
Abstract
Keywords
Introduction
In 2016, 25% of newly diagnosed HIV cases (n = 39 589) in the United States were attributable to heterosexual intercourse. 1 Nationwide, Pennsylvania ranked ninth in the number of new HIV diagnoses. 1 The majority of these HIV cases occurred in Philadelphia, where significant racial and ethnic disparities in incidence are observed among heterosexuals and by sex. 2 Of 162 newly diagnosed cases in Philadelphia among this group in 2016, 56.8% occurred among women and 86.4% occurred among Black and Latinx persons. Despite heterosexual intercourse being a substantial contributor to HIV burden among people of color (POC), there are stark racial and ethnic disparities in accessing biomedical prevention methods, such as pre-exposure prophylaxis (PrEP). 3 This article estimates PrEP awareness, a critical determinant of PrEP seeking, among heterosexual POC participating in the 2016 cycle of the National HIV Behavioral Surveillance (NHBS) study in Philadelphia Metropolitan Statistical Area.
Methods
NHBS is conducted in 23 cities and territories to understand the HIV prevention needs of vulnerable populations in the United States. Recruitment methods are detailed elsewhere. 4 Briefly, a small number of seeds were incentivized to recruit members of their social and sexual networks as is typical in studies using respondent-driven sampling, a Markov chain recruitment method used to derive population-level estimates for hidden groups. Subsequent recruitment waves were conducted until the desired sample size was met. Participants received $25 for completing the study, $25 for optional HIV testing, and $10 per peer recruited (up to 5 peers).
Inclusion criteria for the NHBS include: age 18 to 60 years; ability to complete an interview in English or Spanish; possessing a valid recruitment coupon (except seeds); living in Philadelphia, Delaware, Montgomery, Bucks, and Chester Counties; reporting vaginal or anal sex with an opposite sex partner within 12 months; and living below the federal poverty level or having no more than a high school education.
Surveys measure demographic factors; engagement in prevention and health care services within 12 months (yes/no), including currently insured, having a usual source of care, any medical visit, sexually transmitted infection (STI) testing, HIV testing, and participation in HIV prevention interventions summed from “talking to a HIV prevention professional” and/or “receiving free condoms” (yes/no). HIV risk within 12 months is derived from binary items (yes/no) assessing: condomless anal or vaginal sex, 2 or more sexual partners, transactional sex, STI diagnosis (yes: to either gonorrhea or syphilis), and noninjection drug use (reported use of any: methamphetamine, crack cocaine, powder cocaine, heroin, benzodiazepines, or painkillers). For this analysis, the outcome of interest was PrEP awareness defined as yes to: “Before today, have you ever heard of people who do not have HIV taking PrEP, the antiretroviral medicine taken every day for months or years to reduce the risk of getting HIV?” This description is similar to those provided in other PrEP awareness studies.5-8
The sample for this study was restricted to POC who self-reported being HIV negative during the interview with complete data on PrEP awareness. Sample weights were created using RDS Analyst (RDS-A) to adjust for social network size and potential biases due to nonrandom recruitment (ie, due to homophily) and generate population-based estimates. χ2 tests, Wilcoxon rank-sum tests, and bivariable logistic regressions were used to assess gender differences in HIV risk behaviors, health care engagement, and PrEP awareness. Secondary analyses examined differences in accessing various types of health care between persons PrEP aware (vs not). Analyses were conducted using SAS 9.4 (Cary, NC). Procedures were approved by the City of Philadelphia and Drexel University Institutional Review Boards.
Results
The sample was comprised of 472 POC, 88.1% identified as non-Hispanic Black; the remainder identified as Hispanic/Latinx ethnicity (see Table 1). Most were currently insured (91.3%), had a usual source of health care (92.1%), and a medical visit within 12 months (87.0%). Less than 15% reported participating in some form of HIV prevention intervention, including talking with HIV prevention professional or receiving free condoms despite 78% receiving an HIV test. Far fewer received an STI screen (47.7%) and 4.1% were positive for syphilis or gonorrhea, both of which have been linked to HIV acquisition among heterosexuals. Transactional sex in the past 12 months was reported by 8.3% of our sample. Noninjection drug use was reported by 38.5% of the sample; those reporting noninjection drug use had increased odds of being men (odds ratio [OR] 2.09; 95% CI 1.23-3.58) compared with nondrug users.
Demographic, HIV Risk Behaviors, Health Care Utilization Among POC Participants in the 2016 NHBS in Philadelphia (n = 472).
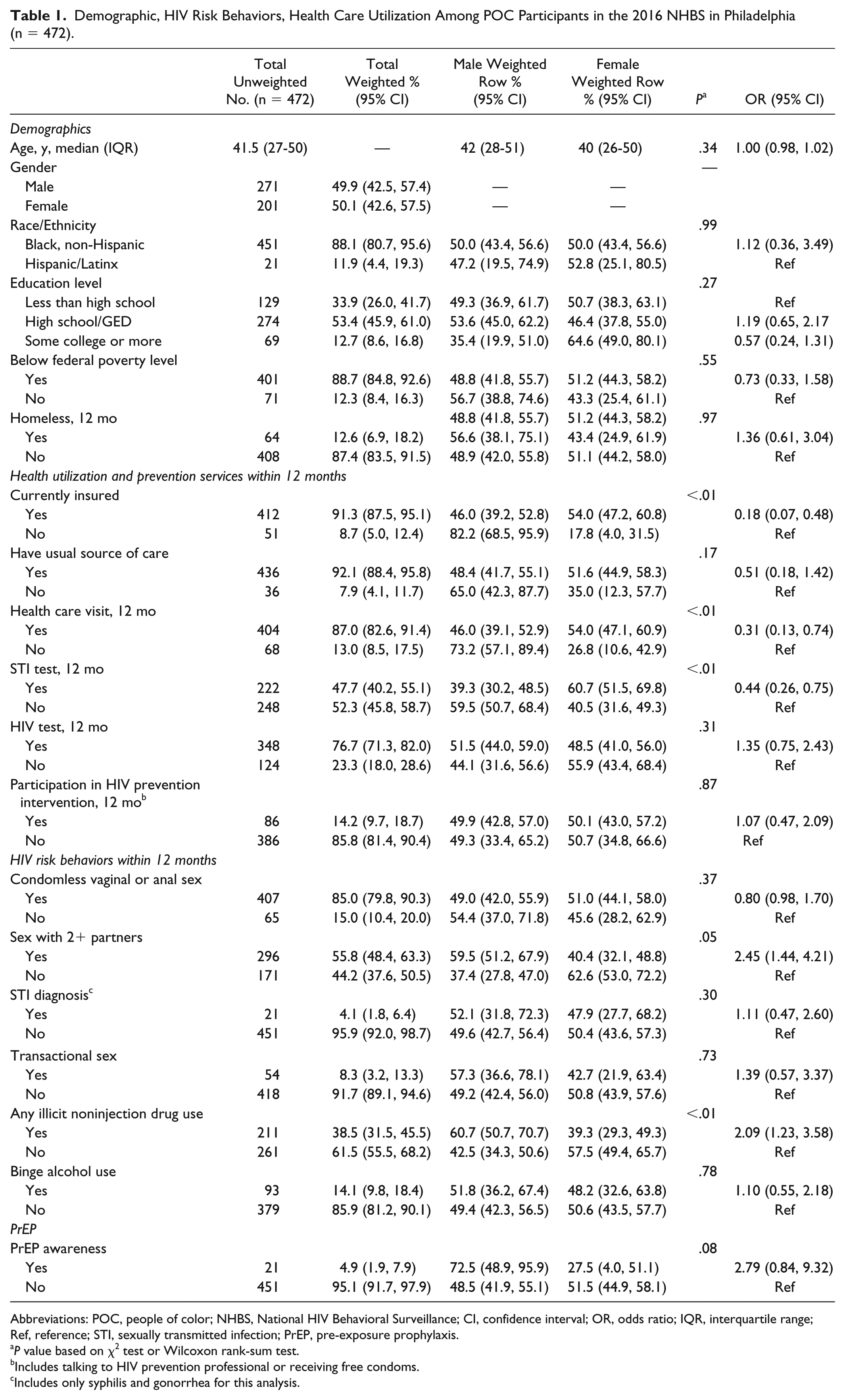
Abbreviations: POC, people of color; NHBS, National HIV Behavioral Surveillance; CI, confidence interval; OR, odds ratio; IQR, interquartile range; Ref, reference; STI, sexually transmitted infection; PrEP, pre-exposure prophylaxis.
P value based on χ2 test or Wilcoxon rank-sum test.
Includes talking to HIV prevention professional or receiving free condoms.
Includes only syphilis and gonorrhea for this analysis.
Overall, PrEP awareness was very low at 4.9% (95% CI 1.9% to 7.9%). PrEP awareness was lower among those who had a health care visit within the past 12 months compared with those who had not (OR 0.09; 95% CI 0.03-0.32) (see Table 2). PrEP awareness was also lower among those with a usual source of health care though this difference did not reach statistical significance (OR 0.41; 95% CI 0.06-2.61). The only health care variable associated with increased PrEP awareness was participation in an HIV prevention intervention (conversations with HIV prevention professional or receiving free condoms). Compared with those who had not participated, those who had participated were 5.53-fold more likely to be PrEP aware (95% CI 1.55-19.7). There was no statistical difference in PrEP awareness by gender, race/ethnicity, undergoing STI testing or receiving a diagnosis of STI positive (with gonorrhea or syphilis) within 12 months, or undergoing HIV testing within 12 months.
Health Care Utilization by PrEP Awareness Among POC Participants in the 2016 NHBS in Philadelphia (n = 472).
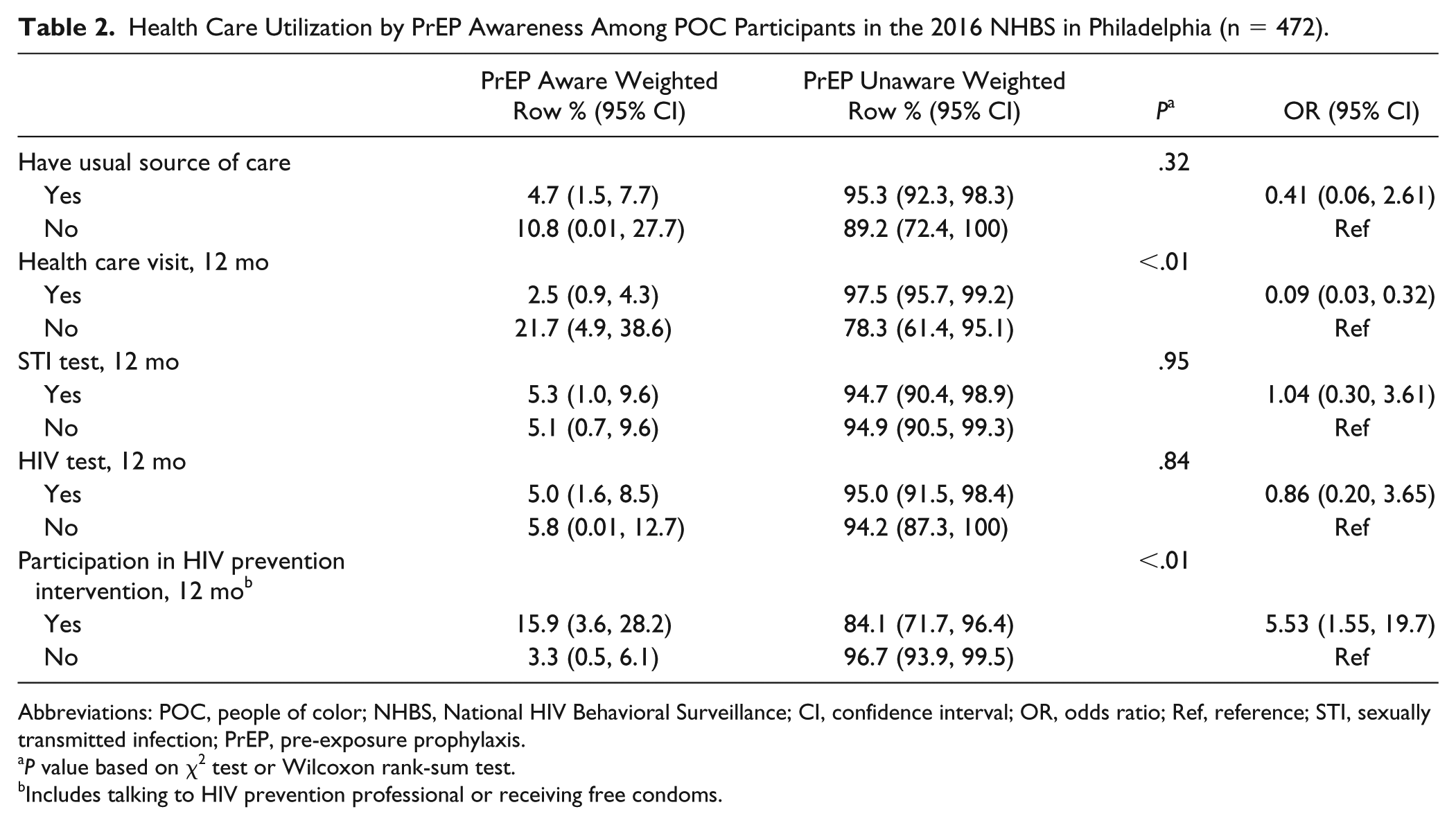
Abbreviations: POC, people of color; NHBS, National HIV Behavioral Surveillance; CI, confidence interval; OR, odds ratio; Ref, reference; STI, sexually transmitted infection; PrEP, pre-exposure prophylaxis.
P value based on χ2 test or Wilcoxon rank-sum test.
Includes talking to HIV prevention professional or receiving free condoms.
Discussion
Generally, PrEP awareness among heterosexual POC who participated in the 2016 Philadelphia NHBS was quite low and is lower than rates of awareness found in larger nationally representative studies. For example, the rate of PrEP awareness in our sample was 4.9%, which is much lower than found in a nationally representative sample of 855 Black individuals participating in an online survey in the same year (4.9% vs 14.5%). 9 Furthermore, in this same comparator study, 19.8% of high-risk individuals knew about PrEP; however, in our study, high-risk behaviors were not significantly associated with PrEP awareness, which suggests additional efforts to educate Philadelphian POC are warranted.
Importantly, the approximately 15% of POC that engaged in in HIV prevention programming were significantly more likely to be PrEP aware which is encouraging. However, it is discouraging that engagement in medical care had no impact on PrEP awareness among the 87% of the sample who had a health care visit within 12 months, some of whom screened positive for an STI. CDC clinical guidelines suggest providers counsel their high-risk patients about PrEP. 10 In this sample, the majority reported inconsistent condom use (85%), more than 2 sexual partners within 12 months (55.8%), and higher than population-level estimates for HIV-related risk behaviors (ie, STI rates in our sample [4.1%] vs national adult prevalence estimates [1.6%]). 11 This suggests 2 important findings. First, heterosexual POC in Philadelphia would benefit from being educated about PrEP in order to increase awareness about this safe, effective, and underutilized HIV prevention modality. Second, there is a disconnect between providers and POC patients when it comes to taking a sexual history, disclosing HIV risk behavior, and/or estimating HIV risk.
Failure to assess risk may be the result of providers being unaware of PrEP and relevant clinical guidelines, their discomfort with prescribing PrEP and with taking sexual history, 12 or having biases that result in a lower likelihood to prescribe PrEP to heterosexual POC.13,14 Studies have found that biases based on race and sexual orientation have an impact on provider willingness to prescribe PrEP. 14 Alternatively, it could be that patients are not disclosing HIV risk to providers. Medical mistrust, stemming from a long history of medical abuse and experimentation on Black Americans, has been well documented. 15 Ball et al 15 suggest that medical mistrust in the form of conspiracy beliefs directly affect Black Americans’ willingness to engage in HIV preventive behavior (ie, condom use) and treatment. Limited research has focused on medical mistrust and PrEP among heterosexuals. However, a recent study among Black men who have sex with men suggests that medical mistrust may affect PrEP willingness and uptake. 16
Our findings must be interpreted within the limitations of the study design. First, we relied on self-reported data with 12-month recall which are subject to social desirability and recall biases. Second, NHBS does not specifically assess patient-provider conversations about PrEP or HIV risk behavior during health care visits. We may have overestimated the missed opportunity for these conversations to occur. Third, RDS is subject to 2 main sources of bias: differential network size (eg, people are connected to networks of different sizes therefore smaller networks may be underrepresented) and nonindependence (eg, homophily or people’s tendency to belong to networks demographically similar to themselves). To account for these biases, we applied sampling weights generated from RDS-A. Fourth, our study may be underpowered because of its sample size. Finally, NHBS does not measure medical mistrust so this may not be a factor in this population. Future iterations of the NHBS could collect these data to further tease apart these relationships.
Our findings suggest PrEP messaging is not reaching heterosexual POC in Philadelphia. Using Centers for Disease Control and Prevention methods, 17 we estimate there are over 3300 heterosexuals in Philadelphia who have a PrEP indication, of whom 78% are Black and 15% are Latinx compared with 4% who are White. 2 Given this, it seems that additional PrEP promotional efforts tailored to heterosexual POC are warranted. A recent cost effectiveness study indicated that primary prevention interventions for heterosexuals are best suited to primary care settings. 18 Thus, interventions that encourage providers to follow PrEP guidelines with patients of color are encouraged.
Footnotes
Acknowledgements
We would like to thank the staff at the Philadelphia Department of Public Health who were involved in data collection, including Nicole Bundy, Rafael Melecio, Dolicia Dobbs, and Jen Shinefeld.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded through a cooperative agreement between the Philadelphia Health Department, AIDS Activities Coordinating Office, and the Centers for Disease Control and Prevention, 6NU62PS005088. Support for Dr Roth and N. K. Tran was provided through a career development award from the American Sexually Transmitted Diseases Association.