
Abstract
Background
Febrile seizures (FS) are often associated with viral infections. COVID-19 infection may be related to FS. The objective is to evaluate the prevalence and characteristics of FS during COVID-19 period.
Methods
This retrospective study of children aged 6-60 months with FS or COVID-19 infection was conducted at a tertiary hospital from January 2020 to November 2023, categorized by pre-Omicron, transition, and Omicron periods. Data from all FS and COVID-19 cases were descriptively analyzed using mean or median, and compared across three periods using ANOVA. The characteristics of FS with and without COVID-19 patients, as well as COVID-19 with and without FS patients, were compared by using t-test or Wilcoxon rank-sum test.
Results
The FS prevalence in COVID-19 patients was 0.36%, with age-specific prevalence of 1.31% in COVID-19 cases aged 6-60 months. Males were more prevalent in all FS groups. Generalized seizures and simple FS were the most common presentations. Thirty-three percent of FS with COVID-19 were complex febrile seizures, compared to 20% in non-COVID-19 cases. Cough was a significant symptom in COVID-19 without FS (p=0.03), while male, higher body temperature, pulse and respiratory rate were more prevalent in COVID-19 cases with FS (p <0.05).
Conclusions
COVID-19 does not increase the risk of FS compared to other causes. Male gender, higher body temperature, pulse and respiratory rate in COVID-19 children are associated with FS. Cough was a less relevant symptom for FS in COVID-19 children. Well-designed, large-scale research is needed to better understand FS in pediatric COVID-19 patients.
Introduction
Febrile seizures (FS) are common in children, with an estimated 2-5% in the US and Western countries, but higher rates are reported elsewhere, such as 9-10% in Japan, 5-10% in India.1,2 FS occurs in children aged 6-60 months, associated with a febrile illness, without CNS infection, neurological disease, or metabolic disturbance. 3 FS are classified as simple (generalized, no recurrence in 24 hours, less than 15 minutes) and complex (focal onset, recurrence in 24 hours, or lasting over 15 minutes).1,3 There is a genetic predisposition involving FEB 1-9, SCN1A/1B, SCN2A, and GABA-A receptor genes. 4 The exact cause is unclear, but it is often related to viral infections like herpesviruses, influenza, adenovirus, parainfluenza, RSV, rotavirus, bacterial infections, or post-vaccination. 5 Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes COVID-19, first identified in Wuhan in December 2019, with symptoms including fever, cough, rhinorrhea, sore throat, fatigue, diarrhea, and vomiting.6-8 Neurological symptoms range from mild to severe, such as headache, encephalitis, seizures, and stroke.9,10 Data on FS prevalence with COVID-19 and related risk factors in children are limited, especially in Thailand. The overall FS prevalence in COVID-19 varies from 0.19% to 4.5%,11-14 with higher rates up to 13% during the omicron period. 11 Younger age, family history, and fewer symptoms increase FS risk. 11 ; older age and higher temperature may also be factors associated with an increased prevalence of FS during the Omicron period. 15 This study aims to evaluate the prevalence of FS during the COVID-19 pandemic and identify characteristics in children with and without COVID-19.
Materials and Methods
Study Design and Setting
This was a retrospective review of medical charts for children aged 6 to 60 months diagnosed with FS or COVID-19 at HRH Princess Maha Chakri Sirindhorn Medical Center, Nakorn-Nayok, Thailand, a 500-bed tertiary university medical center and referral regional hub from nearby hospitals, including the primary, secondary, and general hospitals, from January 2020 to November 2023. Patients were identified using ICD-10 diagnostic codes for FS (R56.0) and COVID-19 (U07.1, U07.2, and B972). This study was conducted from March 2024 to March 2025. Data collection was performed over eight months from March 2024 to October 2024, following Ethics Committee approval, and subsequent analysis was conducted from November 2024 to March 2025.
Diagnosis of FS
Seizures in young children, typically aged 6-60 months, that occur with fever and are not associated with central nervous system infection, or acute symptomatic seizures, such as metabolic disturbances or a history of unprovoked seizures. We classified FS into two types: simple FS, defined as generalized seizures lasting less than 15 minutes without recurring within 24 hours, and complex FS, characterized by focal seizures, seizures lasting longer than 15 minutes, or recurrent seizures within 24 hours.
Diagnosis of COVID-19 Infection
COVID-19 infection was confirmed using polymerase chain reaction (PCR), antigen test kits (ATK), or both to detect SARS-CoV-2.
The Inclusion and Exclusion Criteria
All patients aged 6-60 months diagnosed with FS or COVID-19 at our hospital were included. Children younger than 6 months or older than 60 months were excluded from the FS and the COVID-19 groups. Patients with underlying epilepsy, structural brain anomalies, seizures without fever, or other causes of seizures, such as hypoglycemia or hyponatremia, were excluded from the FS group.
Study Periods
The study periods (January 2020–November 2023) were divided into three periods: pre-Omicron (January 2020- October 2021), transition phase (November 2021–January 2022), and Omicron phase (February 2022–November 2023). The pre-Omicron period began with the first reported COVID-19 case in Thailand in January 2020. The Omicron variant was first reported by the WHO in November 2021, and the first case in Thailand was identified in December 2021. As cases diagnosed with COVID-19 between November 2021 and January 2022 may have involved mixed circulating variants, this interval was defined as a transition period. The subsequent period, from February 2022 to November 2023, was therefore classified as the Omicron period.
Data Collection
Data for FS covered sex, age, clinical signs, fever duration before seizures, seizure type, FS type, history of FS, family history of FS and epilepsy, body temperature (BT), pulse (PR) and respiratory rate (RR), laboratory results (CBC, serum sodium), seizure treatment, FS cause—compared across periods and between patients with and without COVID-19. COVID-19 data included sex, age, symptoms, vital signs, SpO2, ICD-10 diagnosis, and antiviral treatment, also compared among periods and between those with and without FS.
Statistical Analysis
Categorical variables were summarized as counts and percentages and compared using the Chi-square or Fisher’s exact test. Continuous variables were reported as mean with standard deviation (SD) for data that were normally distributed, and as median with interquartile range (IQR) for non-normally distributed data. For comparison between two groups, the t-test was used for normally distributed data, and the Wilcoxon rank-sum test for non-normal data. When comparing more than two groups, one-way ANOVA was used for normally distributed data, whereas the Kruskal-Wallis test was used for non-normal data. A p-value less than 0.05 was considered statistically significant. All statistical analyses were conducted using Stata software, version 14 (StataCorp LP, College Station, TX, USA).
Results
From January 1, 2020, to November 30, 2023, our hospital treated a total of 144,695 pediatric patients. Of these, 36.33% (52,564 patients) were between 6 and 60 months old. The pediatric cases of 2,532 have been reported positive for COVID-19, including 686 in the 6-60 months age group. A total of 124 FS cases in the age group of 6-60 months were recorded, with 9 of these diagnosed with both FS and COVID-19 infection (Figure 1). Flow chart for selection of febrile seizure and COVID-19 study population. ICD-10: The 10th revision of the international classification of diseases; TSC: tuberous sclerosis complex; IEM: inborn error metabolisms; AFI: acute febrile illness; FS: febrile seizures
Prevalence of Febrile Seizure Patients in the COVID-19 Era
The overall FS prevalence among COVID-19-positive patients was 0.36% (9 of 2,532), with an age-specific prevalence of 1.31% (9 of 686) in the COVID-19-positive cases aged 6 to 60 months. Furthermore, the prevalence of FS with COVID-19 cases in all FS was 7.25% (9 of 124).
The Characteristics of All Febrile Seizure Patients
In FS cases, 72 (58.06%) were males and 52 (41.94%) females, with a median age of 20 months (IQR 13-29 months). Among these patients, 98 experienced simple FS, while 26 had complex FS; 22 had recurrent seizures within 24 hours, 2 had focal seizures, and 2 had seizures lasting over 15 minutes. A total of 25 individuals (20.16%) had a history of prior FS, which in 15, 7, 1, and 2 cases had 1, 2, 3, and 4 episodes of previous FS, respectively. Additionally, 41 participants (33.06%) reported a family history of FS. Only 2 (1.61%) reported a family history of epilepsy. Nine participants (7.25%) had prior COVID-19 infections. Of these, one experienced FS during the initial infection and subsequently developed a recurrent FS without COVID-19. Another did not experience FS during the initial infection but later developed FS during a subsequent COVID-19 infection. The remaining participants had no FS during their initial COVID-19 infection; however, they later experienced FS without COVID-19. All were classified into the FS group or the COVID-19 group, according to the prevalence of FS and/or COVID-19 infection during the study period.
Clinical Manifestations and Diagnosis/Causes of All FS Patients Classified by the Study Periods

*A patient may have more than one clinical symptom.
Febrile Seizure Patients in the Pre-Omicron, Transition, and Omicron Periods
The Characteristics of FS Patients in the Pre-Omicron, Transition, and Omicron Periods

GTC: generalized tonic clonic seizures, GT: generalized tonic seizures, GC: generalized clonic seizures, FS: febrile seizures, BPM: beats per minute, WBC: white blood cells, p-value < 0.05= significance.
aThe number of FS cases in the pre-omicron era was 52.
bThe number of FS cases in the pre-omicron era was 51.
Febrile Seizure Patients With and Without COVID-19 Infections
The Characteristics, Clinical Features, Laboratory Values, and Treatment of FS With and Without COVID-19

GTC: generalized tonic clonic seizures, GT: generalized tonic seizures, GC: generalized clonic seizures, FS: febrile seizures, BPM: beats per minute, WBC: white blood cells, p-value < 0.05= significance.
aTotal number of FS with COVID-19 negative was 114.
bTotal number of FS with COVID-19 negative was 113.
COVID-19-Positive Pediatric Patients
The Characteristics, Clinical Signs and Symptoms, Diagnosis, and Treatment in COVID-19 Patients in Each Period
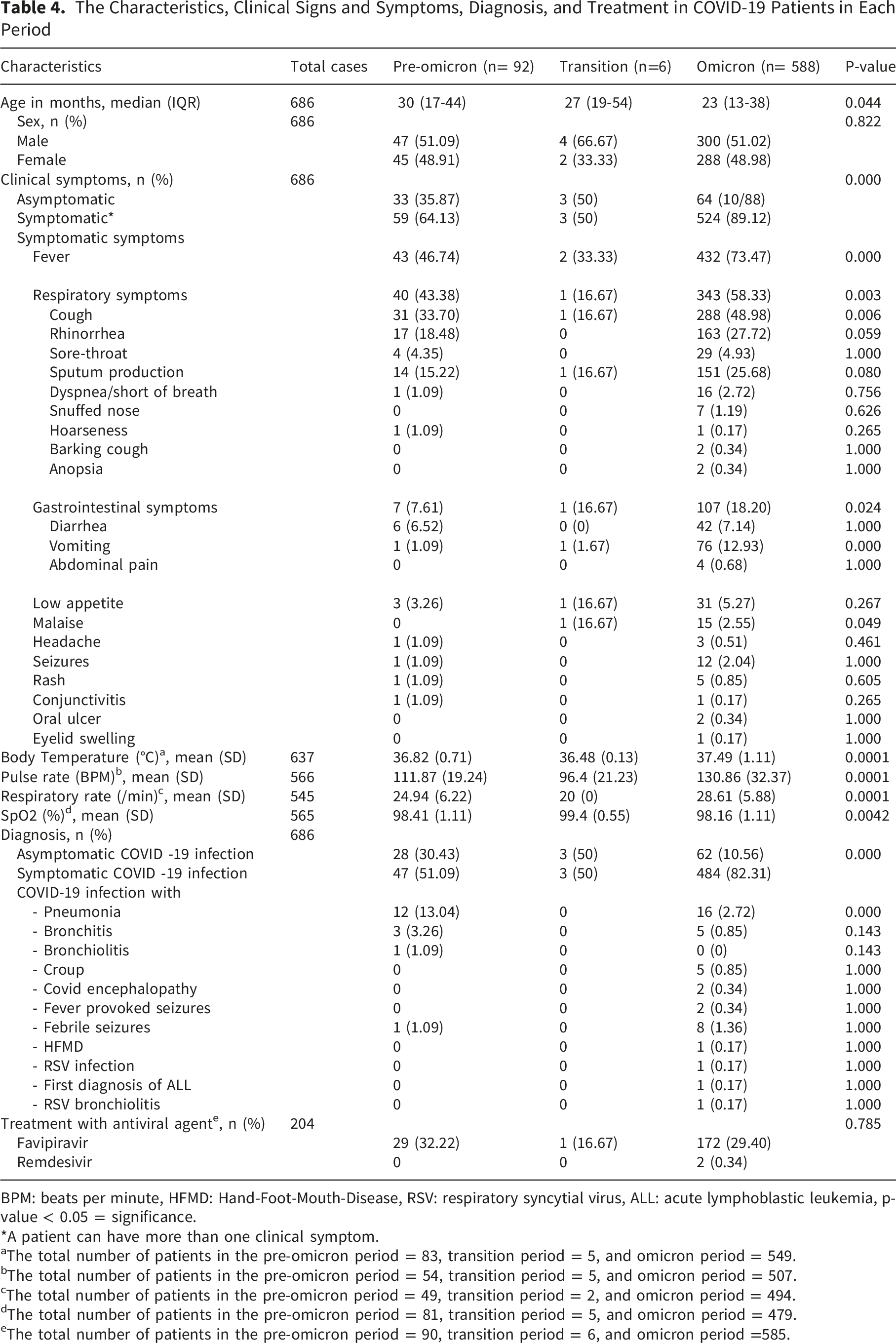
BPM: beats per minute, HFMD: Hand-Foot-Mouth-Disease, RSV: respiratory syncytial virus, ALL: acute lymphoblastic leukemia, p-value < 0.05 = significance.
*A patient can have more than one clinical symptom.
aThe total number of patients in the pre-omicron period = 83, transition period = 5, and omicron period = 549.
bThe total number of patients in the pre-omicron period = 54, transition period = 5, and omicron period = 507.
cThe total number of patients in the pre-omicron period = 49, transition period = 2, and omicron period = 494.
dThe total number of patients in the pre-omicron period = 81, transition period = 5, and omicron period = 479.
eThe total number of patients in the pre-omicron period = 90, transition period = 6, and omicron period =585.
COVID-19 Patients With and Without Febrile Seizures
The Characteristics, Clinical Symptoms, and Treatment of COVID-19 With and Without FS

BPM: beats per minute, p-value < 0.05 = significance.
*A patient may have more than one clinical symptom.
aThe total number of COVID-19 patients without FS was 628.
bThe total number of COVID-19 patients without FS was 557.
cThe total number of COVID-19 patients with and without FS was 6 and 559, respectively.
Discussion
The prevalence of FS in pediatric COVID-19 patients varies across studies and regions, ranging from 0.19% to 4.5%,11-14 with rates during the Omicron wave reaching 5.74-13.0%.11,13,16 In Jeonbuk, South Korea, a study reported that 0.19% of children under five experienced FS following the Omicron surge. 14 In Brunei, 4.5% of COVID-19-positive children under 12 years had FS, with occurrences solely during the Omicron wave. 11 A multicenter US cohort reported that 0.5% of COVID-19-positive patients aged 0-5 had FS, 13 while another study noted a 2.7% prevalence in children aged 6-60 months. 12 There are limited studies on FS prevalence in COVID-19 cases in Thailand. Our research found an overall prevalence of 0.36% among pediatric COVID-19 patients and 1.31% in those aged 6-60 months, mainly during Omicron period. Similarly, other studies reported an increase in FS during the Omicron period, suggesting that this variant may trigger FS more than earlier strains.11,14,16 However, our study did not include virological confirmation of specific SARS-CoV-2 variants. Consequently, we were unable to determine whether FS associated with COVID-19 during the Omicron period was directly attributable to the Omicron variant or whether this variant confers a higher risk of FS compared with other variants.
Most FS cases across all groups (including by period or COVID-19 status) were simple, although complex FS was more common among COVID-19 cases than without COVID-19 (33.33% vs. 20%). Literature indicates that around 70% of FS are simple, 25% are complex, and 5% are febrile status epilepticus. 17 Multiple studies confirm an increased incidence of FS, including complex cases, in pediatric COVID-19 patients, in which complex seizures comprise 20–40% of COVID-19-related FS.11,14,18-20 The Omicron variant is associated with higher rates of both febrile and complex FS than earlier strains, with children experiencing longer seizures and a later onset of FS compared to other infections.14,16,18,20,21
FS incidence peaks between 12 and 18 months, with 90% occurring at age 36 months.22,23 Our median ages in months (IQR) for FS during the pre-Omicron and transition periods were 18 (14-26) and 14 (9-21), respectively. The median ages in months (median, IQR) for FS during the Omicron period (22,13-30.5) and for FS with COVID-19 (27,16-31) were older than the overall FS and those without COVID-19 (20,13-29), aligning with the predominant age range of 12-30 months.11,23 However, no significant age differences were found across periods or between those with and without COVID-19.
There was a male predominance in FS overall, consistent across groups and periods, like pre-COVID-19 data.22,24,25 Notably, we observed a significant male predominance in COVID-19 patients experiencing FS compared to those without FS. Similarly, a study from China reported that the proportion of males in FS with COVID-19 was significantly higher than that of females, 19 suggesting heightened awareness of FS risks in male patients aged 6-60 months. Research also suggests males tend to experience more severe COVID-19 outcomes, including ICU admissions and length of hospital stays. 26 Possible reasons include higher levels of inflammatory cytokines like IL-6 and TNF-α in males associated with poorer COVID-19 outcomes, while females often demonstrate stronger T cell responses, potentially leading to better outcomes.27-29 However, no significant sex differences in severity, mortality, or FS incidence have been reported in children. 19
The leading causes of FS during the pandemic were upper respiratory and unspecified viral infections, consistent with previous findings.5,24,25 Several studies show the risk of FS with COVID-19 is similar to other viral infections, indicating COVID-19 does not increase FS risk beyond typical patterns.12,13,30,31
Our study found a shorter duration of fever before seizure and higher serum sodium in the transition period, possibly due to the longer duration of fever attributed to the lower serum sodium level in the pre-Omicron and Omicron periods. Moreover, the most common causes of FS in the pre-Omicron and Omicron periods were respiratory infections, viral infections, and gastroenteritis. Previous research has associated hyponatremia with FS related to viral infections, including respiratory viruses and SARS-CoV-2 (COVID-19), implicating infection-induced inflammation and dysregulation of antidiuretic hormone (ADH).32-36 Gastrointestinal losses from vomiting or diarrhea during viral illnesses may also contribute to hypovolemia and sodium loss.37,38 However, the underlying mechanisms remain poorly understood.
Our study found that cough was a more prominent symptom in FS cases without COVID-19 compared to those with COVID-19. In contrast, a recent study comparing hospitalized children with FS, regardless of COVID-19 status, reported very similar clinical presentations in both groups, with no significant differences in the frequency of cough or rhinorrhea. This suggests that cough does not occur more often in COVID-19-negative FS cases than in positive ones. 31
In addition, our results showed that COVID-19-positive patients without FS exhibited more pronounced respiratory symptoms (p = 0.007), including cough (p = 0.030), compared to those with FS. Similarly, a Wuhan study, on FS risk in children during the Omicron surge, found that cough was inversely related to FS in COVID-19-positive cases. 39 Similarly, a study from Brunei indicated that children who had COVID-19 with FS had fewer additional symptoms at presentation compared to those without FS. 11
Additionally, our findings showed that patients with COVID-19 infection and FS had significantly elevated BT (39.13°C vs 37.37°C, p=0.000), PR (178.11 bpm vs 127.95 bpm, p=0.000), and RR (36.33/min vs 28.16/min, p=0.021) compared to those without FS. These findings may help raise awareness of the FS risk associated with COVID-19 infection. As highlighted in the Brunei study, higher fever, younger age, and family history of FS were identified as risk factors for FS in children with COVID-19 infection. 11
There are some limitations to our study. First, this is a single-center, retrospective, observational study; some information was unavailable, including CBC, electrolytes, LFT, inflammatory markers (CRP/ESR), and viral panels. Second, our study’s small sample size, especially in the transition period, may not represent the exact prevalence and risk factors of FS in COVID-19 cases. Third, the semiology of seizures and the time of fever before seizure onset, which were collected from the guardian’s statement and medical record, might be inaccurate. Fourth, we did not know the exact COVID-19 strain of cases in all periods because we could not identify the viral strain. Further large-scale, prospective studies with well-designed methods, including the testing of laboratory and inflammatory markers, as well as viral panels, are essential.
Conclusions
COVID-19 does not increase the risk of FS compared to other causes. Male gender, higher body temperature, pulse and respiratory rate in COVID-19 children are associated with FS. Cough was a less relevant symptom for FS in COVID-19 children. Well-designed, large-scale research is needed to better understand FS in pediatric COVID-19 patients.
Footnotes
Acknowledgements
We thank all patients and the Faculty of Medicine, Srinakharinwirot University, Thailand, for their support.
Ethical Considerations
This Study Was Conducted in Accordance with the Principles of the Declaration of Helsinki and Was Expedited and Approved by the Institutional Ethics Committee for Human Research. This study was performed in line with the principles of the Declaration of Helsinki, with expedited review and approval by Srinakharinwirot University Ethics Committee (SWUEC-673004).
Author Contributions
Acharaporn Maksikharin and Olarn Prommalikit substantially contributed to the project by participating in the conception and design, aiding in data acquisition, analysis, and interpretation, drafting and revising the manuscripts, and giving final approval.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Srinakharinwirot University funding (NO 401/2567). The authors declare no relevant financial or non-financial interests.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The complete datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.