
Abstract
Keywords
Introduction
By 2050, there will be 2.1 billion older adults worldwide. 1 The functional decline in the aging population associated with physical frailty corresponds to decreasing social networks,2,3 increasing depression, 4 risk of health problems 5 and poor quality of life.2,6,7 The increasing number of older adults with medical service needs has a major impact on individual quality of life and the global economy. 8 Maintaining the health-related quality of life (HRQOL) of older adults becomes an important focus for public health policy.
Community-Dwelling Older Adults in Thailand
Nearly 20% of the Thai population are older adults (age 60 years or older) with a 10% increase projected by 2050.9,10 In Southeast Asia, Thailand has the second largest number of older adults. 11 Community-dwelling older adults (CDOAs) in Thailand are unique in that 98% live with their children or relatives. 12 A mixed method study found that Thai CDOAs are more likely to seek help from a folk healer or community health volunteers, perceive self as insignificant, and are less likely to report age-related problems. 13 A National Health Examination survey on frailty among 8195 Thai older adults found a high prevalence of frailty (22.1%), which significantly predicted the mortality rate (hazard ratio = 2.34, 95% CI 2.10-2.61, P < .001). 14 Other studies reported that the Thai CDOAs have at least one unmet need related to physical difficulty as well as a high prevalence of hypertension. 12
Under the health security project of the Ministry of Public Health, health care in Thailand has provided free of charge services to all Thais of all ages, including the elderly. The health care services are included prevention, promotion, treatment, and rehabilitation. The provision of care to older persons are focused on the convenient home health care to all level of health networks with multidisciplinary teams from community and provincial hospitals. Recently, the Ministry of Public Health has launched the project “community volunteer caregivers for the elderly,” which was the purpose of initiating the community long-term care system in Thailand. The goal is to improve the quality of life in Thai CDOAs. 15
Comprehensive Geriatric Assessment
The Comprehensive Geriatric Assessment (CGA), an assessment instrument for medical, psychological, and functional capability, is an accepted multidimensional interdisciplinary diagnosis criterion for diagnosis and management of frailty. 16 It has been developed as an integrative plan for treatment and follow-up to reduce functional decline, hospital readmission, and to improve quality of life.17,18 This present study tests this comprehensive assessment in Thai CDOAs to understand the health-related problems in a way that is compatible with other older adult studies.
The objectives of the study were to (1) explore the prevalence of, and describe the health-related problems of, older adults in rural communities in Thailand and (2) identify the factors that can influence changes in HRQOL of CDOAs.
The results of this study can inform optimized health management strategies to improve the HRQOL of CDOAs.
Methods
Study Design, Setting, and Participants
A population-based cross-sectional study was conducted from January 2016 to July 2016 at Ban Sao Hin, a subdistrict in rural Northern Thailand. This subdistrict was selected by using the simple random sampling of all sub districts in rural northern Thailand, which have similar demographic characteristics, lifestyle, health care behaviors, and socioeconomic status. Participants were eligible if they were aged 60 years or older, were able to communicate in Thai and were able to provide written informed consent.
Measurements
General and Geriatric Health Conditions
The general and geriatric health conditions of the participants were measured according to an assessment and screening form developed and validated by the Thai Ministry of Public Health. 19 There are 3 parts to this screening form. Part 1 is the assessment of the general demographic data, part 2 is the general health assessment (eg, illness, drug use, personal perception of health), and social assessment (eg, meaning of life, medical benefit, and social activities), and part 3 relates to geriatric health-related conditions that included eye health, oral health, hearing, and cardiovascular health. Other assessments included evaluations of activities of daily living using the Barthel Index, 19 fall history and falling risks using the Timed Up and Go Test (TUG) 20 and 5 times sit-to-stand 21 routine. Depression was assessed using the 2Q9Q, 19 cognitive function assessment using the MMSE (Mini-Mental State Examination) Thai 2002, 22 and screening for urinary incontinence by asking question, “Do you have urinary incontinence that disturb you activities of daily living in the last week?” (yes or no).
Health-Related Quality of Life
HRQOL of the participants was assessed by using the EQ-5D questionnaire. 23 This self-report questionnaire measured 5 domains, including mobility, self-care, usual activity, pain and discomfort, and anxiety and depression. This Thai version of this questionnaire has been validated and widely used.24-28 The results from the EQ-5D questionnaire were converted to utility value by a previously validated Thai-specific algorithm. 29
Data Collection
Researcher assistants were trained by geriatric experts and by the research team on how to use the assessments and screening forms. After the training, all research assistants passed the posttest evaluations and thus were able to collect data. After obtaining Naresuan University Institutional Review Board (NU-IRB) approval, all eligible participants were invited to Ban Sao Hin community hospital for comprehensive geriatric assessment. A total of 429 CDOAs population were recruited of whom 45 declined to participate in the study. After obtaining informed consents forms, the remaining 384 participants were paid 200 baht (6.38 USD) for their time and to cover transportation costs. The research assistants administered the questionnaires and other study assessments, which took about 1.5 hours in the primary care unit of community hospitals.
Statistical Analysis
Descriptive statistics were used to describe the participants’ characteristics. Mean and standard deviation were used when the data were normally distributed, while median and interquartile range were used to analyze abnormally distributed data. Health factors and HRQOL were correlated using Spearman rho correlation. Univariate and multiple linear regression were used to analyze the associations and prediction values of health-related factors (age, gender, education, marital status, religion, occupation, income, health care coverage, disease status, drug utilization, self-perceived health, living arrangement, caregivers, social activity, hobby, meaning of life, eye health, oral health, hearing status, cardiovascular risk, activity daily living, fall evaluation and fall risk screening, TUG, 5 times sit-to-stands, depression, MMSE, incontinence) and quality of life (EQ-5D-3L)). Health-related factors with P ≤ .01 in the univariate analyses were selected into the final model using a backward stepwise approach. All analyses were performed using STATA version 15.0.
Results
General Demographic Characteristics
The average age of the 384 participants was 70.69 ±7.59 years with an overall age range of 60 to 93 years. Women were in the majority (56.1%), and 66% of participants were married. Almost all participants (99.7%) were Buddhists. Employment statistics show 45.1% unemployed, 26.8% were farmers, and 22% were laborers or self-employed. More than 90% of participants were either uneducated or only completed primary school to 6th grade level education. With the universal health care coverage of Thailand, 90% received their health care from the Ban Sao Hin subdistrict hospital and 87% were under the Universal Coverage Scheme (UCS) provided by the Thai government (Table 1).
Demographic Characteristic of the Elderly (N = 384).

1 US dollar = 31.19 Thai baht based on data from Bank of Thailand in February 2020.
Health and Social Status
The 3 most common medical conditions reported were hypertension (64.6%), diabetes mellitus (23.2%), and osteoarthritis (22.7%). Study participants used an average of more than 2 drugs (mean 2.38, SD 1.93), of which 17% were nonprescribed drugs. Forty-four percent of the participants perceived their health status as good and 48.4% perceived their health better than others. Participation in social activities was 36.3% with 63.3% not participating in social activities outside their homes. Unsurprisingly, given Thai tradition and culture, 94.3% lived with their families or relatives and very few lived alone. Their children were their primary caregiver in 84% of cases. Nearly half of the participants (49.2%) rated “being able to live with the family” as giving meaning to their lives (Table 2).
Characteristics of Health and Social Status.
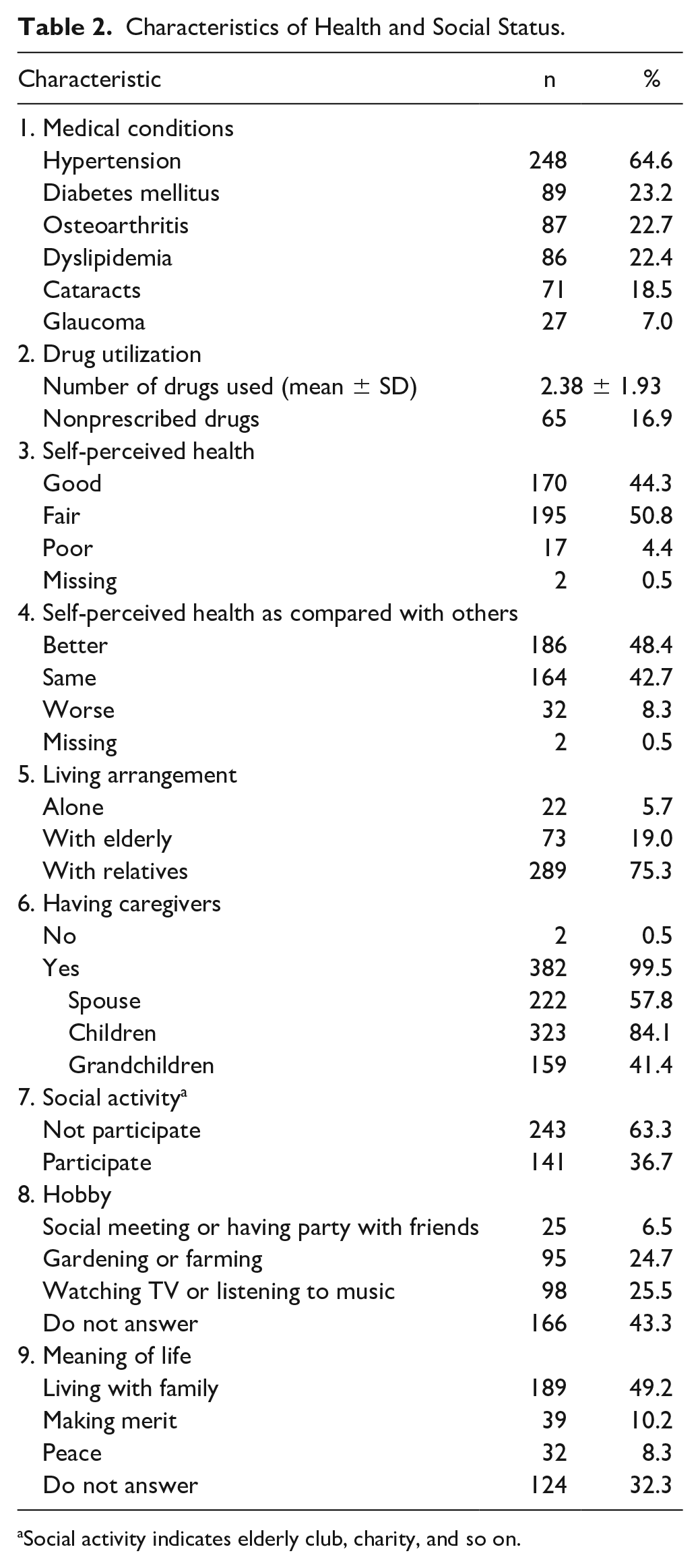
Social activity indicates elderly club, charity, and so on.
Geriatric Health-Related Conditions and Quality of Life
The vast majority of the participants were at risk of a cardiovascular condition (93.5%), and glaucoma (89.6%) and were suffering from dental carries (54.2%). Ninety-eight percent of the participants were able to perform activities of daily living independently. Twenty percent reported falls with 53% happening outside their homes. Common reasons for these falls include unstable chairs at homes (69%), physical obstructions, slippery floors, a steep slope and pets. The TUG results showed that 19% of CDOAs were at risk for falling (TUG ≥15 S), while the sit-to-stand test (≥18S) showed only 7.1% of CDOAs were at risk for falling.
Less than 10% of the participants reported depression (7.6%) and 19% were at risk of developing dementia by MMSE.
In term of quality of life, 88.8% of the participants reported no difficulty walking, 94.5% had no difficulty in self-care, with 94.5% performing usual activities (eg, work, study, housework, family, or leisure activities), and 5% reporting moderate to extreme anxiety or depression. However, 45% reported having moderate to severe pain or discomfort (Table 3).
Health Risk Assessment and Quality of Life.

Abbreviation: ADL, activities of daily living.
The Barthel ADL test. Usual activities are work, study, housework, family, or leisure activities.
The Association of Health Factors and Quality of Life
There was a significant, positive relationship between self-perceived health and HRQOL (ρ = 0.29, P < .001). Age, number of falls, and TUG were negatively associated with HRQOL (ρ = −0.19, −0.23, and −0.23, respectively, P < .001; Table 4).
The Correlation of Health and Social Factors as Well as the Quality of Life.

Based on significant P values (P < .05), only 4 health-related factors; age, history of falls, TUG, and self-perceived health were included in the multiple linear regression model, which showed that age, history of falls, TUG, and self-perceived health correlated with HQOL (Table 5).
The Analysis of Multiple Linear Regression Model for Quality of Life. a

Covariates included age, gender, disability, income, saving, hobby, social activity, exercise, house structure, body mass index, self-perceived health, underlying diseases, Timed Up and Go test, 5 times sit-to-stand, activities of daily living, depression, and Mini-Mental Status Examination.
Discussion
This study provides additional evidence that rural CDOAs suffer from multiple chronic conditions. This finding is consistent with studies from other countries.2,30-32 The most prevalent medical conditions are hypertension, diabetes mellitus, and osteoarthritis with many also suffering from glaucoma and dental issues. While other CDOAs in other countries reported 8% to 37% of dementia 33 and 14% to 63% of falls,34-36 we found a modest prevalence of dementia risks (19%) and falls (20%) in this group of participants.
Another key finding was the association between the number of falls and poor basic functional mobility, as measured by TUG. The TUG is a simple test that has been used to predict falls among community-dwelling elderly,20,37 and to assess balance and gait impairment, which are major features of frailty in the elderly. 38 The incidence of falls can lead to a state of dependency, increasing health care expenses and burden for families and communities.39,40 While other studies focused on frequency of falls, causes of falls, and fall prevention,41-43 our findings suggest that regularly monitoring of functional mobility using TUG could be another strategy for falls surveillance and prevention since this research showed that falls and TUG were associated with the quality of life in CDOAs.
In addition, our study found that among Thai CDOAs who had good self-perception of health were associated with better HRQOL, which is consistent to previous studies.44,45 However, less than half of our participants perceived their health status as “good” (44%) and were socially active (36.7%). This finding suggests the need for health policy makers to focuses on strategies that maintain social activities among older adults. These strategies may include, allowing older adults to work after retirement, extending the retirement age, promoting aged-friendly environment, and providing access to transportation.
Another interesting finding is the idea of living with the family gives most meaningful aspect of life in the older participants. Most of them (75%) lived with their relatives which nearly half (41%) were grandchildren. Grandparenting could benefit intergeneration family relationship. According to the study, 46 they found that Buddhist teachings play an important role in the way of older adults and their family reacting to their conflicts. Our study emphasizes this phenomenon. With the idea of living with the family is very meaningful in CDOAs in Thailand and their living arrangement, we suggest that family physicians can play an important role in the leadership of a comprehensive community program for Thai CDOAs since they understand their patients and families very well. Family medicine in Thailand has been established for almost 30 years. The discipline deals with the medical practice at the family level, which is the interface between individual and community medicine. 47 Additionally, the Family Care Team project was established in 2015 by the Ministry of Public Health, Thailand. 48 Family physicians is the leader of the team that includes nurse practitioners, registered nurses, social workers, and dietitians who work together to provide health care for the community. To improve HRQOL, the comprehensive health program should be initiated and continued by family physicians including vision and dental screening as well as providing resources for the family to care for the older adults at home. Future research can be done to develop and test the feasibility of the program.
This study has many strengths, including the good sample size of the CDOAs in Thailand. All data collectors were trained and required to pass the test before using the CGA to collect the data. We found that the CGA is an effective tool to examine the health status of vulnerable populations. A causal relationship cannot be drawn because of the cross-sectional nature of the design. Longitudinal research studies investigate the long-term benefit of using the CGA and examining the predicting factors of HRQOL will provide evidence that can guide HRQOL enhanced community programs. The other limitation is that this study was conducted only in rural northern Thailand. Therefore, it may not be generalized to all rural area in Thailand.
In conclusion, this study has identified a number of important health-related issues, has described the health status of the participants as a good representation of the population, and examined the factors influenced HRQOL of CDOAs in rural northern Thailand. The study provides evidence to support the need to incorporate CGA in family practice. The role of the family physician in the community can be the key to implement health policy, which should include risk of falls assessment by measuring TUG test, fall prevention, support for an aged-friendly environment for safety mobility, promoting the postponement of retirement and to have social activities outside their homes, all of which will ultimately result in a better quality of life.
Footnotes
Acknowledgements
We greatly appreciate the work, time, and effort of all the health care workers in the community, health care professionals at Naresuan University Hospital and older adults who participated in this study. We thank DrWandee Tubtim, Ms Somsri Khamphan, Ms Duangdao Wongjumpa, and Ms Warangkana Taburee for their assistance in field data collection. We would like to acknowledge the help of Dr Leorey N. Saligan from the National Institute of Nursing Research, National Institutes of Health, USA for providing scientific suggestion and directions for this manuscript. Also, we would like to thank Professor Emiritus Antonnette Graham, Department of Family Medicine at Case Western Reserve University Hospital for editing the manuscript and providing valuable feedback. In addition, we thank Mr Roy I. Morien of the Naresuan University Graduate School for his advice and effort in editing this paper for correct English grammar and English expression.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is sponsored by Naresuan University. This study is financially supported by a research grant from the Faculty of Medicine, Naresuan University, Thailand.
Ethical Approval
This study was approved by Naresuan University Institutional Review Board (IRB No. 233/58)