
Abstract
Introduction
Recently, the hospitalist profession marked their 20th anniversary. More than 50 000 physicians in the United States identify as hospitalists, making it the largest subspecialty in internal medicine.1,2 Hospitalists now practice in 75% of hospitals across the United States. 1 The tremendous growth of the specialty was driven by both economic factors and a large pool of internists primarily trained in hospital settings.1,3-5
Traditional hospital care by a generalist consists of rounding on hospitalized patients once or twice daily while maintaining an active outpatient practice. Drawbacks of this model include reduced outpatient efficiency due to constant hospital interruption and reduced hospital efficiency because acute changes cannot be acted upon in a timely fashion. 6 Hospitalist care involves a physician spending the vast majority of their time in the hospital caring for inpatients. Hospitalists have been shown to have shorter length of stay (LOS) and cost savings when compared with traditional hospital care while preserving patient satisfaction and quality of care.4,5,7,8
However, the Achilles heel of hospitalist medicine is discontinuity. 9 Despite current delivery and payment systems favoring the hospitalist style of inpatient care, long-term relationships between patients and their primary care teams continue to be as relevant inside today’s hospitals as they were in 1948 when W. Eugene Smith 10 published his landmark photo essay titled “Country Doctor.” Continuity of care has been associated with less hospitalization, fewer readmissions, and lower costs.11-13 A recent study of hospitalized Medicare patients showed that even though LOS was shorter for hospitalists, those cared for by their primary care physician had lower mortality and were more likely to be discharged home. 8
Despite making up just 6% of hospitals, it is important to study Academic Medical Centers (AMCs), because they account for more than 20% of hospital care. 14 AMCs commonly care for underserved local patients in addition to providing tertiary care not available elsewhere. 14 At many AMCs, hospitalists practice independently on nonteaching services and also act as preceptors on teaching services. The meta-analysis by Rachoin et al 5 found significant heterogeneity suggesting that different hospitalist environments may have very different outcomes. One study found that the academic-preceptor model had shorter LOS than hospitalists. 15 Another study found that a family medicine teaching service had shorter LOS and lower costs than hospitalists. 16 Family physicians have the benefit of continuity of care and knowledge about outpatient services available when caring for their patients in the hospital. Local community patients at AMCs have very different medical needs when compared with tertiary care patients. Because of these differences, it is important to determine the most efficient ways to care for local community inpatient needs at AMCs. We hypothesized that local family medicine patients cared for by a family medicine inpatient service had shorter LOS when compared with those cared for on other general medical services often staffed by hospitalists, familiar with tertiary patient care at an AMC, after adjusting for illness severity and other factors.
Methods
To test the hypothesis, a retrospective cohort study of Department of Family Medicine (DFM) patients was conducted comparing LOS between those admitted to the Family Medicine Inpatient (FMI) service and those admitted to other general medical inpatient services.
Setting
The DFM provides primary care for more than 80 000 community patients at 4 clinical sites and a single skilled care nursing facility. The FMI service admits any DFM patient who requires general inpatient medical care and is not excluded by specific criteria (age <16 years, requiring cardiac monitoring/telemetry). While most admissions to the FMI service come through the emergency department, the FMI service also accepts direct admissions from clinic and transfers from the intensive care unit or other hospital services. Additionally, DFM patients with specific diagnoses are occasionally admitted to gastroenterology or pulmonary medicine subspecialty services whenever they are below their maximum capacity. The FMI service is a teaching service at an academic medical center and is staffed by a family medicine board–certified attending physician who rotates on service for 1 week at a time, a senior family medicine resident (PGY3), a junior family medicine resident (PGY2 or PGY3) taking 24-hour call every third day, and 1 to 2 family medicine interns (PGY1) working a day or night shift. While the FMI service has no maximum census limit, backup processes exist if the morning census exceeds 12.
Patients outside the DFM are cared for by Hospital Internal Medicine (HIM) when they require general inpatient medical care. The 12 HIM services at the study institution vary in their primary admission criteria and structure. Four services are resident teaching services staffed by a hospitalist or general internist and residents, 1 is a fellowship service staffed by hospital medicine fellows, 2 are medical services for patients with active hematologic or solid organ malignancies, and the remainder are traditional hospitalist services staffed by a hospitalist and a nurse practitioner or physician assistant. One of the hospitalist services accepts patients requiring telemetry for noncardiac reasons. With the exception of the hematology and oncology services, the HIM services admit all patients requiring general inpatient medical care, including local internal medicine primary care patients, regional patients requiring a higher level of hospital care than available locally, and tertiary referral patients. All the HIM services have maximum census limits and backup procedures exist, including the temporary creation of additional hospitalist services should demand exceed capacity.
Occasionally, patients with a DFM primary care provider are inadvertently admitted to an HIM service. This likely happens because primary care clinics have blended teams and cross-departmental scheduling. For example, a DFM patient may be seen for an acute issue by an internal medicine physician and then mistakenly assigned to a HIM service. Additionally, an emergency department physician may erroneously admit DFM patients to a HIM service.
Cohort
A dataset of all hospitalizations of adult primary care patients at our institution during 2011-2013 was used for this study. Only patients giving consent for retrospective chart review research were included. All general medical patients empaneled to a DFM primary physician at any of 4 clinical sites located in and around Rochester, Minnesota who were discharged from either the FMI service or a HIM service were identified. Of note, surgical patients and patients admitted to subspecialty services such as cardiology, gastroenterology, and pulmonology were not included as they are not considered general medical patients. Postpartum patients admitted to the FMI service (n = 25) were the only exclusion.
Study Design
Thus, the final retrospective cohort contained all DFM patients admitted to either the FMI service or various HIM services during 2011-2013. Data regarding demographics, admission and discharge services, dates of hospitalizations and emergency department (ED) visits, LOS, dismissal diagnosis, and the Charlson Comorbidity Index 17 were obtained from the electronic health record. The Charlson Comorbidity Index provides a validated method of predicting mortality by weighting various comorbidities such as heart disease, lung disease, diabetes, chronic kidney disease, and malignancy. 17 It represents a measure of patient complexity useful in case-mix adjustment and has also been associated with hospital readmissions and cost of care.12,18,19 The study was reviewed and approved by the Mayo Clinic Institutional Review Board.
Analysis
Two groups of DFM patients were compared, those dismissed from the FMI service and those dismissed from an HIM service. The main dependent variable was total LOS at the study institution. A secondary outcome of any hospital readmission within thirty days of discharge was also examined, matching the Centers for Medicare and Medicaid Services (CMS) metric for hospital readmission. Although methods to adjust for potentially avoidable readmissions exist, 20 we chose to consider any readmission to eliminate subjectivity. Independent variables include age, gender, marital status, dismissal diagnosis, Charlson Comorbidity Index, number of prior hospitalizations, and number of prior ED visits. The International Disease Classification Version 9 (ICD9) code for the final primary dismissal diagnosis was mapped into 1 of 18 first level categories using the Clinical Classification Software (CCS) available from the Agency for Healthcare Research and Quality (AHRQ). 21 The 4 most common major categories, diseases of the circulatory system (CV), diseases of the digestive system (GI), infectious and parasitic diseases (ID), and diseases of the respiratory system (Pulm) were retained and the remaining categories were collapsed into 1 category (Other).
All data were abstracted electronically and analyzed using R version 3.02 (http://www.r-project.org/). Group statistics for the various factors and the dependent variable LOS were summarized using frequencies, mean, and standard deviation. Differences were compared using a Wilcoxon rank sum test for numeric data or a Fisher exact test for 2 × 2 categorical data or a chi-square test for n × 2 categorical data with P values less than .05 considered significant. As is typical for data that cannot be negative, we assumed LOS would be highly right skewed, thus necessitating a logarithm transform to yield an approximately normal distribution that preserves the positive value only characteristic for further analysis. Multivariate analysis using linear regression was carried out on the logarithm-transformed LOS variable to adjust for known risk factors with P values less than .05 considered significant.12,22-32 Percent change and 95% confidence intervals were calculated for each regression coefficient.
Results
There were 3100 admissions from 2117 unique patients during the study period. The majority of hospitalizations (2626) were dismissed from the FMI service. As expected, the LOS was highly right skewed (see Figure 1). A logarithm transform applied to the LOS data yielded an approximately normal distribution for further analysis.

Length of stay distribution and logarithm transform.
As shown in Table 1, age, gender, and marital status were not different between the groups. Patients dismissed from a HIM service had a higher Charlson Comorbidity Index (median 3 vs 5, Z = −7.55, P < .001), different distribution of final dismissal diagnoses (χ2 =29.2, df = 4, P < .001), slightly more hospitalizations in the previous 12 months (Z = −2.76, P = .006), and were more likely to have been admitted by a different service (19.2% vs 11.9%, P < .001). However, those dismissed from a HIM service had fewer emergency department visits in the previous 6 months (Z = 2.41, P = .016). Thirty-day readmission rates between FMI and HIM dismissed patients were similar. Median LOS was 0.9 days shorter for those dismissed from the FMI service (median 1.8 vs 2.7, Z = −10.04, P < .01).
Bivariate Statistics Comparing FMI to HIM Dismissals.

Abbreviations: SD, standard deviation; FMI, Family Medicine Inpatient service; HIM, Hospital Internal Medicine services; n/a, not applicable.
A multivariate linear regression model for the transformed dependent variable log(LOS) was computed, R2 = 0.24, F(14, 2931) = 64.4, P < .01. Because the dependent variable is log transformed, in Figure 2 we report percent change in LOS for a 1-unit change in the independent variable by exponentiating the coefficient, subtracting 1, and expressing the result as a percentage. Age decile (β = 0.03, t =3.85, P < .01), male gender (β = 0.08, t =3.09, P < .01), disposition to a location other than home (β = 0.39, t = 7.20, P < .01), Charlson Comorbidity Index (β = 0.03, t = 6.27, P < .01), a final dismissal diagnosis of ID (β = 0.37, t = 7.69, P < .01), previous hospitalizations (β = 0.05, t = 4.24, P < .01), and admission by a different service (β = 0.43, t = 10.5, P < .01) are all associated with longer LOS. Prior ED visits (β = −0.02, t = −4.86, P < .01) were associated with slightly shorter LOS. Dismissal from an HIM service was associated with a 33.1% (95% CI: 23.5%-43.5%) longer LOS after controlling for the covariates.
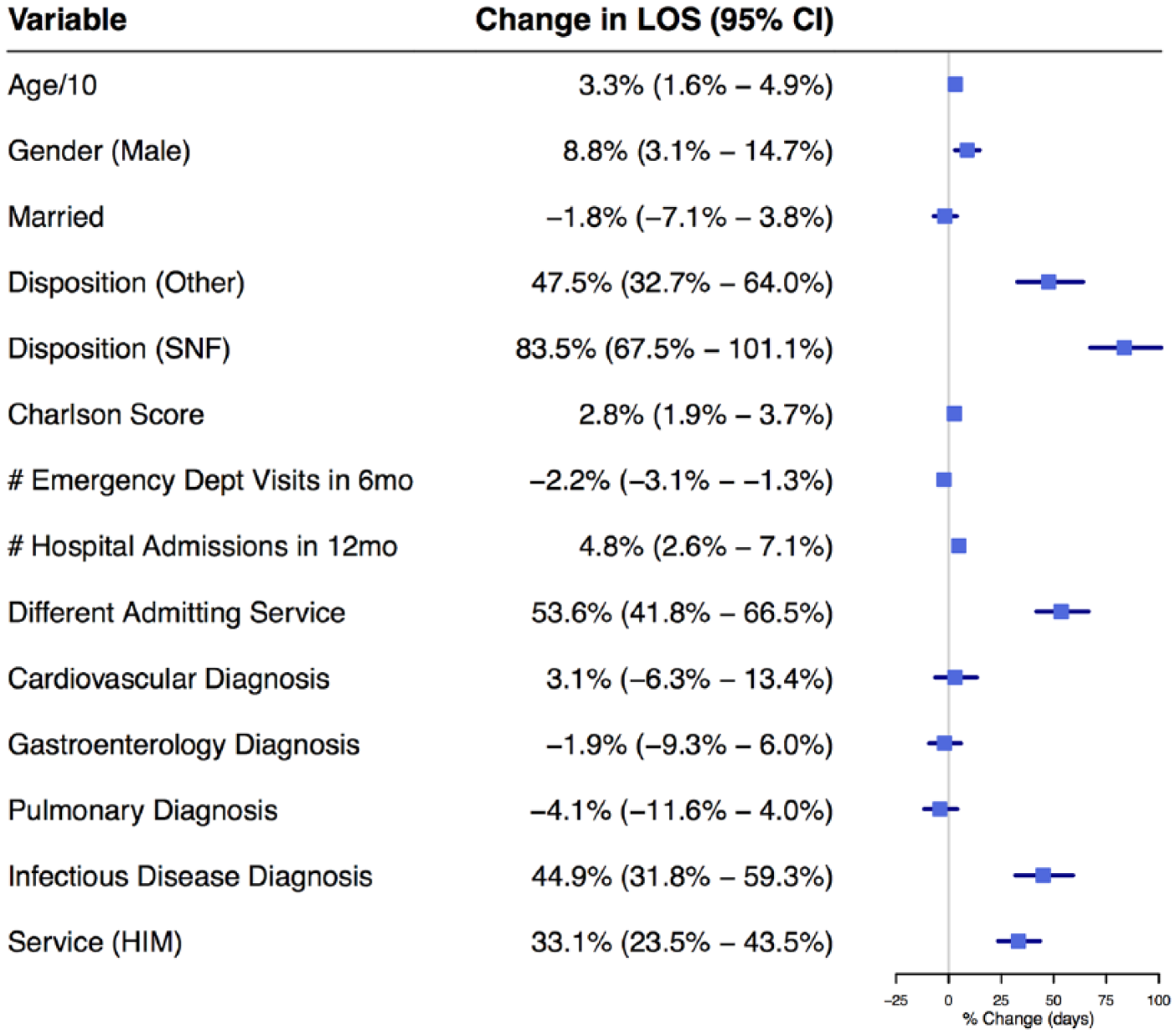
Linear regression model for log-transformed length of stay.
Discussion
Although family medicine patients dismissed by a HIM service have a higher Charlson Comorbidity Index, more dismissals to places other than home, and increased prior hospitalizations, LOS remains 33% longer even after controlling for these variables. This runs contrary to some studies comparing the hospitalist model to traditional practice that show hospitalists decrease costs and LOS.3,4,8 However, one study of a teaching family medicine service structured similar to the FMI service studied did show shorter LOS compared with the hospitalist model. 16 This may be because in the traditional model, the physician caring for the hospitalized patient often has other significant outpatient duties during the workday whereas in our model they have strictly inpatient duties.
Increased awareness of outpatient resources is one possible reason for shorter LOS on the FMI service. The FMI service is covered by staff physicians and residents who rotate on service for a defined period but spend the rest of their time engaged in outpatient practice. Therefore, they may be more aware of outpatient resources and better equipped facilitate an early transition to outpatient care than HIM clinicians. In their outpatient practice, they work closely with the same outpatient nurses and pharmacists who lead care management and anticoagulation management programs that help patients transition from inpatient to outpatient care. Additionally, the FMI service has a dedicated team of inpatient pharmacists, social workers, and nurses who also have extensive knowledge about community and outpatient resources. This facilitates discharge planning, which has been shown to shorten hospital stays and reduce readmissions. 33
A large study of Medicare patients showed primary care physicians were more likely to discharge patients home and had lower posthospitalization mortality. 8 These benefits were ascribed to increased continuity of care. 9 This aligns with our observation that the FMI service was more likely to discharge patients to home, perhaps because increased continuity results in more knowledge about the patient’s sociodemographic condition and support network.
Thirty-day readmission rates did not differ between FMI and HIM services suggesting that, similar to other studies, shorter LOS did not increase readmissions. 34 In fact, longer hospital stays have been associated with higher readmission rates, likely due to confounding with illness severity.29,35 While we did not measure outpatient continuity of care in this study, it has been connected to fewer readmissions. 14
Limitations
The Charlson Comorbidity Index was higher for patients admitted to HIM services. Hypertension, depression, and skin ulcers/cellulitis are not included in the index but have been found to contribute to the cost of care. 19 Additionally, patients cared for on HIM services had a different admitting service more frequently than FMI patients. This often occurs when unstable patients are initially admitted to the intensive care unit and then transferred to the floor prior to dismissal. Thus, it may represent the fact that patients cared for by HIM had a higher acuity level. Despite controlling for these factors, they may incompletely reflect the patient’s illness severity.
Two of the HIM services specialize in the care of patients with active malignancies. DFM patients are sometimes admitted to these services if they require inpatient chemotherapy. These 2 services have longer LOS than other HIM services. While the Charlson Comorbidity Index adjusts for complexity of these patients, we also performed a sub-analysis that excluded the 69 DFM patients admitted to these services. There was no significant change in the multivariate LOS difference, perhaps because the FMI service also cares for many DFM patients with complications of active malignancy.
Patients admitted to subspecialty gastroenterology and pulmonology services were excluded from the study. While DFM patients presenting with gastroenterology or pulmonary complaints are not excluded from admission to these services, they are more commonly admitted to the FMI service. Table 1 demonstrates this with the higher proportion of GI and Pulm final primary diagnoses for the FMI service. These diagnoses were not associated with LOS in the multivariate analysis.
Patients requiring telemetry for cardiac diagnoses are admitted or transferred to cardiology and were not included in this study. However, it is notable there was a slightly increased proportion of CV diagnoses among the HIM group. The reasons for this are unclear but HIM may hold on to some cardiac patients that FMI transfers to cardiology. Additionally, one HIM service cares for patient requiring telemetry for noncardiac reasons. Because these patients have a higher level of acuity, they may have longer LOS. The number of patients affected is likely very small (<50) but due to the data recorded, we were not able to identify them. We are unsure if the Charleston Comorbidity Index adequately adjusts for these factors.
Our study was conducted at a single academic medical center and the FMI service has a teaching structure. Thus, our results may not generalize to other environments. Additionally, a small number of HIM physicians rotate on their teaching services and have outpatient practices very similar to the FMI service. Given the information recorded, we were unable to discern when one of these physicians was primarily responsible for a patient. However, we would expect that this dilution of the HIM hospitalist service model would actually understate the measured differences. We did not evaluate factors such as nursing ratios or hospitalist workload that have been associated with LOS changes.36,37 However, the hospital infrastructure, daily service census, and nursing unit staffing is very similar between HIM units and the FMI unit. Further study regarding the actual knowledge difference between family physicians and hospitalists regarding outpatient resources available to assist patients with the transition from hospital to home is warranted. However, because such knowledge is highly localized, findings at our institution may not generalize.
Conclusion
Local primary care patients at the AMC were safely discharged sooner from the FMI service than HIM services after controlling for covariates. Readmission rates were not different. Continuity of care, more intimate knowledge of outpatient resources available to assist with transitions of care, and potential additional unadjusted complexity of patients on HIM services likely contribute to shorter LOS for FMI patients.
Footnotes
Acknowledgements
We thank Tiffany Matti and Julie Maxson for helping to obtain the data necessary for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Department of Family Medicine, Mayo Clinic, Rochester, MN, Small Grant Funding, Mayo CCaTS grant UL1TR000135.