
Abstract
The abducens nerve, which is vulnerable because of its complex anatomy at the skull base, is seldom affected by acute or severe sphenoid sinusitis. Notably, abducens nerve palsy following asymptomatic chronic rhinosinusitis (CRS) in a healthy young individual after a mild upper respiratory infection (URI) remains undocumented in the literature. Herein, we report a case of acute unilateral abducens neuropathy in a healthy 35-year-old woman with CRS in the ipsilateral sphenoid sinus, following a mild URI 2 weeks earlier. She presented with sudden-onset diplopia, was afebrile, and had normal serum inflammatory biomarkers. Comprehensive ophthalmological and neurological exams revealed no abnormalities except limited lateral gaze in the left eye. Imaging revealed mucosal swelling on the hyperpneumatized left sphenoid sinus, which thinned the clivus and positioned the inflamed mucosa close to the Dorello’s canal, likely facilitating the spread of inflammation to the ipsilateral abducens nerve. Urgent endoscopic sinus surgery combined with systemic corticosteroids and antibiotics led to complete resolution by postoperative day 10. The present case demonstrates acute abducens nerve neuropathy from URI-induced exacerbation of sphenoid sinus CRS with specific anatomical predispositions.
Keywords
Introduction
The abducens nerve, also known as cranial nerve (CN) VI, controls ipsilateral eye abduction; it is the most vulnerable of the CNs because of its anatomical characteristics.1,2 Dysfunction can occur anywhere along its path, from the pons to the lateral rectus muscle, often resulting in abducens nerve palsy. 3 In cases where an adult suddenly presents with diplopia as a result of acute-onset esotropia, it is crucial to consider abducens nerve palsy as a potential diagnosis, with microvascular disease and neoplasm as the leading causes. 4
In exceedingly rare scenarios, however, abducens nerve palsy can arise from severe, toxic acute sinusitis in the sphenoid sinus; it is also occasionally compounded by cavernous sinus thrombophlebitis, as evidenced by a few documented case reports.5–9 By contrast, chronic rhinosinusitis (CRS) can also occur solely in the sphenoid sinus. This is characterized by persistent inflammation of the sinus mucosa rather than an acute infectious process, and typically manifests as mild to moderate symptoms (or is asymptomatic in less severe cases). 10 Unlike acute severe sinusitis, abducens nerve palsy caused by asymptomatic, mild CRS in a healthy young individual has not yet been reported in the literature. Nonetheless, in patients with CRS, an acute upper respiratory tract infection (URI), such as the common cold, can acutely exacerbate the underlying chronic inflammation, thus intensifying the inflammatory burden in the sinus mucosa and potentially affecting neighboring anatomical structures.5,11–13
Herein, we present the case of a 35-year-old healthy woman who experienced sudden-onset diplopia. The diplopia was determined to result from acute, isolated left abducens nerve palsy following a recent URI in this patient, who also had isolated CRS in the ipsilateral sphenoid sinus.
Case report
The reporting of this study conforms to CARE guidelines (for CAse REports). 14
A 35-year-old healthy woman without remarkable medical history presented to the neurology department 2 days after experiencing sudden-onset diplopia that exacerbated while looking left. She also mentioned experiencing mild URI symptoms 2 weeks prior to the appointment, which had completely resolved by her visit. She reported no headaches or vision problems. The patient was afebrile with stable vital signs, a normal white blood cell count of 7,280/µL, 62.0% neutrophils, a C-reactive protein level <0.06 mg/dL, and an erythrocyte sedimentation rate of 14 mm/hour, all of which were indicative of no acute systemic infection or inflammation.
The patient was immediately admitted to the neurology department, where a comprehensive neurological examination confirmed clear consciousness and normal orientation with intact motor, sensory, reflex, and cerebellar function. However, the examination revealed an isolated abnormality in her left CN VI, although all other CN examinations were normal. Subsequently, the patient was evaluated by an ophthalmologist, who revealed a best-corrected visual acuity of 1.0 in the right eye and 0.8 in the left eye, with normal results in fundus examinations, intraocular pressure tests, and optical coherence tomography for both eyes. However, a left esotropia was detected (Figure 1), with a 5-prism diopter difference between both eyes during distant vision. The patient reported her diplopia symptoms upon gazing to the left and into the distance, along with a slight restriction in extraocular movement in the left gaze (Figure 1(a–c)). Cerebrospinal fluid and autoimmune antibody testing were normal. Computed tomography and brain magnetic resonance imaging of the head region (Figure 2) demonstrated no acute hemorrhagic, ischemic, or mass lesions. Nonetheless, a broad mucosal thickening with mucus pooling solely in the left sphenoid sinus was observed, suggesting the possibility of sinusitis in the left sphenoid sinus (Figure 2(a), (d–e)). On suspicion of a sinusitis-related abducens nerve palsy, the patient was consulted and transferred to otorhinolaryngology for further evaluation and treatment.
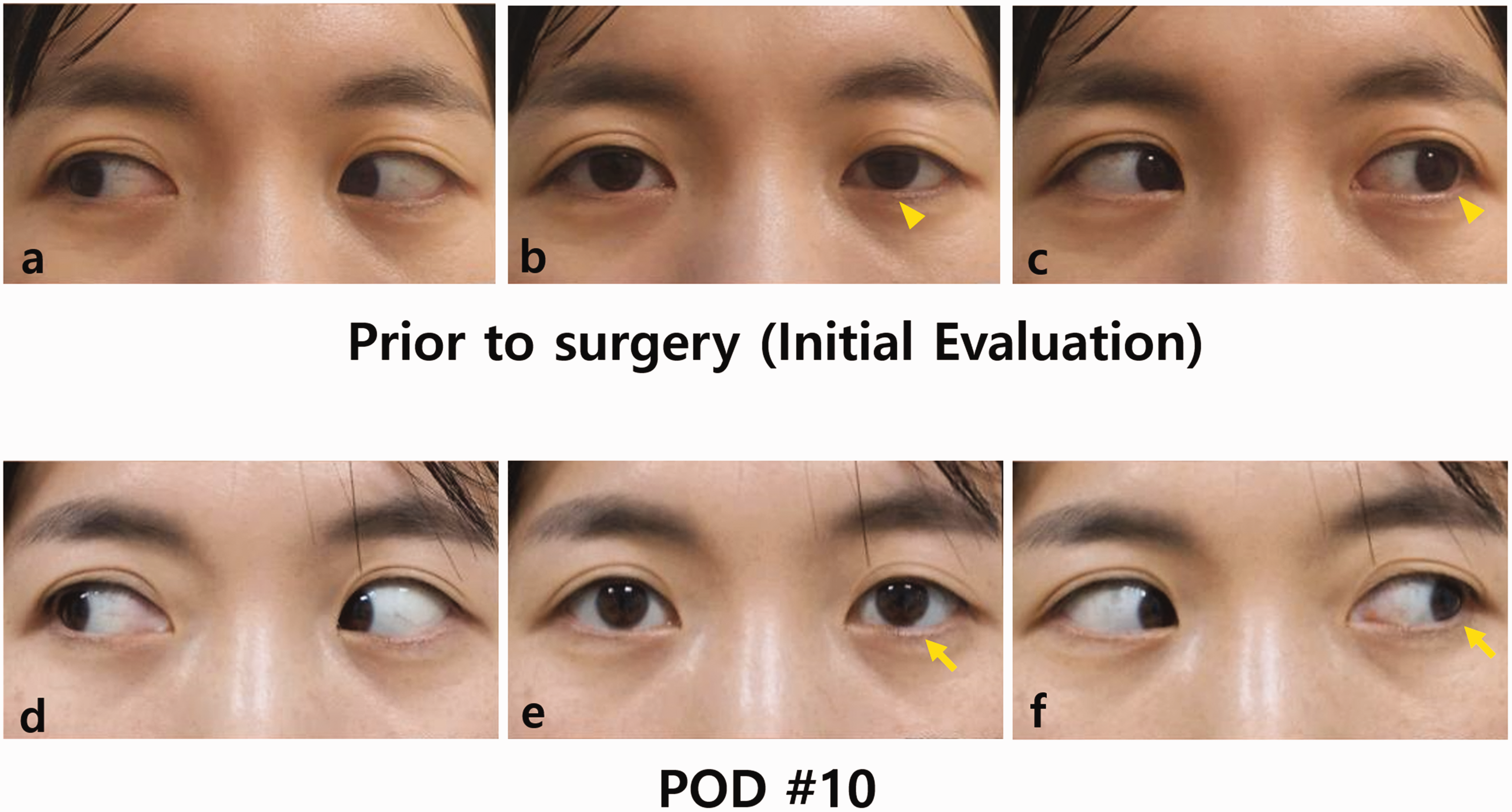
Esotropia of the left eye caused by an isolated ipsilateral chronic sphenoid sinusitis, followed by the complete resolution of the esotropia following endoscopic sinus surgery for the affected sphenoid sinus. (a–c) Esotropia of the left eye upon initial examination. Extraocular movement motion test showed normal right gaze (a); however, there was mild esotropia at rest (b; arrowhead) and a left esotropia was observed with a 5-prism diopter difference between the two eyes at distant gaze (c; arrowhead). The patient reported diplopia symptoms looking into the distance and to the left and (d–f) Complete recovery of eyeball movement on postoperative day (POD) 10. Extraocular movement motion test showed a completely normalized extraocular movement of the left eye during right gaze (d), at rest (e; arrow), and during left gaze (f; arrow).
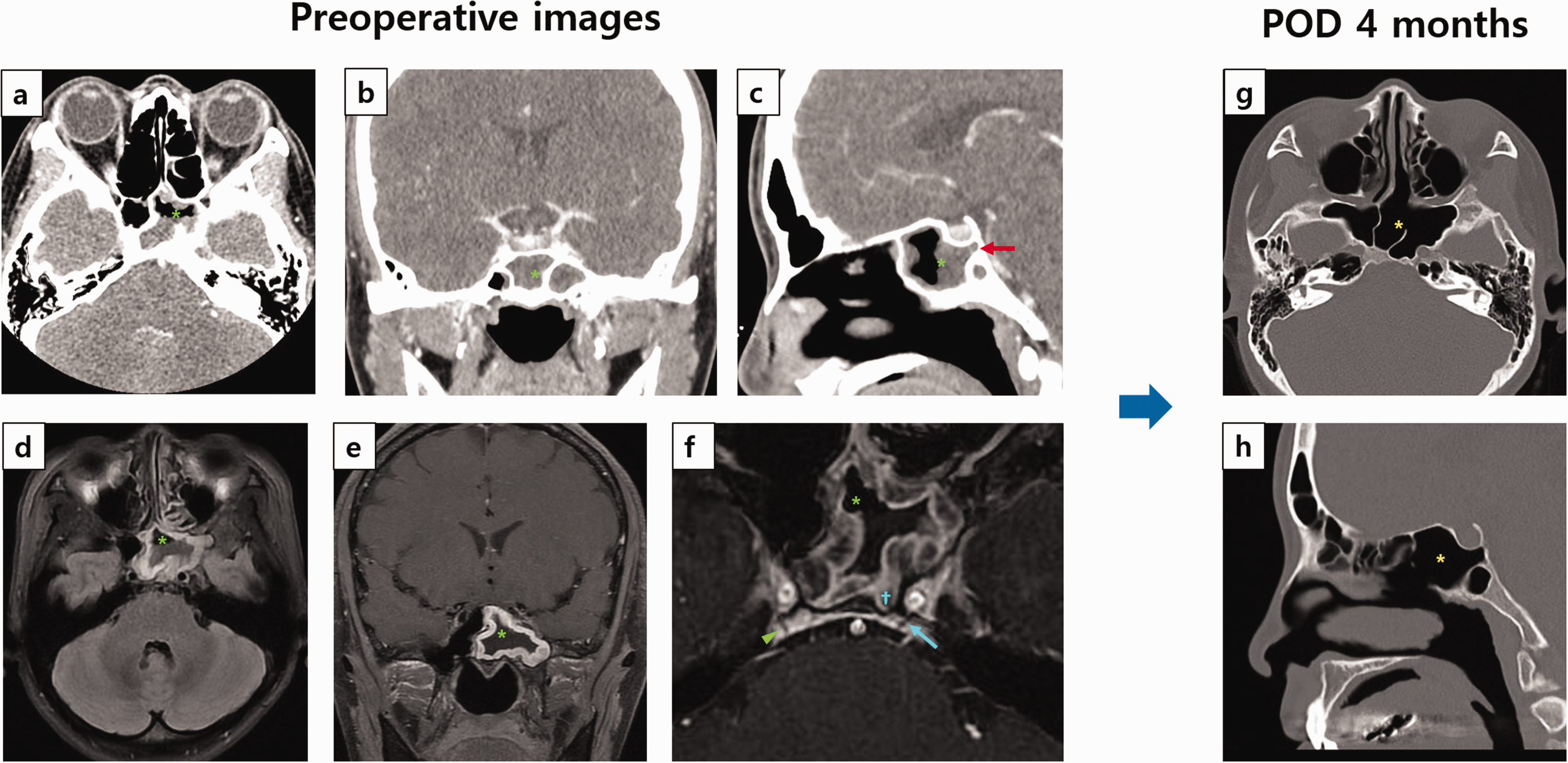
Computed tomography (CT) and magnetic resonance (MR) endoscopic imaging of a 35-year-old woman with acute diplopia and left abducens nerve palsy following a 2-week upper respiratory infection. (a–c) Contrast-enhanced sinus CT images revealed no pathologies except for diffuse mucosal thickening with air-fluid level opacity in the left sphenoid sinus, indicating sphenoid sinusitis (a–c; asterisks). The posterior wall of the sphenoid sinus was notably positioned posterior to the sella, and inferiorly reached the posterior border of the clivus (c, arrow). No enhancement or cavernous sinus widening was observed, thus ruling out acute thrombophlebitis (b). (d–f) Axial T2-weighted and coronal T1-weighted gadolinium-enhanced MR images showed mucoperiosteal thickening and air-fluid levels in the hyperpneumatized left sphenoid sinus (d–f, asterisks). (f) The distance between the left Dorello's canal and the sinus mucosa was 0.7 mm compared with 3.2 mm on the right. The obelisk indicates the most posterior part of the sphenoid sinus posterior wall, which is closest to cranial nerve (CN) VI; the arrow indicates the left CN VI within the clivus; and the arrowhead indicates the contralateral (right side) CN VI, which is further away than the ipsilateral CI VI and (g–h) post-treatment CT at 4 months shows the normalized sphenoid sinus without recurrence (asterisk).
On otorhinolaryngology examination (Figure 3), nasal endoscopy revealed no mucosal edema or discharge in the left sphenoethmoidal recess (Figure 3(a)). Radiographic imaging showed no contrast enhancement patterns or cavernous sinus widening, thus ruling out the possibility of an acute thrombophlebitis in the cavernous sinus (Figure 2(b)). However, her left sphenoid sinus was posteriorly expanded beyond the sella turcica and inferior to the level of the clivus (Figure 2(c)), bringing the left sphenoid sinus and left Dorello's canal into close proximity (Figure 2(f)). Hence, it was suspected that the inflammation triggered by the recent URI may have led to ipsilateral abducens nerve palsy through the direct propagation of inflammation.

Endoscopic sphenoid antrostomy was used to manage isolated unilateral abducens nerve palsy caused by chronic ipsilateral sphenoid sinusitis. Endoscopic sphenoidotomy involved widening the obstructed ostium of the patient's chronic rhinosinusitis-affected left sphenoid sinus, which was causing unilateral abducens nerve palsy. (a–d) The ostium was initially expanded (a) to expose and clear diffuse mucoid secretions and swollen, polypoid mucosa (b, c; arrow and asterisk). A follow-up at 4 months postoperative (POD) showed sustained widening and restored healthy mucosa in the left sphenoid sinus (d, arrowhead).
Even with the immediate administration of ceftriaxone (2 g twice daily), there was no improvement in diplopia or gaze restriction within 24 hours. An urgent endoscopic sinus surgery was therefore scheduled on hospitalization day 2. Under general anesthesia, the natural ostium of the left sphenoid sinus was identified and opened widely via transnasal sphenoid antrostomy. The patient’s left sphenoid sinus revealed no definite purulence or fungal balls, but demonstrated diffuse mucoid secretion (Figure 3(b)) along with severely swollen, polypoid mucosa (Figure 3(c)). After obtaining a bacterial swab culture and removing the collected mucus, irrigation with a mixture of ceftriaxone and dexamethasone saline were applied to the left sphenoid sinus. The polypoid sphenoid sinus wall mucosa was then sent for pathological analysis. This later revealed chronic inflammation with mild eosinophil infiltration, thus confirming the diagnosis of CRS in the left sphenoid sinus. Moreover, the bacterial culture results showed mixed growth of Staphylococcus epidermidis and Klebsiella pneumoniae, which are susceptible to oxacillin and amoxicillin, respectively.
Given that intraoperative findings revealed inflammatory changes in the affected sphenoid sinus mucosa with mucosal polyposis (rather than active suppurative or invasive fungal infection), pulse therapy 500 mg intravenous methylprednisolone once daily and 2 g intravenous ceftriaxone once daily were administered postoperatively. This treatment was accompanied by daily nasal rinsing and irrigation of postsurgical debris throughout her hospital stay.
Immediately following surgery, the patient did not show improvements in her diplopia. On postoperative day (POD) 4, the patient was discharged with oral amoxicillin-clavulanate and 30 mg prednisolone once daily for 7 days. On POD 7, the patient reported an improvement in her diplopia, although a slight restriction of extraocular muscle movement remained. In addition, the patient was given an intranasal fluticasone furoate spray with daily nasal rinsing. On POD 10, she was free of diplopia symptoms, and examination by the ophthalmologist confirmed the complete normalization of her left lateral gaze (Figure 1(d–f)). At the 4-month postoperative visit, the patient remained asymptomatic; her widened sphenoid sinus ostium was maintained and she had completely normalized healthy mucosa in the sphenoid sinus (Figures 2(g–h) and 3(d)).
Discussion
The present report describes a patient who experienced abrupt unilateral abducens nerve paralysis caused by an acute exacerbation of CRS in an excessively posteriorly aerated ipsilateral sphenoid sinus following a recent URI. Although sphenoid sinusitis typically does not lead to intracranial or orbital complications in immunocompetent individuals, it can result in important intracranial or orbital complications in some clinical scenarios.5,12 Because of its thin walls and close proximity to critical structures such as the orbital apex, cavernous sinus, and internal carotid artery, the sphenoid sinus is at risk of spreading infection or inflammation to these areas, which can result in a range of intracranial complications. 15
CRS isolated to a single sphenoid sinus is relatively uncommon, accounting for approximately 2.7% to 3.0% of all CRS cases. 10 Furthermore, sphenoid sinus lesions are often overlooked in clinical cases presenting with CN VI neuropathy, and are frequently initially misdiagnosed as primary neurological disorders.9,16 As demonstrated in the present case, if a patient presents with acute abducens nerve neuropathy, it is crucial to consider a sphenoid sinus lesion as a possible cause to achieve timely diagnostic measures and referral to an otorhinolaryngologist.6–9, 12
Our case was unique in that the patient presented with isolated dysfunction of CN VI, with no signs of severe local or systemic inflammation such as fever, headache, or polyneuropathy affecting other CNs in the cavernous sinus. The surgical and pathological findings suggested that a recent mild URI may have exacerbated the patient’s pre-existing CRS, thus causing inflammation to spread directly and resulting in abducens nerve palsy. Several previous studies have demonstrated how an acute viral URI can exacerbate inflammation in sinuses that are already compromised by CRS.11,17 Viral infections activate antiviral responses through signal transducer and activator of transcription 1/2 and nuclear factor-κB in nasal epithelial cells. This then boosts interferon and cytokine secretion and recruits innate immune cells, thereby increasing levels of interleukin-5 and -6 and eosinophil major basic protein, which in turn intensifies local type-2 immune responses and eosinophilic inflammation.11,17 In the present case, these factors likely triggered an inflammatory flare-up in the sphenoid sinus that had CRS, and the focal inflammation then spread to the nearby abducens nerve, resulting in acute neuropathy of the ipsilateral CN VI.
The abducens nerve is particularly vulnerable to injury because of its complex path through the intricate structures of the skull base.1–3 The abducens nerve emerges from the brainstem through the pontomedullary sulcus and travels laterally along the clivus.2,3 It then penetrates the clival dura and enters Dorello’s canal, an osteofibrous tunnel situated at the petroclival junction, through which the abducens nerve is transmitted from the posterior cranial fossa into the cavernous sinus.2,3 Within the cavernous sinus, the nerve runs along the inferolateral wall of the internal carotid artery, positioned medial to the ophthalmic nerve, which is embedded in the lateral (dural) wall of the sinus. The nerve then traverses the superior orbital fissure and ascends to the orbital apex.2,3
The most common causes of abducens nerve neuropathy are microvascular diseases, such as ischemic infarction and vascular compromise. 4 Nevertheless, its lengthy and complex path through the cranium, skull base, and orbit also renders it vulnerable to traumatic injuries or tumors at numerous anatomical points.1,2 Moreover, because the abducens nerve is “locked” within the bony confines of Dorello's canal at the clivus, acute inflammation of the nerve sheath can compromise its function, 2 which may explain the isolated acute CN VI neuropathy observed in our case. Interestingly, several concurrent factors likely contributed to the acute isolated CN VI palsy experienced by our patient, as follows: mild CRS in a hyperpneumatized sphenoid sinus with clival thinning brought the CN VI closer to the sphenoid sinus mucosa, and a recent URI exacerbated the inflammatory response. Supporting this hypothesis, the proximity of the left Dorello's canal to the inflamed left sphenoid sinus mucosa was only 0.7 mm—significantly less than the 3.2-mm distance on the right (Figure 2(f)).
Our case of unilateral solitary abducens nerve palsy caused by sinusitis also presented many differences from other reported instances. Typically, other cases have featured nasal symptoms (i.e., nasal discharge or postnasal drip) and severe headaches accompanied by vomiting.6–8 They have also shown elevated inflammation markers, such as erythrocyte sedimentation rate and C-reactive protein, and their radiological images have indicated lesions spreading to adjacent paranasal sinuses or acute dural inflammation.6,8 Conversely, our patient only exhibited mild URI symptoms 2 weeks prior to developing CN VI neuropathy, and this had resolved by the initial presentation; her inflammation biomarkers remained within normal ranges.
In most cases of an acute exacerbation of CRS, medical treatment is generally favored over surgery unless there are accompanying intracranial or orbital complications. 11 However, in the present case, we chose to perform a surgical intervention because the CN symptoms persisted despite 24 hours of intravenous empiric antibiotics. Our case thus illustrates a scenario in which urgent surgical intervention is recommended to evacuate and ventilate the affected sinus, even in the absence of severe acute infection symptoms. This is likely particularly important when the affected sinus is suspected to impact nearby CN function.
Conclusion
In mild CRS cases involving a posteriorly hyperpneumatized sphenoid sinus, a minor URI can trigger acute isolated abducens neuropathy, thus reflecting the complex anatomical relationship between CN VI and skull-base structures. In addition to systemic antibiotics and steroids, urgent endoscopic sinus surgery should be considered early in the treatment to drain and ventilate the afflicted sinus, as evidenced by the complete recovery of our case by POD 10.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241274587 - Supplemental material for Isolated abducens nerve palsy following upper respiratory infection in a patient with ipsilateral chronic sphenoid sinusitis
Supplemental material, sj-pdf-1-imr-10.1177_03000605241274587 for Isolated abducens nerve palsy following upper respiratory infection in a patient with ipsilateral chronic sphenoid sinusitis by Yunhyung Lee, Sung Mo Kang, Soonwook Kwon and Marn Joon Park in Journal of International Medical Research
Footnotes
Author contributions
Concept and design: Marn Joon Park, Sungmo Kang, Soonwook Kwon. Acquisition, analysis, or interpretation of data: All authors. Drafting of the manuscript: Yunhyung Lee and Marn Joon Park. Critical revision of the manuscript for important intellectual content: All authors. Administrative, technical, or material support: Yunhyung Lee. Supervision: Marn Joon Park.
Data availability statement
All relevant data are included in the manuscript. The raw clinical and image data used and analyzed in the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethics statement
The institutional review board of Inha University Hospital authorized this study (Investigation No.: 2024-01-043-000). Informed consent was obtained from the patient for both the treatment and the use of photos and case details for publication purposes.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.