
Abstract
Shared decision making (SDM) is associated with increased service satisfaction among pediatric patients. Our objective was to examine the association between SDM and service use experiences across racial/ethnic child groups. This secondary data analysis used the 2009-2010 National Survey of Children with Special Health Care Needs (CSHCN) and 2011 Pathways to Diagnosis and Services Survey. We used a rank-and-replace matching approach consistent with Institute of Medicine recommendations for health disparities research. We included CSHCN aged 6 to 17 years. The exposure of interest was parents of CSHCN reporting engagement in SDM with clinicians. There were 4032 CSHCN included in analysis. CSHCNs experiencing SDM had a 16% higher probability of reporting service use compared to those not experiencing it (95% CI, 14.24-19.42). Black children experiencing SDM reported seeing all needed care providers at a lower rate than whites (79% and 87.6% respectively; 95% CI, -14.05-3.27). The benefit of SDM over not experiencing it for blacks was 12.2% less than for whites for the outcome of seeing all needed care providers. For the outcome of receiving all needed treatments and services, the SDM benefit was 9.1% lower for Hispanics compared with whites. SDM can improve service experiences but implementation flexibility may be needed.
Keywords
Introduction
Compared with children in the general population, children with special health care needs (CSHCN) area at higher risk for physical, developmental, and emotional conditions and engage in services at a higher rate. 1 According to the Department of Health and Human Services, 15% of children in the United States (ie, about 11.2 million children) are considered to have special healthcare needs. 2 In addition, 23% of national households with children have at least 1 CSHCN. 2 Given the co-occurring needs of this population that include developmental delay (DD), intellectual disability (ID), and autism spectrum disorder (ASD), ongoing service use and strong communication between families and multiple providers are essential for the delivery of high-quality care.
Family engagement and quality communication is critical among CSHCN belonging to traditionally disenfranchised groups such as underrepresented racial and ethnic groups, those with low literacy skills, and those with language skills that are discordant with those of the health care team. Previous studies have shown that these groups experience disparities in access to evidence-based practices and lower quality of communication with service providers.3-5 The shared decision making (SDM) model has been designed to better serve high-need pediatric patients by actively involving their families in conversations with providers and in decision making to better reflect families’ values, preferences and needs in the development of treatment plans. SDM refers to the process in which both patients and their providers contribute to the medical decision-making process on an ongoing basis. 6
SDM is well suited for CSHCN as it creates opportunities for clinicians to describe treatment options and engage families in decisions about which treatment(s) best aligns with the family’s care goals, resources, and cultural beliefs. 7 A meta-analysis of SDM in the pediatric patient population found a correlation with improved health care knowledge, reduced decisional conflict and treatment outcomes. 8 SDM is associated with positive outcomes for CSHCN such as decreased health care costs, rates of hospitalization, emergency department visits, and office visits. 9 The SDM model has strong policy support as it is included in the Centers for Medicare and Medicaid Services’ Beneficiary Engagement and Incentives models, and it is endorsed by the American Academy of Pediatrics.10,11 Still, inequities remain among underrepresented CSHCN, especially among minority racial and ethnic groups. Research show these groups lack access to SDM and, once they access it, they report lower quality in their SDM experiences compared with white families.12-15
A systematic literature review showed variation in how racial and ethnic minority groups experience SDM in health care settings. 16 Reviewed studies reported that some minority patients do not feel comfortable being expected to actively engage in decision making with a clinician in the early stages of the clinical process while trust and familiarity with the particular health condition(s) were developed. 16 This evidence suggest that some minority patients differ on their decision-making preferences throughout the clinical process and these differences may be reflected on families’ report of SDM access and expected outcomes. As a result, we hypothesized that for racial and ethnic minority groups, SDM may not achieve similar outcomes as it does for white children.
This study tested this hypothesis using a national data file with a representative sample of CSHCN with cognitive and intellectual delays. We examined variation on families’ report of health care service experiences nine months after they reported experiencing SDM with clinicians. This data file also allowed the authors to control for relevant covariates at the child, family, and service levels. We followed the Institute of Medicine (IOM) definition of health disparity as “a difference in treatment provided to members of one underrepresented racial or ethnic group that is not justified by a patient’s health status or treatment preferences.” 17 We used a rank-and-replace matching approach that has been previously tested for an examination of IOM-defined disparities, while controlling for predisposing, enabling and need factors that were selected a priori and guided by the Anderson model of health care utilization.18,19 The present study also addresses a gap in the literature12,13 by empirically examining variation in SDM among racial and ethnic minority groups using a large national survey dataset.
Methods
Data Sources and Search Strategy
This was a retrospective secondary analysis of the 2009-2010 National Survey of Children with Special Health Care Needs (NS-CSHCN) and its subsequent associated 2011 Survey of Pathways to Diagnosis and Services (Pathways).20,21 The Pathways data file, a telephone-based interview survey, was conducted from February through June of 2011, an average of 9 months after the initial NS-CSHCN interview. The Pathway survey followed a sub-sample of CSHCN aged 6 to 17 years who were reported as diagnosed with DD, ID, and ASD by a health care provider in the NS-CSHCN survey. Both data files were linked using a common child identifier.
This study included a sample of 4032 children aged 6 to 17 years and participating in the NS-CSHCN and Pathways surveys. Survey results are weighted to represent the population of noninstitutionalized CSHCN ever diagnosed with DD, ID, or ASD in the United States (n = 2 091 803). The same survey respondents participated in both national surveys to provide information on the child. A total of 87% of respondents agreed to participate in the survey. 20 The NS-CSHCN was administered in English and Spanish while the Pathways survey was administered only in English. 22 Most of the respondents (80%) were the child’s mother (biological, step, foster, or adoptive), 14% were the father (biological, step, foster, or adoptive), and 6% were some other relative or guardian (hereafter all together referred to as “parents”). The overall weighted telephone interview completion rate in the Pathways survey was 62%, which combines the contact rate and the participation rate. 20
Service use experiences outcome variable was measured through the following parent-reported survey questions from the Pathways survey: (1) saw all the service providers needed to care for their developmental needs during the past 12 months and (2) received all the treatments and services necessary to meet their developmental needs during the past 12 months.
Race and ethnicity variables were drawn from the publicly released NS-CSHCN data file contains imputed data for child’s race and ethnicity. This variable had the following categories: non-Hispanic white (reference group), non-Hispanic black, Hispanic, and other-race (ie, non-Hispanic children identified by a single one of the following categories: American Indian, Alaska Native, or Native Hawaiian/Pacific Islander, or multiracial).
SDM was measured through 4 survey items: parents reported that they (1) discuss with providers a range of options to consider for their child’s treatment, (2) are encouraged to ask questions or raise concerns, (3) it is easy to ask questions or raise concerns, and (4) their health care providers consider and respect what treatment choices the parent feels would be best for child. The SDM variable was coded as one (1) if parents answered “usually” or “always” to all questions and zero (0) otherwise. This scoring of the SDM variable has been used in previous publications of studies using the NS-CSHCN survey.2,23 Parents who answered “don’t know” or “refused” to any of the 4 questions were set to missing (n = 36, 0.89%).
We selected covariates guided by the Anderson model of health care utilization. 19 Covariates included predisposing (child’s sociodemographic characteristics, including child’s age starting at 6 years old per Pathways survey criteria and health status); enabling (parent education, family income, child insurance coverage at the time of the survey, experiencing medical home concordant care, geographic region of residence); and need (child’s health status that included type and number of health conditions, number of functional difficulties, daily activity limitations) factors. The binary medical home concordant care variable was derived from 5 subcomponent measures: (1) the child had a personal doctor or nurse, (2) the child had an usual health care source, (3) family received family-centered care, (4) there were no problems getting needed referrals, and (5) the family perceived effective care coordination. The final variable was constructed as a binary measure (yes = 1; no = 0) if a CSHCN met all 5 inclusion criteria. This measure has been used in other studies examining the NS-CSHCN data. 24 We followed recommendations from the NS-CSHNC survey developers for the construction of this medical home variable. 22
Statistical Analyses
We carried out analyses using all survey respondents who completed Pathways telephone interviews. We applied the Pathways interview survey sampling weights to all analytic work to reflect the population of noninstitutionalized CSHCN aged 6 to 17 years who ever had ASD, ID, or DD in the United States (4032 Pathways sample representing a population size of 2 091 803). Complete case analysis was implemented given that variable missingness was less than 1% of the sample. We present descriptive statistics for child-family characteristics and service use experience outcomes by racial and ethnic groups. Bivariate analyses test white-minority differences and all statistical tests were conducted at the 2-tailed significance level of .05 using SAS for Windows version 9.4. 25
To examine SDM effects and racial disparities, we used the procedure SURVEYLOGISTIC to fit a multiple regression modeling each binary care receipt outcome as a logit function of race, SDM, and race by SES interactions. We included covariates to control for differences in health status and comorbid health conditions (ie, child has emotional, developmental, or behavioral health needs, daily activity limitations, number of functional difficulties), socioeconomic status (SES) variables, and race by SES interactions. For variance estimation, we applied sample design information (Pathways stratum, clusters, and weights) and used the Taylor series linearization method to account for complex survey design and potential bias resulting from survey nonresponse.
The IOM defines disparities as differences in treatment received by racial and ethnic minority groups that are not justified by the underlying health conditions or treatment preferences of these individuals. 17 In other words, it recognizes that socioeconomic differences mediate this race/ethnicity and disparity relationship. 26 To follow the IOM recommendation, a matching-based data analysis method has been implemented in health services research to adjust for health status when examining variation among population groups and it has been tested in similar areas of research.17,27 The rank-and-replace method is designed to uncover “underlying mechanisms of disparities” via adjusting for group differences in health status by transforming the entire distribution of health status for minority populations to approximate the white health status distribution.18,26-29
The rank-and-replace approach follows a multistep process. First, we computed a health-status index score for each individual by summing over the products of each health status variable value times the corresponding coefficient from the regression model solutions. Individuals were then assigned ranks based on the health status index scores within their race. Next, we replaced the health status index score of each minority individual with the equivalently ranked white individual and recalculated their predicted outcome.
The resulting predicted value was inversely transformed to obtain individual predicted probability of the service use outcomes. A minority group mean was subtracted from the average probability of the white group to obtain the white-minority disparity. The impact of SDM on racial disparities was assessed by a difference-in-difference estimator technique using robust standard errors. 30 That is, white-minority disparity of children with SDM minus white–minority disparity of children without SDM.
To account for stratified cluster sampling design, standard errors of disparities and difference-in-disparities were estimated using a bootstrapping method with 100 replicates. We used generalized estimating equation approach with a working correlation matrix structure to obtain empirical standard error estimates, then summarized results of 100 bootstrap samples for the robust standard error estimates.
Results
The study included a survey sample size of 4032, representing a US population size of 2 091 803 noninstitutionalized CSHCN aged 6 to 17 years. Over two-thirds of the study sample were male (69%) and with an average age of 11.72 years (SD = 3.06). The prevalence of current developmental conditions as reported by the child’s parent were 35.7% with DD only, 1.1% with ID only, 12.3% with ASD only, 15.4% with both DD and ASD, 15.2% with both DD and ID, 0.3% with both ASD and ID, and 7.2% with all 3 conditions.
Over half (62.6%) of the sample was non-Hispanic white, 15.7% non-Hispanic black, 12.9% Hispanic, and 8.8% non-Hispanic other. Table 1 presents comparisons of child and family characteristics by racial and ethnic group. Compared with white children, black children had lower prevalence of autism (21.1% vs 33%, P = .004), and both black and those of other racial groups had more comorbid health conditions (average of 3.8 conditions in each minority group vs 3.4 in whites, P = .02). Overall and compared with whites, black and Hispanic children had lower frequency of experiencing medical home concordant care, and their parents had fewer years of education and lower income compared with families of white children.
CSHCN Weighted Characteristics by Race/Ethnicity Group (n = 2 091 803). a
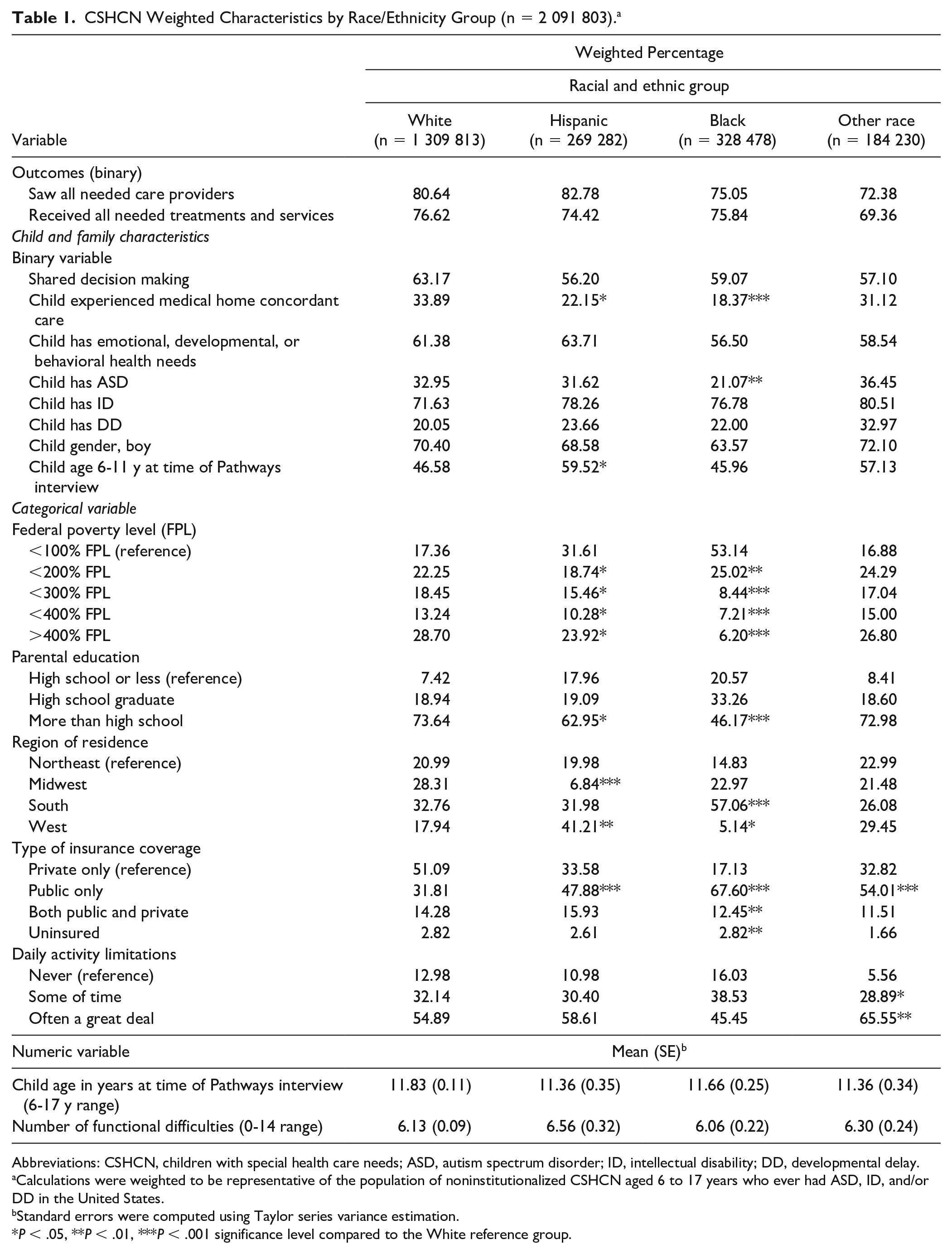
Abbreviations: CSHCN, children with special health care needs; ASD, autism spectrum disorder; ID, intellectual disability; DD, developmental delay.
Calculations were weighted to be representative of the population of noninstitutionalized CSHCN aged 6 to 17 years who ever had ASD, ID, and/or DD in the United States.
Standard errors were computed using Taylor series variance estimation.
P < .05, **P < .01, ***P < .001 significance level compared to the White reference group.
Racial and Ethnic Disparity Estimates
We present data analyses results in three stages (Table 2). First, we present estimates on the average predicted probability of service use by race and ethnicity for the entire CSHCN population. Among all children, the other race group had an 8.4% lower probability of reporting seeing all needed care providers compared to whites (P < .001), and a 7.8% lower probability of reporting that they were receiving all needed treatments and services (P < .001). Overall, children who experienced SDM had a 16% higher probability of reporting service use compared to those who did not experienced SDM for both outcome variables.
Racial and Ethnic Comparisons of Predicted Probabilities in Service Use, and Shared Decision Making (SDM) Effect.

Standard error estimates derived from 100 bootstrap samples.
Second, we present stratified results by SDM and non-SDM groups. Among children experiencing SDM, black children reported seeing all needed care providers at a lower rate than their white counterparts (79% and 87.6% respectively; P = .002). On the other hand, among children not experiencing SDM, the other race group was about 16% less than white children in both outcome variables (P < .001).
Finally, we present the overall SDM impact on service use experiences as the difference in minority-white disparities between SDM arm and non-SDM arm. The overall benefit of SDM over not experiencing it for black families was 12.2% less (P = .004) than the benefit for white families for the outcome of seeing all needed care providers. For the other-race group, the overall SDM impact was 16% higher than the benefit of SDM in whites on the outcome of seeing all needed care providers (P < .001). For the second outcome of receiving all needed treatments and services, the SDM benefit was 9.1% lower for Hispanic children compared to whites (P = .008), and 18.1% higher for the other-race group compared to whites (P < .001).
We implemented sensitivity analysis by analyzing the survey data using a traditional data analysis method of multiple logistic regression estimating race, SDM, and race by SES interactions. Overall, the results of these analyses were consistent with the results from the rank-and-replace method. See Figure 1 for a display of results from both the rank-and-replace and the logistic regression models.

White-minority disparity estimates of probabilities in receiving care by estimation methods.
Discussion
We used a nationally representative sample of CSHCN to examine the role of SDM on healthcare service experiences among racial and ethnic minority children and adolescents and compared with their white counterparts. After adjusting for SES differences and associated health status, following IOM recommendations, we found that racial and ethnic minority groups reported health care service use at a lower rate than whites. These results are consistent with existing literature reporting minority patients consistently experience lower access to needed health care services compared to whites.17,26,31-33
CSHCN require a wide array of primary and specialty care services to successfully manage their cognitive, developmental, and behavioral health conditions. Lack of access to needed care poses additional sources of stress to minority families and perpetuates health disparities, likely contributing to reported poorer health service experiences compared with their white counterparts. 33 These findings are especially troubling for CSHCNs because they need care at a higher rate than the average child, and minority families more often report receiving inadequate care. Hence and service use experiences during healthcare encounters with providers, minority CSHCN may be at highest risk for potential care quality gaps. 34
The SDM model has been designed to better serve CSHCN and help close documented disparities. It has been hailed as “the pinnacle of patient-centered care” embraced by policy makers, health care providers, and insurers. 35 In line with the literature, our study showed that a higher percentage of families who experienced SDM reported health care service use compared to those who did not experience it.8,36 These results are clinically significant as well with a 16% increase in reports of service use among CSHCN.
Despite these promising results, disparities remained for some racial and ethnic groups once we implemented subgroup analyses and controlled for predisposing, enabling and need characteristics. Results showed that SDM may be exacerbating disparities for black and Hispanic children and adolescents with special health care needs. These results seem to confirm our hypothesis that some racial and ethnic minority groups may experience decision making, within the clinical encounter, differently than their white counterparts. One possible explanation for this difference can be that some minority families may have different decision-making preferences than nonminorities due to cultural values and a history of mistrust given structural inequities within the health care system.16,37
These factors may pose more of a challenge for service providers early on in the SDM engagement process. Lack of flexibility on the timing of SDM implementation among clinicians may contribute to perceived lower SDM quality among minority groups. That is, previous research suggests preferences among some racial and ethnic minority patients for a more directive decision-making style by providers early on during the health care process, while still maintaining high-quality provider-patient communication. This gradual process, leading to a SDM style, could provide some patients with the time needed to increase trust and become more familiar with available treatment options. 16 This may be the case in this study as families who participated in the NS-CSHCN reported SDM engagement an average 9 months prior (earlier in the clinical process) to reporting health care service use experiences. The provision of a flexible approach to SDM as a way to adjust to patient needs and preferences also reflects a sense of cultural humility from the provider end. In fact, cultural humility has been referred in the literature as “key to patient/family partnerships for making difficult decisions.” 38
We recognize several limitations of this secondary data analysis study. First, data relies on self-reported experiences from parents. We are unable to confirm whether families received SDM as a formal patient-centered strategy delivered by a trained provider. In addition, we do not have information about the content and quality of the SDM process for these families. If we did, we could better elucidate whether these findings are also driven by poor quality SDM, by differences in preferences for SDM or cultural values (given that race/ethnicity is a poor proxy for culture) or by other dynamics within the medical encounter. It is also possible that the sample underrepresented non-English speaking families as the Pathways survey was completed only in English.
The data used in this study include families who reported experiencing SDM at least once before reporting on their health care service use experiences 9 months later. However, we cannot claim causality as this survey research was not a longitudinal study. We are also unable to measure continuity of care within this timeline because this information was not reassessed in the Pathways survey. Last, we found a positive relationship between SDM and health care service use for the other-race group after adjusting for covariates. This group is composed of American Indian, Alaska Native, or Native Hawaiian/Pacific Islander, or multi-racial CSHCN. Given the high heterogeneity of this other-race group, any conclusions and ability to generalize is problematic. Additional research on the impact of SDM on each of the racial subgroups included is needed. Despite these limitations, this study uses a nationally representative sample of CSHCN and their families’ accounts of SDM and service use experiences during health care encounters with providers. 39 In addition, we have adjusted for socioeconomic and medical complexity factors. These experiences allow us to examine variation in how subgroups of CSHCN experience SDM and its association with service use experiences.
This study’s results support the importance of further research to optimize SDM among racial/ethnic minority CSHCN. When health care service delivery does not meet the needs and preferences of all children and their families, especially those belonging to disenfranchised and vulnerable groups, it perpetuates inequities in access to high-quality services and the risk of poor downstream health outcomes. SDM can potentially make great strides in eliminating avoidable health care disparities by incorporating historically underrepresented minority patients’ values, expectations, and preferences throughout the decision-making process. Additional qualitative research is needed to gain a better understanding of how these factors play a role in the access, quality, and outcomes of SDM efforts across minority racial and ethnic groups over time.
Practice Implications
Our study has implications for clinical practice and results suggest that SDM is one mechanism to improve health service experiences for pediatric patients but that flexibility from clinicians may be needed on its implementation. These findings indicate that it is important for clinicians to be mindful that SDM may be experienced in different ways among some minority CSHCN and their families. Clinicians may avoid unintentionally becoming overreductive when engaging minority families in decision making by focusing on cultural humility. 40 This term is defined by Tervalon and Murray-Garcia 41 as, “a lifelong commitment to self-evaluation and self-critique, to redressing the power imbalances in the patient-clinician dynamic, and to developing mutually beneficial and non-paternalistic clinical and advocacy partnerships with communities on behalf of individuals and underserved populations.” This concept may be particularly relevant during the early stages of the clinical process as a way for clinicians to provide minority patients with the space and time to become, rather than necessarily start as, equal decision-making partners with the clinician. Customized approaches to SDM may increase accessibility and effectiveness for historically underrepresented minorities and thereby achieve greater equity in health care use.40,42
Footnotes
Acknowledgements
The authors acknowledge the valuable feedback on drafts of this manuscript provided by Kathleen Thomas, PhD, and the assistance provided by Mrs Gabrielle Jacobs.
Author Contributions
Conceptualization: Monica Perez Jolles, PhD, Leah Zullig, PhD, Gauri Kolhatkar, MD, MPHS, MS; Methodology: Perez Jolles; Formal analysis and investigation: Pey-Jiuan Lee, MS; Writing – original draft preparation: Perez Jolles; Writing – review and editing: Perez-Jolles, Zullig, Lee, Kolhatkar; Resources: Zullig; Supervision: Perez Jolles.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.