
Abstract
Introduction
In Canada, pharmacists often receive a prescription and dispense medications to patients in person, because both pharmacists’ access to electronic health records (EHRs) and medication mailing are uncommon.1,2 A 2016 report by the Canadian Pharmacists Association recommended that pharmacists be allowed access to health records to document patient information and treatment indications. 1 Previous studies have found that pharmacists with access to information in patients’ EHRs were able to identify more medication related problems. 3 However, due to concerns about confidentiality, some physicians may dislike sharing information in patients’ EHR. 4 Mail-order pharmacies (ie, pharmacies that mail medications to patients) are also relatively uncommon in Canada. 2 Studies have found that patients’ adherence to statins and diabetes medications was higher among those who received their medications by mail.5,6 However, some social assistance eligible Americans expressed concerns about delivery times when utilizing mail order pharmacies. 7
The Advisory Council on the Implementation of National Pharmacare recommended the adoption of a list of essential medications in Canada to ensure access to these medications. 8 It recommended that such medications be evidence-based and that initially a short list be implemented to ensure more timely access. 8 Other high income countries such as Sweden have adopted essential medications lists and have found high adherence to this list 15 years later. 9 Adopting a short list of medications will involve substituting patients’ medications with those on the list, when necessary.
This study aims to evaluate a pharmacy model involving pharmacist access to the EHR, medication mailing and advice over the phone that was used in a clinical trial of free essential medication distribution. The Carefully seLected and Easily Accessible at No cost Medicines (CLEAN Meds) randomized controlled trial is assessing the effects of providing free and convenient access to a short list of essential medications on adherence to medications. 10 The study sample consisted of 786 participants with half randomized to the intervention group which utilized the pharmacy model in which the pharmacist had EHR access and mailed medications to participants (medications needed immediately were dispensed in-clinic). Twenty-two participants withdrew making the final sample 764 participants. 10 To evaluate this pharmacy model, we conducted qualitative studies of participants, prescribers, and the pharmacist involved in the trial and described medication substitutions and incidents that occurred.
Methods
Participant Comments
A patient experience questionnaire was administered to participants at 9 to 12 months following enrollment in the trial and was conducted either on the phone, in person or via email, as per the participant’s preference. The questionnaire consisted of 14 yes-or-no questions with an option to leave a comment for each question, and a section which asked for additional comments. Seven questions related to the pharmacy model and asked participants about their ability to get information about their medications, whether the information given by the pharmacist changed the way they took their medication, delivery times and the condition of medications on delivery. The quantitative results of the study have been reported elsewhere. 10 In this study, we identified comments made by intervention participants to the 7 questions related to the pharmacy model and conducted thematic analysis.
Prescriber Focus Groups
As part of another study, prescribers from the rural and urban sites of the trial were recruited to participate in focus groups, which aimed to learn about their opinions of and experiences with prescribing medications from a short list of essential medications. Two focus groups were held with a total of 15 prescribers in attendance from the urban site in Toronto. One focus group was held with a total of 4 prescribers in attendance from rural sites (Assiginack and Mindemoya). All focus groups were held at St Michael’s Hospital in Toronto, Ontario.
Although no question was asked about the pharmacy model, prescribers commented about the model in all three focus groups. We summarized prescribers’ comments related to the pharmacy model.
Chart Stimulated Recall
We conducted chart stimulated recalls (CSRs) with the pharmacist utilizing a random sample of intervention participants’ charts. CSRs involve interviewing an individual about a participant encounter while viewing that participant’s medical chart to prompt the individual’s recollection of events. 11 We asked the pharmacist questions about his interactions with participants and primary care teams, use of the EHR, opinion of how care provided through this model differed from that of the regular community pharmacy (the study pharmacist has experience working in a community pharmacy) and its overall impact on patient care. We took notes and audio recorded the CSRs for later transcription and analysis. We analyzed the transcripts using inductive content analysis. 12 We read each transcript twice for familiarity and on the third reading, we coded the transcripts. These codes were then categorized into major themes. 13
Medication Substitutions
Since only a short list of essential medications were provided for free in the trial, medication substitutions were expected. We conducted chart reviews for all participants in the intervention group of the trial to determine the number of times participants’ medications were substituted, the substitutions that were made, the reasons for substitutions and the person who initiated each substitution. We included medication substitutions for the first 30 months of the trial, after which the pharmacy software changed, and data were no longer available.
Medication Incidents
We reviewed the medication incidents reported by the pharmacist for 28 months of the trial and categorized each medication incident (which caused no or temporary harm) into the following categories based on their cause: adherence, delivery, dosing, incorrect medications, interactions, miscommunication, missing medications and substitution.
Results
Participant Comments
A total of 310 (of 395, 78.5%) intervention group participants completed the survey. We identified 2 major themes from the comments: ease of obtaining information about medications and satisfaction with the delivery service. Representative quotes are presented in Table 1.
Themes, Key Concepts, and Representative Quotes From Participant Comments.
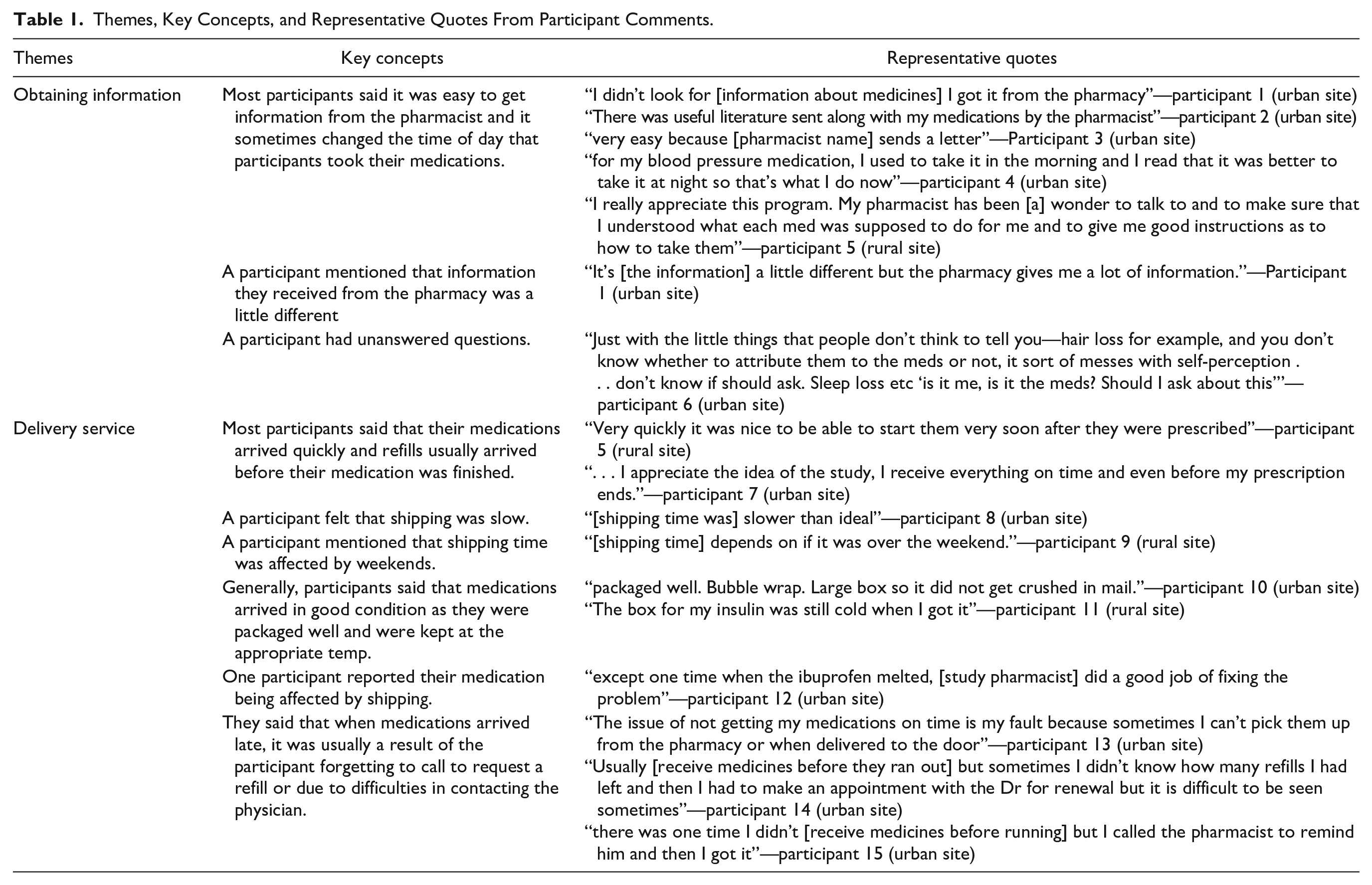
Theme 1: Obtaining Information
Most participants said that it was easy to get information from the pharmacist about their medications. However, a participant mentioned that information they received from the pharmacy was “a little different” and another participant had unanswered questions.
Theme 2: Delivery Service
Most participants said that their medications arrived quickly, and refills usually arrived before their medication was finished. However, a participant felt that shipping was slower than preferred, and another mentioned that sometimes, delivery was interrupted on weekends.
Generally, participants said that medications arrived in good condition as they were packaged well and were kept at the appropriate temperature. However, one participant reported that their medication appeared “melted” on receipt. Participants said that when medications arrived late, it was usually a result of the participant forgetting to call to request a refill or due to difficulties in contacting the prescriber.
Prescribers Focus Groups
Most often, prescribers commented on the pharmacy model when asked about their initial concerns regarding prescribing from only a short list of medications, and when asked about the instances of medication substitution. These comments reflected prescribers’ thoughts that allowing the pharmacist access to a participant’s health record was very helpful and they welcomed suggestions from the pharmacist regarding alternative medications to prescribe. A prescriber also mentioned that having medications mailed to participants’ homes was another important aspect of this pharmacy model as it helped to increase participants’ access to medications. Representative quotes are presented in Table 2.
Theme, Key Concepts, and Representative Quotes From Prescribers’ Focus Groups.

Chart Stimulated Recall
Saturation of themes was reached after 30 chart reviews. The 2 major themes identified were that this pharmacy model allowed for improved drug therapy management and participant experience, and that it made pharmacy services more accessible to participants engaged with the study. Representative quotes are presented in Table 3.
Themes, Key Concepts, and Representative Quotes From Chart Stimulated Recalls (CSRs) With the Study Pharmacist.
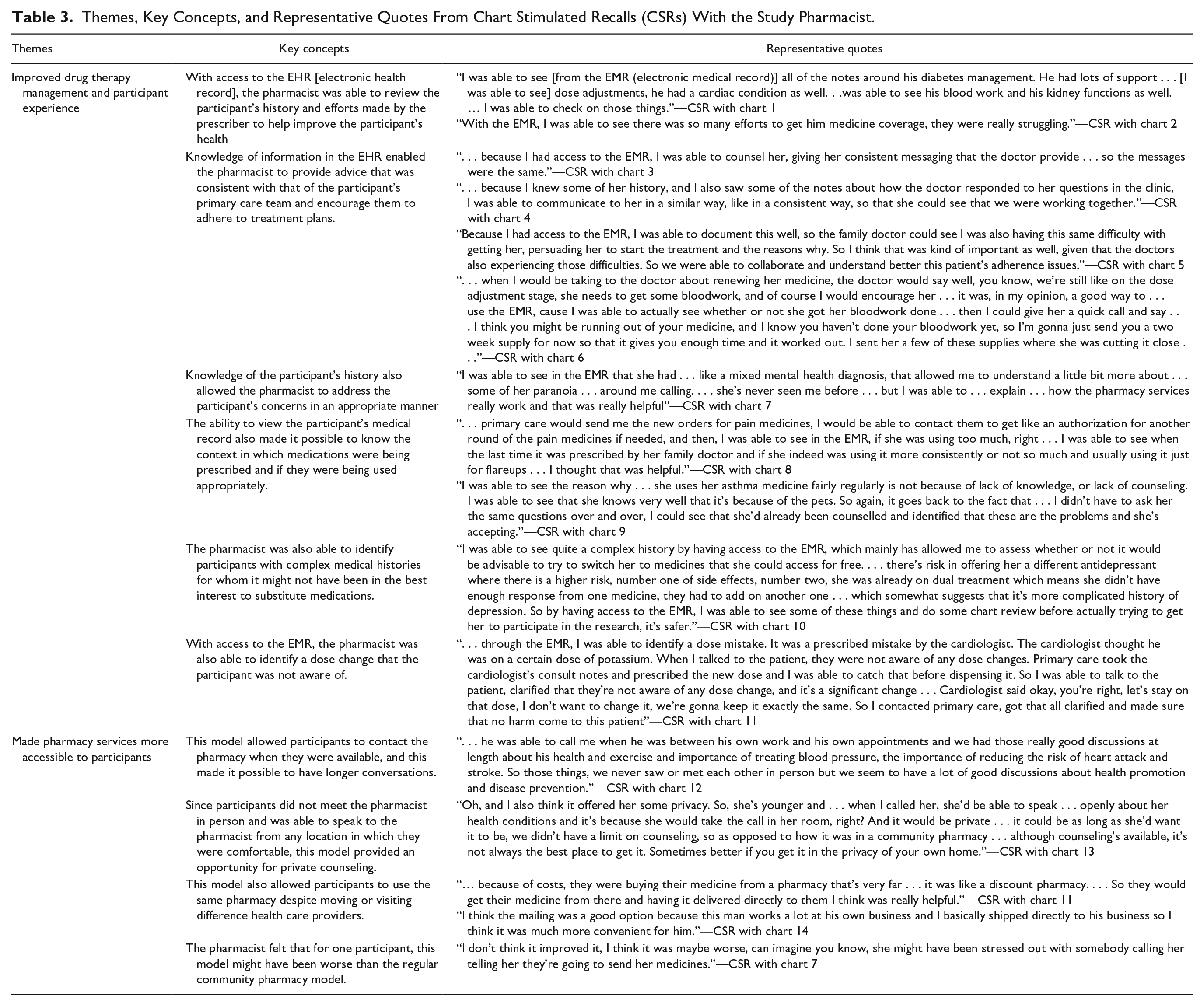
Theme 1: Improved Drug Therapy Management and Participant Experience
With access to the EHR, the pharmacist was able to review participants’ medical histories and see prescribers’ efforts to help improve the participant’s health, such as efforts to support medication coverage. With this information, the pharmacist was able to provide advice to the participant that was consistent with that of their primary care team and encourage participants to adhere to treatment plans. For example, the pharmacist encouraged participants to complete diagnostic tests, such as bloodwork, as this information was available in the EHR (see Table 3 for quotes). Knowledge of the participant’s complete primary care medical history, including mental health status, allowed the pharmacist to understand and address the participant’s concerns in an appropriate manner.
Access to the participant’s EHR made it possible to know the context in which medications were being prescribed and if they were being used appropriately, such as if pain medications were being prescribed frequently. The pharmacist was also able to identify participants with complex medical histories, including those using multiple antidepressants, for whom it might not have been in the best interest to switch medications. The ability to review participant’s current and previous medications in the EHR allowed the pharmacist to identify a dose change, of which the participant was unaware.
Theme 2: Made Pharmacy Services More Accessible to Participants
The pharmacist said that it was easy to contact most participants by telephone. The responses indicate that this model made pharmacy services more accessible to participants by allowing flexible timing for communications and enhanced privacy. In some cases, this pharmacy model served as a consistent source of heath care advice despite visiting different health care providers.
For one participant, this model might have been worse than the regular community pharmacy model as the lack of physical interaction might have made the participant anxious.
Medication Substitutions
A total of 395 participants were enrolled in the intervention group of the trial. Nine participants withdrew consent; 386 participants were included in this study. We found that 163 unique substitutions occurred a total of 380 times.
Medication substitutions were initiated by the study pharmacist (292, 76.8%), doctor (32, 8.4%), participant (19, 5%), nurse practitioner (7, 1.8%), or other members of the health care team (2, 0.5%). A total of 28 (7.4%) substitutions were initiated jointly by the pharmacist, participant, doctor or nurse practitioner. About 60% of the substitutions (226) occurred on enrollment in the study (Table 4) and 85% (322) were from a medication not on the essential medications list (i.e. not provided for free in the trial) to one that was.
The Frequency of Medication Substitutions at Different Times in the Trial.

Medication Incidents
Thirty participants experienced a total of 38 unique medication incidents.
Most incidents related to problems with delivery (16) and were mainly due to closures on weekends or holidays, delivery not completed as scheduled and difficulties in locating the participant’s address. These incidents affected a total of 13 participants, and 6 of these incidents contributed to or resulted in temporary harm.
Most incidents relating to adherence (12) resulted from either delivery problems, participants not taking medications as prescribed, or miscommunication between participants, prescribers and the pharmacist. These affected a total of 11 participants and temporary harm was reported in 4 incidents.
Seven incidents occurred in which participants received an incorrect dosage of a medication and these affected 6 participants. Most often, these incidents resulted from participants taking a higher dose than prescribed or being prescribed a dose lower than what they previously used. One incident caused temporary harm as the participant took a “double dose” of a combination medication and experienced side effects related to receiving a dose higher than recommended for one of the medications.
Miscommunication between participants, prescribers and the pharmacist caused 5 medication incidents, and affected 5 participants. One of these incidents resulted in temporary harm as the intervention group participant stopped taking some medications due to costs, since they did not receive on-list medications from the research pharmacy. There were 4 incidents involving 4 unique participants who were not able to locate their medications, none of which resulted in temporary harm.
In both incidents relating to substitution, participants reported that they were harmed temporarily as they experienced side effects after switching from a medication that is not on the list to one that is. In the interaction incident, the pharmacist identified interactions between a newly prescribed medication and a medication the participant was taking. In the incorrect medication incident, the wrong brand of glucometer testing strips was sent to the participant. Harm was not reported in the interaction nor incorrect medication incident.
Discussion
Pharmacist access to EHR information facilitated collaborative care with prescribers according to prescribers and the study pharmacist, especially around medication substitutions. This was supported by participants who found it easier to obtain information about their medications through this model. Participants were pleased to receive medications in the mail and problems with delivery were rare and usually not associated with any delays in treatment or harms. We also found that the pharmacist utilized the EHR to suggest and coordinate medication substitutions with primary care. This supports the finding from our analysis of the medication substitutions, which indicated that most were initiated by the pharmacist. Eighty-five percent of substitutions (322) were from a medication not on the essential medications list to one that was, and this was the result of providing free access to only a short list of essential medications.
Our finding that the study pharmacist used the EHR to help ensure the rational use of medications is consistent with the results of a randomized controlled trial which found that intervention group community pharmacists who were allowed access to patients’ health records identified significantly more medication related problems and omissions in preventative care than control pharmacists without access to patient’s health records. 3 Other studies conducted with physicians and family medicine graduates in Canada found that they thought that patient information (and preferably information in the EHR) should be shared across care settings and they supported sharing information with community pharmacists, respectively.14,15 We found that participants were satisfied with medication deliveries and this is also consistent with a study done with the Veterans Administration Consolidated Mail-Order Pharmacy system, which found that 88% of patients felt that their medications almost always or usually arrived on time. 16 Since this pharmacy model provided the pharmacist access to information to determine appropriate medication substitutions, wide adoption of this pharmacy model might facilitate implementation of a formulary consisting of only a short list of essential medications.
Limitations
Since the patient experience questionnaire was administered as part of the trial and without the specific aim to learn about patients’ experiences with this novel pharmacy model, these results may not be representative of all participants’ impressions. The focus groups with prescribers were also conducted for a study with a different aim and so, the results reported here may also not represent all prescribers’ impressions. We were also not able to compare comments made by patients and prescribers who utilized this pharmacy model with those who did not. Since there was only 1 study pharmacist in the trial, the chart stimulated recalls were done with the same pharmacist and there is possibility for recall bias. Due to the qualitative nature of the patient experience questionnaire, prescriber focus groups and chart stimulated recalls, our position may have influenced these components and results, although we also provide quantitative information about medication substitutions and incidents.
Conclusion
A pharmacy model that provided the pharmacist access to patients’ EHRs and mailed medications to participants allowed the pharmacist and prescribers to collaborate in prescribing appropriate medications. This model also improved participants’ access to pharmacy services and was supported by participants and prescribers. Future work should aim to explicitly determine acceptance of this model to a wider population and examine the financial implications of this model, if adopted on a broader scale.
Footnotes
Author Contributions
MZA gathered and interpreted the data, wrote the first draft of the manuscript and contributed to revisions of the manuscript. NP designed the study, interpreted the data and contributed to revisions of the manuscript. NU gathered the data and contributed to revisions of the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NP reports grants from Canadian Institutes for Health Research, the Ontario SPOR Support Unit, the Canada Research Chairs program and Physicians Services Incorporated during the conduct of the study. All other authors (MZA, NU) declare that they have no competing interests.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Keenan Research Summer Student Program.