
Abstract
Background:
Previous publications have demonstrated the benefits of pharmacist involvement in hypertension management, including in rural health care settings. Unlike many of the previous studies that evaluated pharmacist interventions occurring in collaboration with physicians, this study uniquely assessed the impact of pharmacist-led interventions under a collaborative practice agreement (CPA) on hypertension outcomes in a rural, medically underserved federally qualified health center (FQHC) in the southeastern U.S.
Objectives:
To evaluate the effectiveness of direct pharmacist intervention under a CPA compared to physician-only standard care in achieving blood pressure (BP) control. Secondary outcomes included all-cause hospitalization rates and adherence to antihypertensive medications.
Methods:
This retrospective, single-center observational study included adult patients with hypertension seen by either a clinical pharmacist or a primary care provider over a 3-month period. Primary outcomes were the proportion of patients reaching target systolic and/or diastolic BP and the median time in days to control. Secondary outcomes included all-cause hospitalizations and changes in antihypertensive medication adherence, measured by proportion of days covered (PDC).
Results:
Among 159 patients, those managed by pharmacists achieved significantly faster BP control (SBP: 49 days vs 182 days, P < .0001; DBP: 146 days vs 160 days, P = .0061). Combined SBP/DBP control was also achieved more quickly (160 days, P < .0001), despite higher initial BP levels. Notably, 0% of patients in the pharmacist group were hospitalized, compared to 10% in the physician-only group (P = .0065). Medication adherence improved, with average PDC rising from 72.5% to 80.2%, and 70.4% of patients reaching ≥80% adherence by study end.
Conclusions:
Pharmacist-led hypertension management under a CPA significantly improves BP control, time to goal, medication adherence, and reduces hospitalizations compared to physician-only care in a rural, underserved FQHC setting.
Key Points
Pharmacist interventions in community and ambulatory care settings improve blood pressure.
Pharmacist intervention under a collaborative practice agreement in a federally qualified health center in a rural and medically underserved community significantly improves time to achievement of blood pressure control and is associated with significantly fewer hospitalizations compared to standard of care
Background
Hypertension is defined by the American Heart Association (AHA) as a condition when the systolic blood pressure (SBP) is consistently greater than or equal to 130 mmHg and/or the diastolic blood pressure (DBP) is consistently greater than or equal to 90 mmHg. 1 Hypertension is known as a “silent killer,” as there are often no obvious symptoms of hypertension, yet severe and life-threatening cardiovascular events, such as myocardial infarction, stroke, and death can occur. 1 Rural and underserved populations have an increased likelihood of developing hypertension, increasing their risk of cardiovascular events. 2 This increased risk of both hypertension and its subsequent events can be attributed to limited healthcare access in rural and underserved areas. 2
Given the increasing workloads placed on primary care physicians, pharmacists are well positioned to take on a greater role in the management of chronic disease. Research has demonstrated the effectiveness of pharmacist-provided disease management activities, including hypertension. A 2025 systematic review and meta-analysis of randomized controlled trials evaluating pharmacist delivery of hypertension care services included 95 studies published between 1973 and 2023. This review and meta-analysis demonstrated statistically significant reductions in blood pressure (5.3 mmHg reduction in SBP) and improvements in blood pressure control with pharmacist care services, with the greatest improvements seen in outpatient clinics compared to community pharmacies. 3 At least 5 of the 95 studies in this meta-analysis and a few other studies not included in the meta-analysis have taken place in a rural setting, yet pharmacist-led hypertension management in federally qualified health centers in rural and medically underserved areas remains largely understudied.4 -11
Federally Qualified Health Centers (FQHCs) provide greater access to rural and underserved patient populations regardless of the ability to pay for services by utilizing a sliding fee scale and 340B pricing to provide cost-savings for the health center.12,13 FQHCs strive to promote interdisciplinary involvement among all healthcare professionals to provide the best care for their patients. 12 Some FQHCs utilize collaborative practice agreements (CPAs) to allow pharmacists to provide a higher level of care by granting the ability to perform physician-approved services. 14 Pharmacists acting under a CPA may modify medication therapies, order and evaluate laboratory tests, authorize medication refills, provide patient education, and more. The use of CPAs can help expand healthcare access and improve health outcomes, such as reducing morbidity and mortality, in rural areas by allowing pharmacists to directly manage chronic disease states, such as hypertension.
Tucker-Brown et al 4 analyzed the role of pharmacists in hypertension management in rural, primary care settings within a FQHC. The study showed high levels of engagement among clinical pharmacists, increased provider engagements, increased follow up by the subsequent referral of patients to the Hypertension Management Program (HMP) and improvements in hypertension control. 4 They concluded, “A team-based, patient-centered approach to hypertension management can be adapted for FQHCs or similar settings that serve patient populations disproportionately affected by hypertension.” 4 However, the study did not analyze the impact of direct clinical pharmacist interventions, as pharmacists in this study were required to have their clinical recommendations approved by the physicians rather than executing interventions directly under a CPA. 4
In summary, there is substantial evidence demonstrating the effectiveness of pharmacists at lowering blood pressure through clinical interventions. Several studies have evaluated rural pharmacist interventions for hypertension management.3 -11 Yet, there are limited publications describing the pharmacists’ role in hypertension management in FQHC settings in rural and medically underserved areas in the Southeastern United States where the clinical pharmacist has autonomy to practice under a CPA. This study aims to address this gap in the literature by analyzing the impact of CPA-enabled, clinical pharmacist-led hypertension interventions on the proportion of patients that achieve target BP control versus those patients receiving standard care in a rural and medically underserved federally-qualified healthcare (FQHC) setting in the Southeastern United States. Additionally, this study analyzes the impact of direct clinical pharmacist interventions on the rate of all-cause hospitalizations and adherence to antihypertensive pharmacotherapy in this population.
Objectives
This study aimed to evaluate the impact of direct clinical pharmacist intervention under a CPA on the proportion of patients that achieved blood pressure control (BP), the time to achievement of blood pressure (BP) control in days compared to physician-only, standard of care at a rural FQHC. Secondarily, this study analyzed the differences in hospitalization rates between the clinical pharmacist intervention and standard of care group and the improvement in adherence to antihypertensive medications in the PharmD group from baseline.
Methods
Following Institutional Review Board (IRB) approval, a retrospective, single-center, observational cohort study was conducted at a rural FQHC Family Medicine Clinic in a medically underserved area of the Southeast United States. Data was collected from January 1, 2024 through April 1, 2024. For patients in the clinical pharmacist intervention group, adherence was assessed using the proportion of days covered (PDC) calculated over the 6 months prior to the first pharmacist visit and compared with PDC during the active management period. Patient inclusion criteria included adults (≥18 years) with a documented diagnosis of hypertension who had at least 1 encounter with a physician and/or pharmacist during a 3-month study period. Patients were excluded if they presented with hypertensive emergency (SBP ≥180 mmHg or DBP ≥120 mmHg), recent angina or stroke in the past 6 months, renal insufficiency (CrCl <30 mL/min), pregnancy, management by a cardiologist, or impaired cognitive function such as dementia or Alzheimer’s disease. These exclusions were applied to minimize confounding variables from acute cardiovascular events, as such patients would likely require hospitalization regardless of outpatient hypertension management.
Patients were identified for study inclusion based on ICD-10 codes of hypertension and eligible patients were assigned to the clinical pharmacist intervention group if they had at least 1 PharmD clinic visit during the 3-month study period. Otherwise, they were assigned to the standard of care group. Patients in the clinical pharmacist intervention group had received adherence counseling, lifestyle modification education, and/or antihypertensive medication initiation, discontinuation, or dose adjustment under the pharmacist’s CPA. The CPA authorized pharmacists to initiate, titrate, or discontinue antihypertensive medications, order and evaluate laboratory tests, provide adherence and lifestyle counseling, and document all care in the electronic health record for physician review. Clinical pharmacists followed the same AHA/ACC guideline-directed therapy as providers in the standard of care group to ensure consistency in hypertension management. Pharmacist visits included in-clinic encounters only, and did not include telehealth, phone calls, or remote patient monitoring. Prior to any medication adjustments, 2 blood pressure and heart rate measurements were collected and the average result was documented. Pharmacists also quantified any hospitalizations that may have occurred prior to the visit. Patients assigned to the standard of care group had received hypertension management from a primary care provider without pharmacist involvement. Standard of care visits from primary care providers may or may not have specifically addressed hypertension or related medications, but hypertension was listed on the patient’s problem list for each encounter, and a clinic blood pressure measurement was collected for all included visits.
The primary endpoints of the study included: (1) the proportion of patients who achieved target SBP of less than 130 mmHg and/or DBP of less than 80 mmHg, and (2) the median time, measured in days, to achieve SBP and DBP goals. The secondary endpoints included: (1) incidence of all-cause hospitalizations during the study period, and (2) changes in medication adherence among patients in the clinical pharmacist intervention group assessed by proportion of days covered (PDC). Data was collected using a standardized data collection form by 3 of the investigators and then deidentified and provided to the biostatistician for descriptive and inferential statistical analyses.
Baseline characteristics of the patient population were summarized using means and standard deviations for continuous variables and percentages for categorical variables. Differences between the treatment groups at baseline were assessed using independent samples t-tests for continuous variables and the chi-squared (χ2) tests for categorical variables. The primary outcome, time to blood pressure control, was analyzed using the Kaplan-Meier method to estimate the median time to event for each treatment group. Differences in the time to blood pressure control between the treatment groups were compared using the log-rank test. Secondary outcomes, including hospitalization events, were analyzed using the chi-squared (χ2) tests. Fisher’s exact test was employed when expected cell counts were less than 5. Medication adherence was quantified by the Proportion of Days Covered (PDC), compared between the pre and post intervention using the paired t-test. PDC was calculated using prescription fill histories available through the internal 340B community pharmacy management system. Standard of care patients often filled prescriptions externally, and consistent fill history was not accessible, limiting comparison across groups. The proportion of patients achieving 80% adherence was compared pre and post intervention using McNemar’s test.
Results
A total of 159 patients met the inclusion criteria and were included in the final analysis. Patients meeting exclusion criteria were automatically excluded using predefined parameters in the EHR prior to cohort identification. Seventy-nine patients received clinical pharmacist interventions, and 80 patients received standard care from a primary care provider (PCP). Baseline demographic and clinical characteristics of the 2 groups are summarized below in Table 1. Patients in both groups had similar age, renal function, and comorbidities based on their Charlson Comorbidity Index scores. The clinical pharmacist intervention group had significantly higher baseline systolic (147.1 mmHg vs 137 mmHg, P = .001) and diastolic (90.4 mmHg vs 83 mmHg, P = .001) blood pressures indicating a greater degree of uncontrolled hypertension.
Baseline Characteristics of Study Participants.

Abbreviations: DBP, diastolic blood pressure; SBP, systolic blood pressure.
The clinical pharmacist intervention group achieved SBP control significantly faster than the standard of care group. The median time in days to achieve a SBP <130 mmHg was 49 days in the clinical pharmacist intervention group compared to 182 days in the standard of care group despite having higher initial blood pressure readings (P < .0001). The clinical pharmacist intervention group also achieved DBP control (<80 mmHg) significantly faster than the standard of care group (146 days vs 160 days; P = .00061). By day 160, counting from the first patient encounter within the study window, 50% of the patients in the clinical pharmacist intervention group had achieved both SBP and DBP goals (<130/80 mmHg) while no patients in the standard of care group reached both SBP and DBP control during our study period (P < .0001). All primary endpoints are outlined in Table 2 below.
Primary Outcomes.
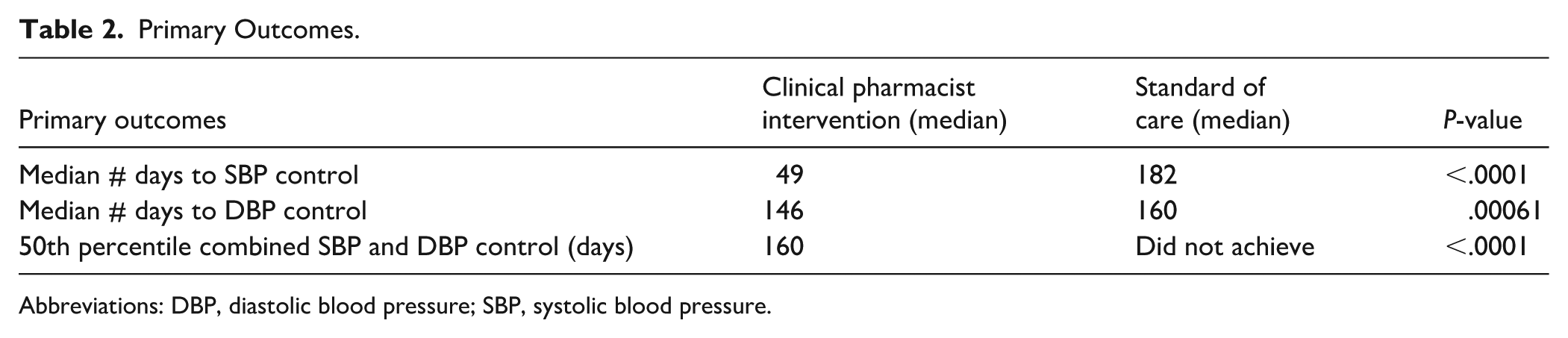
Abbreviations: DBP, diastolic blood pressure; SBP, systolic blood pressure.
With regard to secondary outcomes, there were no hospitalizations among patients in the PharmD group during the study period. However, 10% (n = 8 total, 3 cardiovascular-related) of patients in the standard of care group required hospitalizations during the study period (P = .0065). This suggests a potential clinical benefit associated with pharmacist engagement in chronic disease state management. Within the clinical pharmacist intervention group, the average PDC improved from 72.5% at baseline to 80.2% following clinical pharmacist intervention (P = .057). By study completion, 70.4% of patients in the clinical pharmacist intervention group achieved a PDC ≥80%. As PDC data was not consistently available for patients in the standard of care group, direct between-group comparisons were not feasible. Secondary outcomes are outlined in Table 3.
Secondary Outcomes.
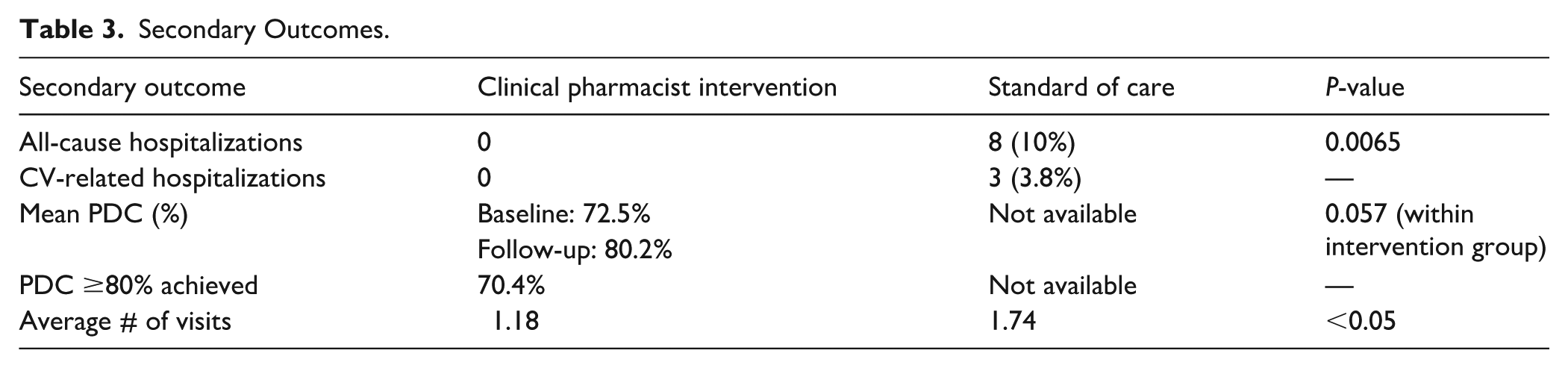
The most common pharmacist-led interventions included adherence counseling (48.1%) and medication initiation (32.9%) as allowed under the CPA. Other pharmacist-led interventions included hypertension medication dose increase (10.1%), hypertension medication dose decrease (7.6%), and hypertension medication discontinuation (15.2%). Of note, on average clinical pharmacist intervention patients received 1.18 PharmD visits, whereas the average standard of care patient received 1.74 visits with a PCP.
Discussion
Among patients that received hypertension management, those who received clinical pharmacist interventions provided under a CPA had statistically significantly shorter time to achievement of systolic, diastolic, and combinated blood pressure control than those who only received physician-managed, standard care for hypertension. There were no hospitalizations in the clinical pharmacist intervention group and antihypertensive medication adherence rates were improved, as demonstrated by an 8% increase in PDC.
The findings of our study show that clinical pharmacists are qualified to provide care to complex patient characteristics, as shown by the patients in the clinical pharmacist intervention group having a higher Charlson Comorbidity Index score indicative of a higher comorbid disease burden at baseline. In fact, despite patients in the PharmD invention group having higher SBP and DBP at baseline, pharmacist inventions were still able to provide a quicker time to achieve both SBP and DBP control, prevent hospitalizations, and improve antihypertensive medication adherence with a lower average number of clinic visits compared to those receiving standard care. This may reflect more focused hypertension management during pharmacist encounters, as opposed to standard of care visits where multiple comorbidities may have been addressed. This finding suggests pharmacists were able to achieve target blood pressure control in less total visits compared to physicians, potentially improving provider availability and health care access.
Because we kept our inclusion criteria broad, we anticipate that these findings would be generalizable to a typical Family Medicine FQHC population, which represents a strength of this study. Alternatively, a limitation is the retrospective nature of this study. Further, the types of specific interventions (eg, hypertension medication initiation, medication adherence counseling, etc.) provided by physicians within the standard of care group were not collected. Another limitation is that adherence data was only available for patients in the clinical pharmacist intervention group as most participants filled their medication at internal affiliated pharmacies. Because consistent PDC data could not be collected for the standard of care group, we were unable to make between-group comparisons. Instead, we focused on within-group improvement in adherence after clinical pharmacist intervention.
Many previously published studies have shown the benefits of pharmacists’ interventions for hypertension management. Several have demonstrated the same benefits in rural health care settings, but the majority of those pharmacists occurred in collaboration with physicians rather than autonomously underCPAs.4 -11 Additionally, prior to this study, the impact of clinical pharmacist-led hypertension interventions provided under a CPA on hypertension management in rural and medically underserved FQHCs in the southeastern United States was not documented. Only 1 small study describing qualitative impacts of PharmD involvement in an interprofessional team-based hypertension management program in a rural FQHC has been published. 4 Thus, our findings provide further support for implementation of CPAs to allow pharmacists to provide clinical services to patients to better manage chronic disease states, like hypertension, especially in rural and underserved areas such as those serviced by FQHCs. Due to the relative efficiency with which pharmacists were able to get their patients to SBP and/or DBP control compared to standard care, our findings also indicate a possibility that pharmacist involvement could reduce hospitalizations and have downstream benefits toward improving access to care, addressing health disparities, and bridging primary care gaps that negatively impact patients in rural and medically underserved areas.2,3 Future studies could explore the impact of telehealth, phone visits, or remote patient monitoring on outcomes, as our study included in-clinic pharmacist encounters only.
Conclusion
Direct clinical pharmacist in collaboration with physician hypertension management via a collaborative practice agreement in a rural, underserved FQHC significantly improves the percentage of patients that achieve blood pressure control, the time to blood pressure goal achievement, and the rate of all-cause hospitalizations compared to those who received standard of care physician-only hypertension management. The PDC data also suggests that clinical pharmacist-led interventions may enhance patient engagement with therapy to improve adherence. The findings of this study suggest that a pharmacist-physician collaborative practice model can be utilized to achieve optimal patient outcomes in rural and medically underserved areas with hypertension, as pharmacists can perform medication adjustments, diet and physical activity education, and encourage medication adherence.
Footnotes
Author Note
Lamb B, Floyd E, Goff J, McGee M, Owens L, Barfield R. Impact of Direct Pharmacist Intervention on Achievement of Blood Pressure Control at a Federally Qualified Health Center Within a Medically Underserved Area. Presented at American Pharmacists Association Annual Meeting. Nashville, TN, March 2025, #1016. Lamb B, Floyd E, Goff J, McGee M, Owens L, Barfield R. Impact of Direct Pharmacist Intervention on Achievement of Blood Pressure Control at a Federally Qualified Health Center Within a Medically Underserved Area. Presented at American Society of Health-System Pharmacists Midyear Meeting. New Orleans, LA, December 2024, #6-370.
Author Contributions
Maegan Lamb: conceptualization, methodology, validation, investigation, data curation, writing (original, review, & editing), and project administration; Evie C. Floyd: investigation, data curation, writing (original, review, & editing), and visualization; Reagan K. Barfield: conceptualization, methodology, supervision, and writing (original, review, & editing); Janet V. Goff: investigation, data curation, writing (original, review, & editing), and visualization; Joseph Magagnoli: formal analysis and methodology; Whitney Maxwell: writing (review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding support was provided by the South Carolina Center for Rural Primary Health Care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.