
Abstract
Keywords
Introduction
Hearing loss is one of the most prevalent chronic disabilities affecting more than 1.33 billion people globally. 1 Unaddressed hearing loss has a devastating impact on the individual and family, but also on the global economy. A recent report from the World Health Organization (WHO) estimated the annual cost of unaddressed hearing loss to be approximately USD750 billion. 2 The high costs of hearing loss and widespread prevalence draws attention to the importance of access to care. 3 Early access to timely diagnosis and management can reduce the adverse effects of hearing loss and, ultimately, can minimize the burden of disease. 4 Unfortunately, accessible hearing care is not a reality in many developing world regions like sub-Saharan Africa where, ironically, the majority of people with hearing loss reside. 5
In many low- and middle-income countries, primary health care (PHC) remains the only effective gateway to some form of health care. 6 Thus, expanding and decentralizing ear and hearing care to a PHC clinic may increase equitable access for early diagnosis and management.4,7 Providing hearing care at PHC may, however, be challenging due to equipment costs and insufficient numbers of hearing care providers with one audiologist to every million people or more in developing world regions.8,9 To address these challenges at a PHC level, the traditional model of audiological service delivery needs to be approached in a different way. 10
Self-reported hearing loss is a simple screening method that can facilitate early hearing detection and timely referral to audiological services in a PHC setting if linked to a clear and efficient referral pathway. 11 This method has been proposed to be affordable, time-efficient, and can be administered by any health care worker.3,11 The use of a single question may also overcome language and cultural barriers,11-14 which is considered an important factor in multicultural and multilingual settings like South Africa.
Using self-reported hearing loss as a single hearing screen question or a questionnaire on hearing functioning have both been proposed as valid screening methods.3,11,12,14-18 The Hearing Handicap Inventory for the Elderly–Shortened (HHIE-S), for example, is a screening questionnaire consisting of ten questions evaluating the perceived social situational and emotional effects of hearing loss in the elderly. 16 Although the HHIE-S was standardized for individuals older than 65 years, Nondahl et al 16 found that it demonstrated lower sensitivity and accuracy in older individuals (65-92 years) compared with younger individuals (48-64 years). Contrary, using a single question such as “Do you feel you have a hearing loss?” showed sufficient accuracy in young and older individuals in various reports.11,16,17 Using a single question to screen for self-perceived hearing loss has also the advantage that it is easy to administer and may also be used in cases where individuals present with poor sight or minor cognitive impairment.11,17
Using a single question to screen for hearing loss may be particularly accurate in cases where there is a moderate or severe hearing loss, in cases where individuals are 60 years and older, in cases where individuals have a high-frequency hearing loss (4 and 8 kHz), and also in individuals who experience speech-recognition-in-noise difficulties.15-20 Hence, it shows the potential value of using a self-report of hearing loss in a PHC clinic. 11 However, self-report of hearing loss is not regarded as a standard or recommended protocol to identify hearing loss. 15 Although its use in combination with an audiometric screening has been proposed,20,21 it requires further investigation, particularly in PHC settings to investigate the performance of this technique in isolation or with a second-stage audiometry screen. Using second-stage audiometry screen may be beneficial as it may provide more accurate results. 20 The current study therefore evaluated the performance of self-reported hearing loss in isolation and in combination with pure tone audiometry screening in PHC clinics in South Africa.
Methods
This research project was approved by the Institutional Research Board of the University of Pretoria, South Africa and was part of a larger community-oriented primary care (COPC) project in Gauteng (Tshwane) province 22 (protocol number: 102/2011).
Selection and Description of Participants
A cross-sectional design was used at 2 PHC clinics (PHC clinic 1 and PHC clinic 2) situated in underserved communities in Tshwane, both having limitations in human resources for hearing care and a lack of appropriate equipment. Nonprobability purposive sampling was used to recruit participants at both clinics. At PHC clinic 1, all individuals who visited the clinic were offered a hearing screening. At PHC clinic 2, all individuals who were available during the time that the services were delivered and who wanted their hearing tested were recruited for the study. Only those 16 years and older, who provided signed consent and who completed the screening protocol (i.e., self-reported hearing loss and audiometric hearing screening) were invited to participate in the study.
Participants who presented with a mixed or conductive hearing loss were referred to the clinics’ general practitioner for further medical examination and intervention. Participants who presented with a sensorineural hearing loss were referred to the nearest district hospital for a hearing aid fitting evaluation.
Procedures
Hearing screening included a self-report of hearing loss as well as audiometry screening for all participants. Participants who failed the audiometry hearing screening were invited to undertake diagnostic audiometry to confirm that there was a hearing loss. Diagnostic testing was also performed on a group of 81 participants who passed the screening test to allow determination of screening specificity (Figure 1). A convenience sampling strategy was used to select these participants. One to 2 participants per day who passed the hearing screening, were selected based on their availability and clinic time constraints. Instructions were provided in English or Afrikaans. Written instructions in Sepedi were used if participants did not understand English or Afrikaans. If participants were unable to understand one of these three languages, a health care nurse who was available at the specific time, was asked to translate the information.

Flow diagram of how results are presented in the current study.
Self-Reported Hearing Loss
The key question used in the current study was “Do you have a hearing problem? “Yes/No.” 11 Using a single question demonstrated sufficient accuracy in various reports.11,16-18 The participant’s response was recorded on the data collection form.
Pure Tone Audiometry Screening
Pure tone audiometry screening was conducted on all participants regardless of their self-reported hearing loss response. Pure tone audiometry screening was conducted by audiology students from the University of Pretoria under supervision of an experienced audiologist (first author). Testing was conducted in an examination room without sound isolation. Because of time and facility constraints at clinics more than one participant was examined at the same time in a room in some instances. Each ear was assessed. Audiometry screening was performed with the validated hearScreen Android OS application (hearX group, Pretoria, South Africa) on a Samsung Galaxy Pocket Plus S5301 phone with calibrated supra-aural Sennheiser HD202 II headphones (Sennheiser, Wedemark, Germany).23,24 Screening audiometry was conducted according to recommended guidelines 25 with a failure to respond to 35 dB HL at any of the test frequencies in either ear indicating immediate rescreening of both ears using the same protocol. 23 The hearing screening application monitored and recorded noise levels during data collection for each participant. Noise monitoring using the hearScreen application on these smartphones has been reported to be accurate within 1 to 1.5 dB, depending on frequency. 23 Recorded noise levels consisted of mean ambient noise recorded by the smartphone during pure tone presentation (1.2-second duration) in the octave band corresponding to the test frequency. 23
Pure Tone Diagnostic Testing
Diagnostic testing was used for confirmation of a hearing loss on participants failing the screening for a second time on either ear. The procedure was performed on the same day, and in the same examination room as the screening tests. Automated pure tone audiometry (air- and bone-conduction) was performed for both ears at 0.5, 1, 2, 4, 8 kHz using a Type 2 Clinical Audiometer (KUDUwave, eMoyo, South Africa). Insert earphones were placed deep in the ear canals with circumaural headphones placed over the ears to improve attenuation of ambient noise, and to minimize the occlusion effect. An automated threshold-seeking paradigm was used with a similar threshold-seeking method used in a manual test configuration, that is, the modified Hughson-Westlake method. Air and bone conduction thresholds were determined with masking of the nontest ear when indicated. A hearing loss in an ear was confirmed by diagnostic audiometry if the 4-frequency average (4FA) was ⩾25 dB HL (clinically significant hearing loss). The software actively monitored ambient noise levels across octave bands throughout the test procedures in both clinics. Whenever the noise exceeded the maximum ambient noise level allowed for establishing a threshold, the test operator could pause the automated testing and wait for the transient noise to subside before continuing the test.
Data Analysis
Self-reported hearing loss data were obtained from the data collection form while audiometric screening data was extracted from the cloud-based data management system (mHealth Studio, hearX group, South Africa). Participant confidentiality was ensured as behavioral pure tone threshold information for each individual was reported using an alphanumeric code. The identity of the participant represented by this code was known only to the first author.
Data were analyzed using SPSS v24 (IBM Corp, Armonk, NY, USA). Data were reported according to 3 groups: screening group, assessment group, and diagnosed group (Figure 1). The screening group included all participants and descriptive statistical measures were used to determine how many participants self-reported hearing loss, failed audiometry screening, and both self-reported hearing loss and failed audiometry screening. A binary logistic regression model was used to determine the effect of age (as a continuous variable), gender and race on self-reported hearing loss (P < .05 indicated significance). Participants were divided into 3 age-groups (16-39, 40-59, and ⩾60 years) to determine the effect of increasing age on self-reported hearing loss. In the assessment group, all participants who failed audiometry screening, and who attended for diagnostic assessments (including 81 participants who passed the audiometric screening) were included in the analysis to evaluate the performance of self-reported hearing loss in isolation, and a combination of self-reported hearing loss and pure tone audiometric screening. Descriptive statistical measures were used to determine how many participants self-reported hearing loss, and how many self-reported hearing loss and failed audiometry screening. Descriptive statistical measures were used to report how many participants were diagnosed with mid-frequency hearing loss ([4FA] 0.5-4 kHz and high-frequency average [HFA] 4 and 8 kHz) resulting in the diagnosed group. The performance (sensitivity, specificity, positive predictive value, and negative predictive value as well as overall test accuracy) of the different protocols (self-reported hearing loss and self-reported hearing loss with second stage pure tone audiometry screening) was calculated in reference to diagnostic audiometry results (4FA and HFA). A high-frequency loss was confirmed if the HFA was ⩾25 dB HL.
Results
A total of 1084 participants, 16 years and older, were included in the study; 55.6% were from PHC 1, 74.0% were female, and 69.0% and 31.0% of the sample was African and Caucasian respectively. The mean age was 41.2 years (SD 15.5 years; range 16-97 years). Four hundred and thirty-six participants (40.2%) self-reported a hearing loss while 189 participants (17.4%) failed the pure tone audiometry screening. One hundred and thirty-six participants (12.5%) both self-reported hearing loss and failed pure tone audiometry screening (Figure 1).
The mean age of those who self-reported hearing loss was 44.2 years (SD 15.8 years; range 16-97 years), and the majority were female (72.4%; n = 316). Gender and race did not have a significant association with self-reported hearing loss (P = .498; P > .05; Binary logistic regression). Self-reported hearing loss increased significantly with increasing age (P < .05; binary logistic regression) (Table 1).
Distribution of Self-Reported Hearing Loss Across Age and Gender Categories (n = 1084).

The highest sensitivity for self-reported hearing loss compared with failed audiometry screening was found in the ⩾60 years age-group (Table 2). Specificity was highest for the younger age-group (16-39 years).
Sensitivity and Specificity for Detecting Significant Hearing Loss (4FA ⩾25 dB HL by Diagnostic Audiometry) for Those Who Self-Reported Hearing Loss According to Different Age-Groups (n = 436). a
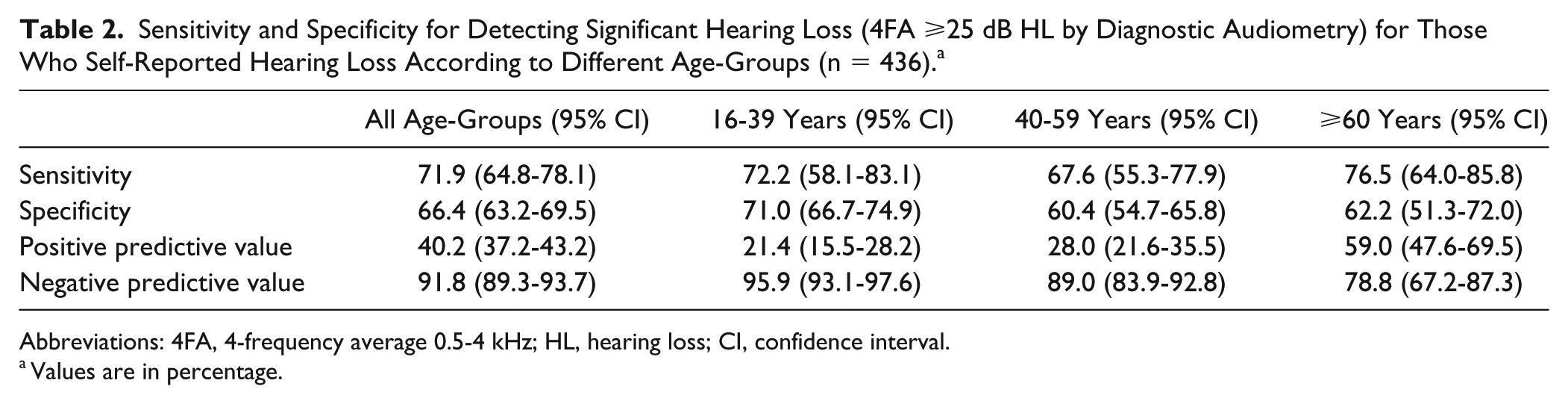
Abbreviations: 4FA, 4-frequency average 0.5-4 kHz; HL, hearing loss; CI, confidence interval.
Values are in percentage.
To compare the test accuracy of self-reported hearing loss alone and in combination with second-stage pure tone audiometry screening, the assessment group included 195 participants who attended diagnostic assessments (Figure 1). The mean age of the assessment group was 45.6 years (SD 17.9 years; range 16-97 years; 65.1% female, 66.2% and 33.8% African and Caucasian, respectively). Of these 195 participants, 69.7% self-reported a hearing loss, and 49.7% both self-reported hearing loss and failed the hearing screening test (Figure 1).
Of the 195 participants that were tested diagnostically, 131 (67.2%) were identified with a mid-frequency hearing loss (4FA ⩾25 dB HL) (Table 3). Using HFA ⩾25 dB HL as cutoff, all participants who were identified with hearing loss using 4FA were identified with an additional three participants who did not have a 4FA ⩾25 dB HL.
Descriptive Comparison of Participants Diagnosed With Hearing Loss Using an Audiometric Cutoff 4 FA ⩾25 dB HL and 4FA and HFA ⩾25 dB HL.

Abbreviations: 4FA, 4-frequency average 0.5-4 kHz; HFA, high-frequency average 4-8 kHz; SR HL, self-reported hearing loss; PTA screen, pure tone audiometry screening.
Combining self-report with second-stage audiometry screening revealed a higher test accuracy (81.0% and 86.1%, depending on the audiometry cutoff) compared with self-report hearing loss alone (Table 4). Using the combined test protocol also revealed higher specificity (100%) in comparison to self-report measures alone (62.3%). The combination of self-report and an audiometry screening was more sensitive in detecting those with a high-frequency hearing loss (81.1%) than those with mid-frequency hearing loss (72.8%). However, self-report alone was more sensitive to detecting a mid-frequency than a high-frequency hearing loss.
Sensitivity and Specificity (With 95% Confidence Intervals) of Different Screening Protocols Used in Primary Health Care Clinics Using a 4FA ⩾25 dB HL and HFA ⩾25 dB HL Cutoff in Assessment Group (n = 195). a
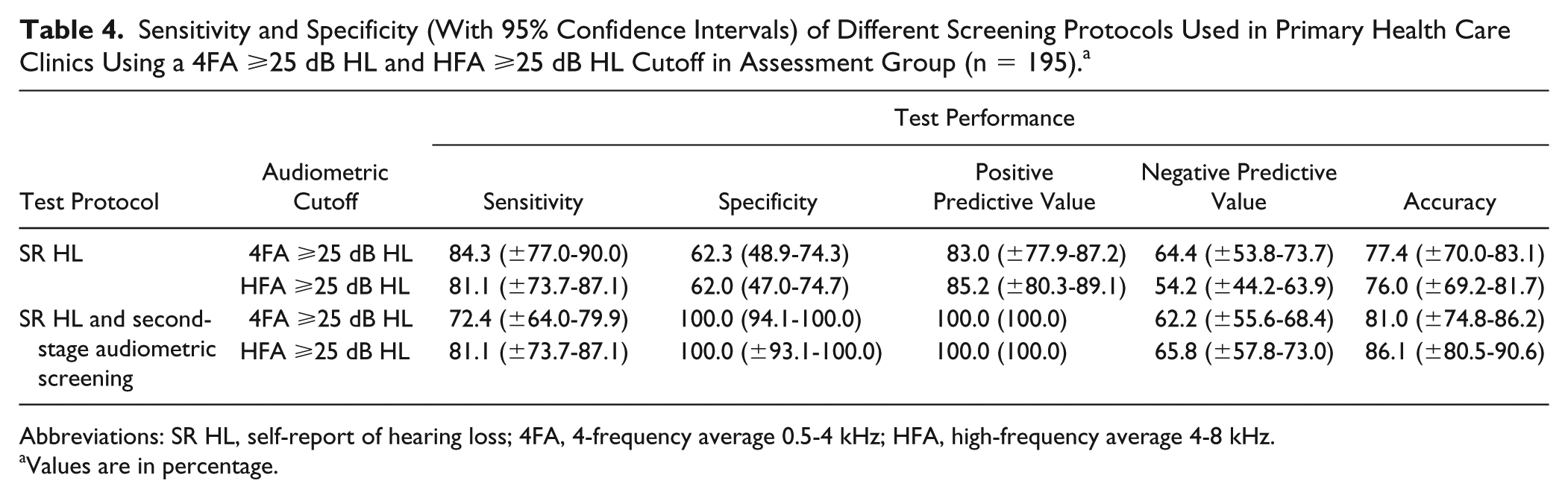
Abbreviations: SR HL, self-report of hearing loss; 4FA, 4-frequency average 0.5-4 kHz; HFA, high-frequency average 4-8 kHz.
Values are in percentage.
Discussion
The burden of chronic diseases such as hearing loss is increasing in low- and middle-income countries. 5 In the midst of the growing burden of hearing loss, hearing care services are still scare in these regions. 5 As PHC continues to be the only effective gateway to some form of health care in many low and middle income countries, decentralizing hearing care at PHC levels for early detection and treatment has been promoted by the WHO.6,26 The current study therefore evaluated the performance of self-reported hearing loss in isolation, and in combination with second-stage pure tone audiometry screening in PHC clinics in South Africa.
Results of the current study demonstrate that the number of people who self-reported hearing loss increased significantly with increasing age. The highest sensitivity, compared with the number of people who failed audiometry screening, found to be most common in the ⩾60 years age category. This is in agreement with previous studies indicating a significantly higher prevalence of self-reported hearing loss for older age samples, probably due to the increasing prevalence of presbycusis with age.11,14,16-18 Nondahl et al 16 also found that older individuals are more likely to self-report hearing loss as they are more accepting of hearing impairment as they consider it a typical aspect of aging. Contrary to this, Kamil et al 27 reported an increasing rate of subjective underestimation of hearing loss in adults 70 years and older. The authors further noted that different perceptions of hearing loss in younger versus older adults (eg, older adults may consider hearing loss to be normal and do not report it), which may contribute to an underestimation of hearing loss in older adults. 27 Apart from different perceptions of hearing loss related to age, stress, anxiety, the presence of middle ear infection and tinnitus can also influence accurate self-report measures resulting in over- or underestimation of hearing loss.28-30 As such, using self-report measures may not be sufficiently sensitive to identify hearing loss and may require a combined approach that includes a test in combination with self-report or as a second-stage screen. 21
The study findings showed a high specificity (100%) for a combined screening method. This is an important finding for the efficiency of a screening program particularly in a PHC setting as unnecessary referrals will most likely be excluded. 31 In addition, a combined screening method had a higher test accuracy (86.1% and 81.0%) than self-report measures in isolation (77.4% and 76.0%) when compared with a 4FA and HFA ⩾25 dB HL audiometric protocol when used as the gold standard. This indicates that using self-perceived hearing loss and a second stage audiometry screen has greater benefit for timely diagnostic audiology referrals compared with self-reported measures in isolation. Previous studies also indicated the need to combine both self-report measures with a hearing assessment for a more accurate identification of hearing loss.20,21
This study has shown that a screening strategy of a self-report plus an audiometry screen will better identify those with a high-frequency than those with a mid-frequency hearing loss. This is despite the fact that the screening frequencies do not include 8 kHz. A large percentage of speech cues are found between 4 and 8 kHz, and therefore it is possible that participants are reflecting deficits in high frequency speech perception when self-reporting hearing loss. 11 Using this screening strategy may also be appropriate to detect high-frequency hearing loss in conditions such as presbycusis and ototoxicity from HIV and tuberculosis treatment 32 in PHC clinics where conditions such as HIV and tuberculosis are being treated at primary level, at least in the South African context. 33
One of the basic challenges for PHC hearing care is finding a screening tool that is affordable, simple, and efficient. Self-reported hearing loss is a simple procedure that can be a strong predictor of quality of life and well-being, it can play a role in determining the social burden of hearing loss and it can also be used to evaluate the need for audiological rehabilitation.17,21 Using a single question has demonstrated performance results similar to the HHIE-S16-18; thus it may be a useful initial screen to facilitate timely referrals11,17 particularly in a PHC context.
The findings of the current study, however, demonstrated that, when used in isolation, however, self-report measures may not be sufficiently sensitive to detect hearing loss in a PHC context. A single question on self-perceived hearing loss may also not always be an accurate screening method in a PHC setting with the risk of being interpreted differently by some participants. 11 Thus, future research should investigate if the use of a questionnaire such as the HHIE-S may be more appropriate in a PHC context.
Findings from the current study showed that combing self-report measures with a user-friendly, affordable second stage audiometry screening tool, has the potential to accurately detect in particular high-frequency hearing loss. The results of the study furthermore indicated that a simple high frequency audiometry screening as a second-stage screen may significantly improve overall performance and efficiency of the screening protocol. This implies that the screening protocol becomes optimized in terms of time and resource requirements as only those who self-report hearing loss are screened. Using this affordable, simple, and efficient hearing screening strategy may improve access to hearing care at PHC clinics in resource-starved countries. Future studies may investigate whether the inclusion of 8 kHz in the audiometry screening is appropriate for PHC contexts to improve management of hearing loss resulting from ototoxic treatments.
Footnotes
Acknowledgements
The authors would like to acknowledge the audiology students at the University of Pretoria, who assisted in hearing testing, and the participants at the different clinics who participated in this study.
Authors’ Note
Opinions expressed, and conclusions arrived at, are those of the authors and are not necessarily to be attributed to the National Research Foundation.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The hearScreen application is intellectual property owned, patented and trademarked by the University of Pretoria. The product is being developed for commercialization and more information is available at ![]()
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The financial assistance of the National Research Foundation (NRF) toward this research is hereby acknowledged (Grant No. 87757).