneumonia and diarrhea. 15 Despite numerous government efforts to reduce under five mortality due to diarrhea and pneumonia, the number of diarrhea cases in Kenya reduced by only 2% (17% in 2008 to 15% in 2014) and ARI cases increased by 1% (8% in 2008 to 9% in 2014). Kenya remains at a higher prevalence of diarrhea (21%) and pneumonia (16%) than the prevalence in Africa (diarrhea 17%, pneumonia 14%). 16 This is a major public health concern that will deter Kenya from achieving GAPPD goal of zero deaths due to diarrhea and pneumonia by 2025.
Studies carried out in Kenya such as a study by Simiyu 17 and Onyango et al 18 have focused on diarrhea and pneumonia independently without considering their occurrence concurrently. The interventions proposed have in turn focused on each outcome separately. This study seeks to assess the prevalence of comorbidity of pneumonia and diarrhea in children <5 years, and to identify risk factors associated with comorbidity of pneumonia and diarrhea in children <5 years.
Findings from this study will provide the basis for an integrated package of public health interventions that will combat combined comorbidity of diarrhea and ARI in Kenya’s children <5 years.
Methods
Study Setting
Kenya is located in the eastern part of Africa in latitude 5° north and 5° south and between longitude 24° and 31° east. The country is divided into 47 counties and has a total area of 582 646 km2.
Sample Design, Sample Size, and Sample Population
Secondary data from the Kenya Demographic Health Survey (KDHS) 2014/2015 19 was used for analysis. KDHS is a national household survey conducted every 5 years that provides information to monitor population and health situation in Kenya. The sample for KDHS 2014 survey was adopted from the fifth National Sample Survey and Evaluation Programme (NASSEP V) which is a master sampling frame. Calculations for sample size depend on the desired relative standard error at domain level and the number of domains. 20 The 2014 KDHS was designed to produce representative estimates for most of the survey indicators at the national level, for urban and rural areas separately, at the regional (former provincial) level, and for selected indicators at the county level. To meet this requirement, the sample had 40 300 households from 1612 clusters across the country. In rural areas there were 995 clusters and 617 clusters in urban areas. A 2-stage sample design was used where samples were selected independently. The first stage involved selecting 1612 enumeration areas with equivalent likelihood from the NASSEP V sampling frame. In the second stage, the households were listed and 25 households selected from each cluster. Data collection was done using structured questionnaires administered by trained enumerators. Interviewers visited only preselected households and no replacement of the preselected households was allowed. The women’s questionnaire and household questionnaire was administered in all households. Data entry was done using CSPRO software.
A sample size of 20 964 children <5 years old was used in the study.
Outcome, Exposure, and Confounding Variable
The dependent (outcome) variable was comorbidity of diarrhea and ARI. The outcome variable was generated by combining the variable for if child had diarrhea and if child had ARI. Presence of comorbidity was assigned the value 1 and 0 otherwise. ARI was estimated by asking mothers who have children under the age of 5 years whether in the 2 weeks preceding the survey, the child had been ill with a cough accompanied by short, rapid breaths, and difficulty in breathing as a result of chest problem. 19 Diarrhea prevalence was estimated by asking mothers of children born 5 years before the survey whether their children had experienced episodes of diarrhea in 2 weeks preceding the survey. The World Health Organization defines diarrhea as passage of 3 or more loose or liquid stools per day (or more than frequent passage of stool than is normal for an individual). 9
The exposure (explanatory variables) consisted of child’s age in months, child’s gender, place of residence (rural and urban), wealth quintile, caregiver’s age, caregiver’s education, exclusive breastfeeding below 6 months, and nutritional status (wasting, stunting, and underweight).
Data Management and Data Analysis
Data management and analysis was done using STATA 14. Data management involved merging of the children’s data set (KR file) and household dataset (HR file) using a unique identifier.
Descriptive weighted analysis was done to show of children under 5 years of age who experienced comorbidity. Frequencies, row percentages and confidence interval were obtained from the tabulation. Missing values were excluded in the overall weighted total in order to account for all children <5 years.
Weighted descriptive analysis and regression analyses were done in order to account for stratification in the data. The weights were obtained by dividing the women’s individual sample weight (variable v005) by 1 000 000.
Bivariate logistic regression was carried out to assess the effect of individual risk factors on comorbidity. Risk factors that were significant from bivariate logistic regression were incorporated in the multivariate logistic regression. A P value <.05 was considered to be statistically significant.
Results
Descriptive Analysis Results
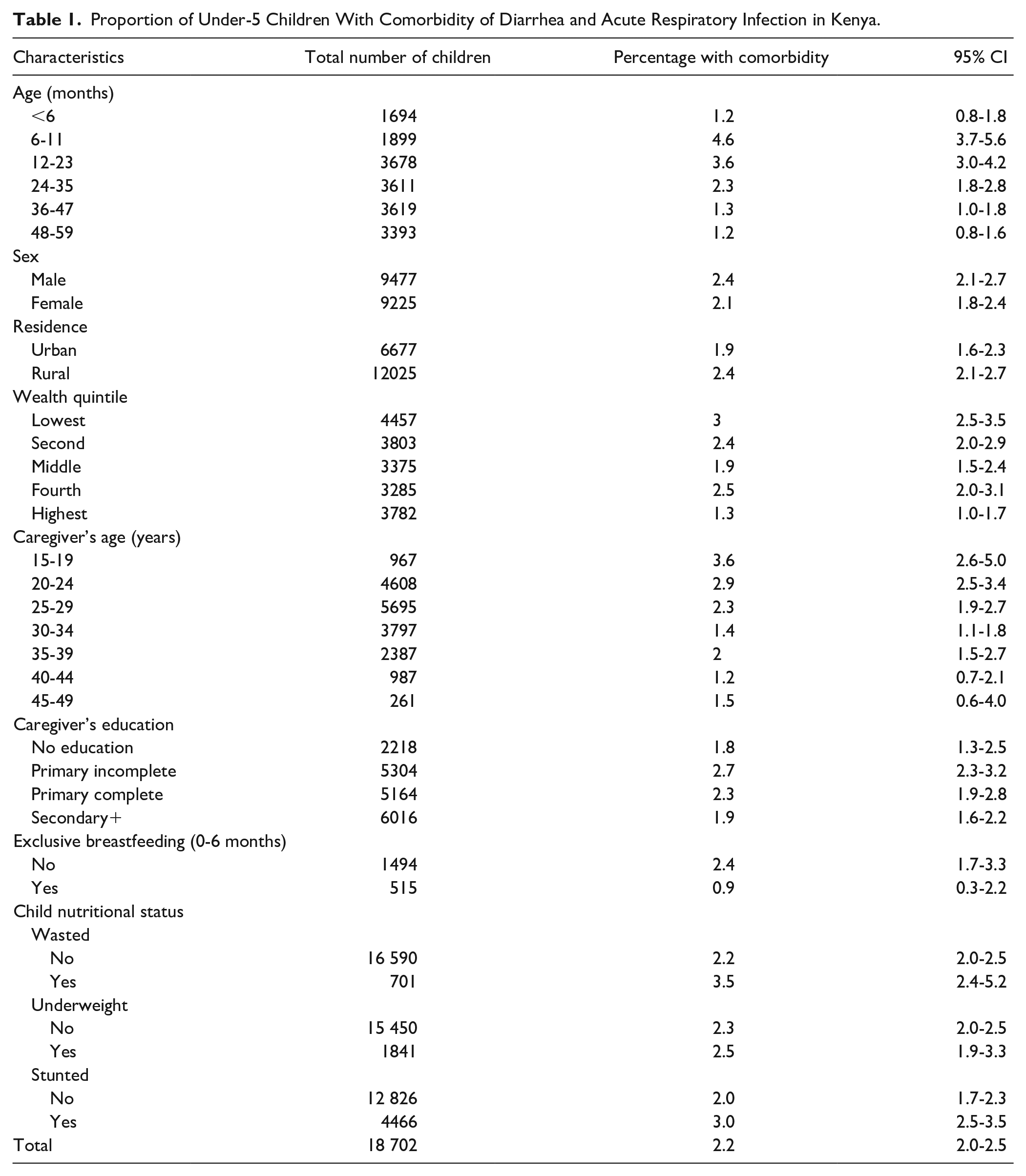
Table 1 shows the proportion of under-5 children with diarrhea and ARI. Out of the 18 702 children involved in the survey, 411 children (2.2%) had comorbidity from diarrhea and ARI within 2 weeks preceding the survey. The highest percentage of children with comorbidity of diarrhea and ARI were aged 6 to 11 months (4.6%), followed by children aged 12 to 23 months (3.6%), and children whose caregivers were between 15 and 19 years old (3.6%). Families in the highest wealth quintile and caregivers aged 40 to 44 years of age had the least proportion of children with comorbidity (1.3% and 1.2%, respectively).
Proportion of Under-5 Children With Comorbidity of Diarrhea and Acute Respiratory Infection in Kenya.
Risk Factors for Comorbidity of Diarrhea and ARI
From Table 2, sex, residence, exclusive breastfeeding, wasted and underweight children did not have significant influence on comorbidity. After 6 months, the risks of combined infections decreased with a child’s aging status, with those between 6 and 11 months identified as 4 times more likely (odds ratio [OR] = 3.94, 95% CI = 2.29-6.77) to contract both infections. Children between 12 and 23 months were 3 times riskier (OR = 3.08, 95% CI = 1.86-5.08) and risk doubled for those between 24 and 35 months (OR = 1.91, 95% CI = 1.11-3.29) compared with those in reference category of 0 to 6 months. Moreover, children within the middle quintile were 0.62 times less likely to develop cases (OR = 0.62, 95% CI = 0.43-0.89), while those in the highest quintile were most protected (OR = 0.42, 95% CI = 0.26-0.69) compared with children from the poorest households in the population. Younger caregivers had a negative association with a child’s comorbidity. Children with older caregivers were less likely to develop to cases compared with children with teenage caregivers. Specifically, children whose caregivers were 25 to 29 years old were 0.61 times less likely to develop comorbidity (OR = 0.61, 95% CI = 0.38-0.99) and those whose caregivers were 30 to 34 years old were 63% protected (OR = 0.37, 95% CI = 0.23-0.61). Compared with teenage caregivers, comorbidity was almost halved for children whose caretakers were aged 35 to 39 years (OR = 0.55, 95% CI = 0.33-0.91) and even lower for children taken care of by 40- to 44-year-olds (OR = 0.31, 95% CI = 0.16-0.62).
Bivariate Logistic Regression of Model Factors Associated With Comorbidity of Diarrhea and Acute Respiratory Infection in children <5 Years, Kenya.

Implies statistical significance with P < .05.
Children of caregivers with incomplete primary education were 1.49 times more likely to develop both ARI and diarrhea infections (OR = 1.49, 95% CI = 1.01-2.19). Furthermore, results indicate that stunting and comorbidity had a significant association with childhood comorbidity.
Stunted children were 1.42 times (OR = 1.49, 95% CI = 1.13-1.95) more likely to develop comorbidity cases than their counterparts. Table 2 shows the relationship between comorbidity and the single risk factors analyzed for diarrhea and ARI.
Adjusted Relationship Between Comorbidity and Risk Factors
Only variables that were significant in the bivariate analysis were included in the multivariate analysis. Results established that the likelihood of combined morbidity was highest among the younger children with those <6 months old used as a reference category. Probability of infection was almost doubled among children aged 24 to 35 months (adjusted odds ratio [OR] = 1.88, 95% CI = 1.09-3.26, P = .023), approximately 3 times higher for those between 12 and 23 months (aOR = 2.84, 95% CI = 1.71-4.70, P < .0001) and highest among children between the ages of 6 and 11 months (aOR = 3.48, 95% CI = 2.02-5.99, P < .0001).
Wealth quintile was also statistically significant; with reference set as the lowest/poorest quintile. It was found that the middle quintile were 0.58 times less likely to develop comorbidity cases (aOR = 0.58, 95% CI = 0.39-0.85). Children of caregivers aged 30 to 34 years old were 50% less likely to develop comorbidity (aOR = 0.49, 95% CI = 0.28-0.85) compared with those of teenage caregivers. This estimate was slightly lower among caregivers aged 40 to 44 years (aOR = 0.47, 95% CI = 0.23-0.95). In terms of the caregiver’s education, the odds were 1.66 times higher for those whose caregivers had incomplete primary education (aOR = 1.66, 95% CI = 1.11-2.50) compared with those with no education at all (Table 3).
Multivariate Logistic Regression of Model Factors Associated With Comorbidity of Diarrhea and Acute Respiratory Infection in Children <5 Years, Kenya. a

Variables that were significant in the bivariate logistic regression were included in the multivariate regression.
implies statistical significance with P < .05.
Discussion
Burden of Comorbidity by Age
From KDHS 2014 report, 9% (1582) of children under 5 years had ARI, 15% (2843) had diarrhea, and our findings confirmed that 2.2% (411) had both diarrhea and ARI at least 2 weeks preceding the survey. Figure 1 shows the morbidity for diarrhea, ARI and combined morbidity for children <5 years decreases with age.
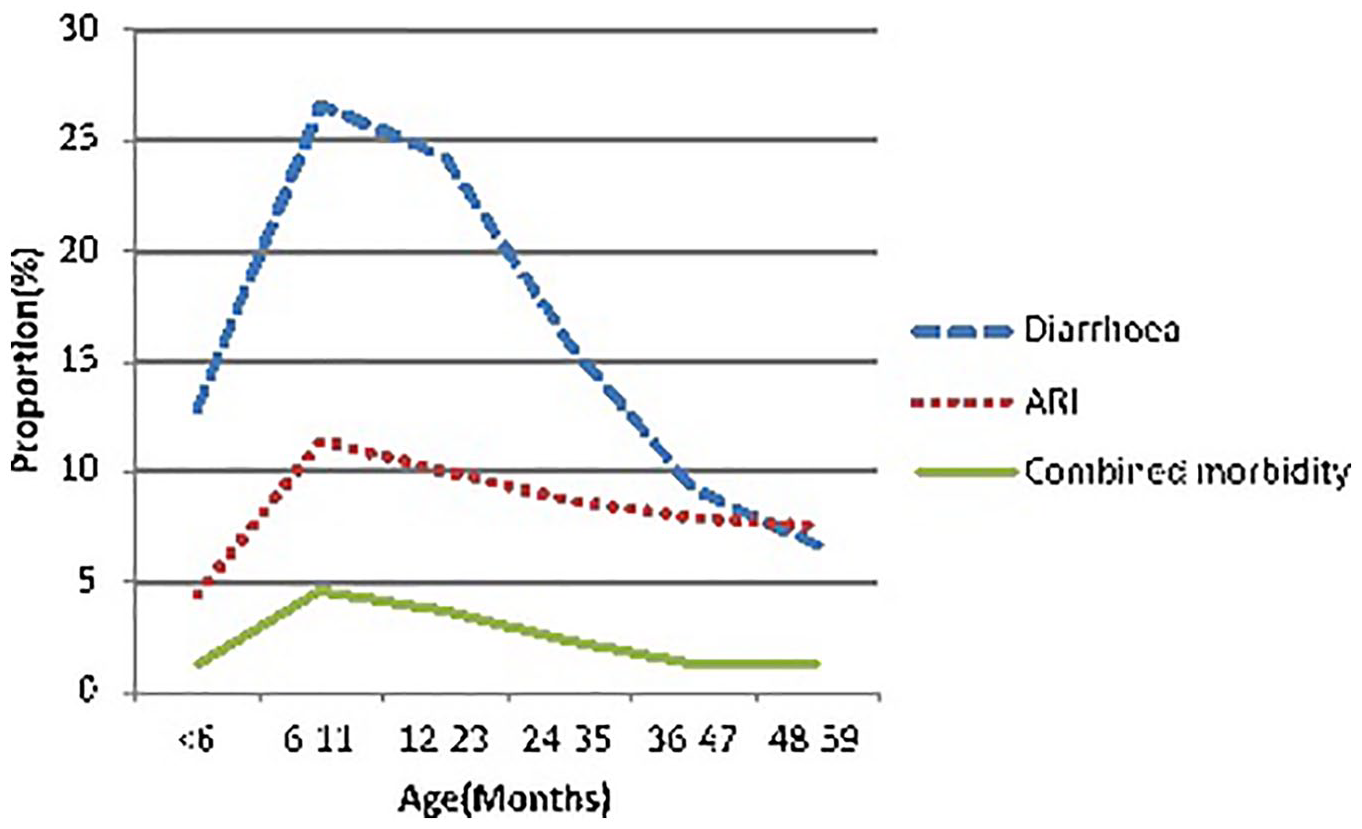
Distribution of cases of diarrhea, pneumonia, and combined morbidity in children under 5 years of age. Source: KDHS 2014.
All-cause morbidity peaks between 6 and 11 months, with diarrhea morbidity characterized by a rapid decrease with age compared with morbidity from ARI or the combined diseases. The burden of diseases is higher in younger age groups, 26.6% of children with diarrhea, 11.4% with ARI, and 4.6% with combined morbidity occurs in those between 6 and 11 months of age. Age 6 to 11 months is therefore a critical period for targeting interventions that address children vulnerabilities to both diarrhea and ARI.
Findings from this study are similar to studies conducted in India 21 and China, 22 which also found the prevalence of diarrhea to be highest among children aged 6 to 11 months. A study conducted in India 23 on the incidence, pattern, and severity of ARI in under-5 children revealed that the highest prevalence of ARI was in children less than 2 months of age. Other findings 24 revealed that combined morbidity of diarrhea and ARI was highest in children aged 12 to 23 months, which also differs from our findings.
This difference in morbidity patterns observed in different age cohorts might also be attributed to differences in culture, varied risks exposures and inherent geographical differences between the study populations.
Relationship With Malnutrition
This study also found no association between stunting and comorbidity from diarrhea and ARI. Other studies confirm a relationship between pneumonia, diarrhea, and stunting, with children exposed to prolonged acute diarrhea highly associated with stunting.3,25
Studies confirm that repeated episodes of diarrhea results in loss of nutrients, damage of the mucous membrane and a reduction in the absorptive function.26,27
Stunting interferes with lung growth increasing the odds of developing respiratory failure and making children less likely to tolerate pneumonia. 28 For children who had developed pneumonia, they were associated with incidence of stunting.29,30 A study 31 found that children who are stunted, wasted, or underweight, compared with the well-nourished are almost twice as likely to develop the bacteria Shigella whose main symptom is diarrhea. Overall, studies confirm stunting as a shared risk factor for both diarrhea and pneumonia; a contradiction to our research findings.
It is also established that ARI and diarrhea can result in stunting, which makes the association a cycle. 3 Findings by Schmidt et al 32 established that continued episodes of diarrhea could lead to acute undernutrition, which increases the chance of ARI.
Though our results show no significant relationship (P >0.05) between underweight or wasting and comorbidity, a different study found that wasting is significantly associated with prolonged diarrhea 33 and the risk of pneumonia and diarrhea is much more likely among underweight children. 34 The lack of association between underweight, wasting, stunting, and comorbidity may possibly be explained by the low statistical power imposed by the subanalysis of the KDHS 2014 survey. Stunting was identified as a significant risk (crude OR = 1.49, 95% CI = 1.13-1.95) in the bivariate analysis; however, other factors may have compounded the association in multivariate analysis. Hence, nutritional status remains as an important determinant for comorbidity and subsequent studies powered to assess comorbidity in diarrhea and ARI should be investigated.
Modeling Shared Risk Factors
Whereas this research focused on modelling a multivariable analyses to determine the shared risk factors, analysis of individual risk factors to diarrhea and ARI has been done in several studies.32,35 Only 4 factors (child age in months, wealth quintile, caregiver’s age, and caregiver’s education) were identified as shared risks to ARI and diarrhea in this study. A child’s age and nutritional status is directly related to the occurrence of ARI and diarrhea; with the youngest children(<6 months) identified as the most protected cohort probably due to breastfeeding and continuous presence of their maternal antibodies. 36 After 6 months, weaning predisposes changes on a child’s nutritional habits and with continual growth; a child’s maternal protection is weakened or lost. As the child gets older, he or she acquires natural immunity. 36
This argument can explain the elevated risks (aOR = 3.48, 95% CI = 2.02-5.99) observed between 6 and 11months and declining trend in comorbidity observed in higher age cohorts. Surprisingly, breastfeeding was also not a significant protective factor in this study. Our result contradicts previous studies,7,37 which confirmed breastfeeding as a shared risk factor to both diarrhea and ARI. A high coverage in breastfeeding and undetected small effects posed by this study design could be attributed to the lack of association observed in the results.
Children from wealthier families are less likely (aOR = 0.58, 95% CI = 0.39-0.85) to contract diarrhea and ARI than those from the poorest households. This may be explained as wealthier households tend to afford better nourishment and health care for their children. Wealthier families can also minimize their children’s exposure to risk factors like unsanitary environments and contaminated water. 36 These findings are supported by other studies which found that higher poverty level increase risk of ARI and diarrhea.38,39
Disease burden was highest in children of caregivers with limited education background, with those from caregivers with incomplete primary education more likely (aOR = 1.66, 95% CI = 1.11-2.50) to suffer infections compared to those of caregiver with no education at all. This might be attributed to the fact that caregivers with no education tend to start child bearing early so have older caregivers with more experience in preventing and managing childhood diseases taking responsibility for their children compared to caregivers with incomplete primary education who are socially considered mature nurture their families. Literacy levels may also affect the level of awareness and access to health information. 40 Even though this study did not find a significant relationship between higher level education and comorbidity, other studies found that the higher the parents’ or caregiver’s level of education, the lower the risk of getting sick for the children. 39
These study findings highlight the paucity of a nationally representative prevalence data to infer causality between investigated exposures and outcomes. More national surveys and localized prospective cohort studies with standardized data collection methods are required to allow for more effective comparisons.
Limitations
KDHS 2014 survey was carried out during the dry season (May to October). The results might have varied in the wet season since incidence of diarrhea changes from season to season. 41 There may have been slight recall bias and misclassification of diseases since cases were self-reported by the caregivers and not subject to clinical diagnosis. Cross-sectional study design has inherent time bias as both outcome and exposure were collected at the same point in time thus cannot be used to infer a causal relationship between risks and outcome. This study focuses on Kenya only, which also limit applicability or generalizability to other countries.
Conclusion
From this study, the child’s and caregiver’s age, a household’s wealth status, and education level of the caregiver were associated with comorbidity from diarrhea and ARI. We therefore recommend that implementation of programs aimed at reducing combined diarrhea and ARI in children under 5 years should focus on addressing socioeconomic barriers that limit caregivers’ access to wealth and education. Children aged between 6 and 11 months present a critical widow of opportunity to avert comorbidity from diarrhea and ARI in children under 5 years. Given that the study highlights that these 2 diseases occur together for ages 6 to 11 months, at a rate that is greater than other ages, further studies may aim to understand the immunologic and biochemical mechanisms of this relationship in relation to some children being more susceptible to sequential infections because of compromised immune functions.
Research Data
Assessing Comorbidity of Diarrhea and Acute Respiratory Infections in Children Under 5 Years: Evidence From Kenya’s Demographic Health Survey 2014
Assessing Comorbidity of Diarrhea and Acute Respiratory Infections in Children Under 5 Years: Evidence From Kenya’s Demographic Health Survey 2014 by Diana Mutuku Mulatya and Faith Wayua Mutuku in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The researchers thank Ms Alyn Achieng for helping with the data analysis and Dr Vincent Were for critically reviewing the research paper. Special thanks to the Kenya National Bureau of Statistics and ICF International for collecting the data and Measure DHS for granting data user rights.
Author Contributions
Ms Diana Mulatya developed the research proposal. She also contributed to data analysis, interpretation and finally to write-up of this manuscript. Ms Faith Mutuku was a student at University of Nairobi, working with her to review the proposal design, conducting literature review and further contributing to write-up of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors were solely responsible for funding the data analysis and development of the research article. Funding for undertaking Kenya Demographic Health Survey, 2014 was provided for by the Government of Kenya.
Ethical Approval
Ethical approval was sought from the London School of Tropical Medicine and Hygiene (LSHTM) committee. The study did not entail field-based methods and relied on secondary data that is available in the public domain. As such, local approval was not required.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.