
Abstract
Background:
Typically, mothers are the primary caregivers for their children; therefore, their knowledge and attitude towards febrile seizures impact the management of this condition in the home environment.
Aims:
This study is designed to explore mothers’ knowledge, attitudes towards managing febrile seizures at home, and the correlation between socio-demographic variables and knowledge and attitudes towards managing febrile seizures.
Methods:
This research adopted a cross-sectional design consisting of a convenience sample of 84 mothers who had attended a paediatric clinic or accompanied their child during hospitalisation at two public hospitals in northern Jordan between August 2021 and December 2021. The data employed by this study were gathered via a valid structured questionnaire that was adapted from the work of Elbilgahy and Abd El Aziz.
Results:
This study revealed that 63.6% of participants possessed a good knowledge of the condition, and that 63.1% of participants exhibited positive attitudes towards febrile seizure management. In addition, there was a significant positive correlation between the knowledge and attitude scores (r = 0.274, p = 0.012) of mothers regarding the management of febrile seizures in children. Furthermore, the findings of this study indicate that the educational level of mothers was only an associated factor of knowledge (B = −0.821, p = 0.034).
Conclusion:
Mothers demonstrated generally good knowledge and positive attitudes towards febrile seizure management; however, important misconceptions persist. Targeted educational interventions by healthcare professionals are needed to improve safe home management and support parental confidence.
Introduction
According to recent global epidemiological data, febrile seizures (FSs) affect ~1%–4% of children aged 6 months–5 years, with notable differences in prevalence among demographic groups. 1 These seizures, resulting from fever (38 °C or higher), are usually benign and self-limiting; however, they can be distressing for caregivers. 2 Long-term outcomes are generally positive, though a subset of children with complicated FSs may develop epilepsy. 3
Currently, mothers bear the primary responsibility for recognising and managing FSs, yet many hold misconceptions that can lead to potentially harmful practices. Studies show inadequate maternal knowledge of FSs and appropriate treatment, which potentially endangers immediate and long-term health outcomes for affected children. 4 For instance, a Nigerian study highlighted gaps in caregivers’ first aid knowledge, 5 while research in Indonesia found that higher maternal knowledge correlates with better home management of FSs. 6
However, even knowledgeable mothers sometimes struggle to apply their knowledge in high-pressure situations, emphasising the need for practical training over merely theoretical instruction. Moreover, misconceptions about FSs and their association with epilepsy are prevalent across different regions, including the Middle East,1,7 where a Baghdad study indicated a low mean knowledge score among mothers. 1 In Jordan, significant anxiety and uncertainty regarding FS management were observed, coupled with a lack of educational programs. This study aims to assess mothers’ knowledge and attitudes towards managing FSs in children under 6 years, intending to inform the development of culturally appropriate educational programmes to enhance maternal competence and reduce anxiety related to FS management. 8
This study seeks to address the current knowledge gap by evaluating mothers’ knowledge and attitudes concerning the home management of FSs in children under 6 years of age. Its findings will guide the creation of culturally relevant teaching programmes to empower mothers, alleviate anxiety, and enhance safer FS management.
The Health Belief Model
The Health Belief Model (HBM) was selected as the theoretical framework for this study because it explains health-related behaviours based on individuals’ knowledge, perceptions, and beliefs. Since the present study focusses on mothers’ knowledge and attitudes towards managing FSs at home, the HBM provides an appropriate framework to understand how perceived severity, perceived benefits, perceived barriers, and self-efficacy may influence mothers’ responses to FS episodes.
The knowledge of mothers and their attitudes to the management of FSs demonstrate the main HBM constructs; therefore, the findings of this research can be discussed in terms of the HBM. 9 The perceived severity of FS correlates with mothers recognising it as a severe condition, whereas the perceived benefits are represented via mothers recognising the use of appropriate management techniques. Inferior knowledge (or misunderstanding) can be perceived as a barrier to effective treatment, and mothers’ confidence in managing FSs in the home environment is associated with self-efficacy. Using the HBM framework, it is essential to emphasise the necessity for customised nursing interventions to improve maternal knowledge, reduce the obstacles, and increase confidence in safe home management.
Despite previous studies examining parental knowledge and attitudes towards FSs, limited research has explored this topic within the Jordanian context, particularly among mothers of children already diagnosed with FSs. In addition, few studies have simultaneously examined the relationship between maternal knowledge and attitudes and their associated factors. Therefore, the present study adds context-specific evidence that may support the development of targeted educational interventions for improving home management practices.
Study context
Jordan is a developing country in the Middle East, characterised by healthcare issues influenced by its socio-economic conditions and culture. Despite advancements in the healthcare system, it continues to face several challenges (such as health literacy levels and service accessibility), particularly in rural regions. 6 The treatment of common childhood ailments (such as fever and FSs) is typically guided by traditional beliefs and practices, which significantly contribute to health-seeking behaviours. 10 Such findings highlight the need for context-bound studies that will clarify the underlying dynamics of parental knowledge and attitudes towards child health management. The findings of research conducted in this particular cultural and medical context are essential to the creation of focussed and effective health interventions and education programmes that are culturally responsive and practically feasible for Jordanian families. 11
Study aim
This study aimed to assess mothers’ knowledge and attitudes towards the home management of FSs in children and to examine the relationship between these factors and selected socio-demographic characteristics.
Method
Design
This research employed a cross-sectional descriptive survey design, which is recognised as suitable for research concerning health and social sciences because it allows researchers to gather data at a single point in time to describe the characteristics, attitudes, behaviours, or conditions of a specific population. 12 This cross-sectional study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
Settings
The current research was conducted in the outpatient clinics and paediatric wards of two public hospitals that serve several government-related areas in northern Jordan. They are specialist paediatric hospitals which provide both curative and preventive care services for children. Primarily, these public hospitals are accessed by low- to mid-level income individuals (who represent the majority of the population in northern Jordan).
Sample and sampling
A convenient sampling strategy was employed to recruit participants. The inclusion criteria for participants were as follows: (1) Mothers who had visited a paediatric clinic or accompanied their child to the paediatric ward at Previous history of maternal health and between August 2021 and December 2021, and (2) mothers with children under 6 years of age with first or recurrent FSs. It should be noted that the mothers of children who suffered from seizure-related metabolic disorders or neurological disorders were excluded from this study.
Children with both first and recurrent FSs were included to reflect the range of clinical presentations among affected children. To address potential bias related to prior experience, additional analyses were conducted comparing mothers of children with single versus recurrent FSs, and no statistically significant differences were found in knowledge or attitude scores.
Data were collected at a single time point for each participant. Each mother was enrolled only once during the study period, and repeat visits were not included in the dataset to avoid duplicate entries. In the Jordanian context, mothers are typically the primary caregivers and are most frequently responsible for accompanying children during hospital visits; therefore, participant recruitment was limited to mothers. Cohen 13 suggested using a minimum of 84 participants with a significance level of 0.05, a medium effect (d = 0.5), power of 0.8. Based on the general rule of thumb, N ⩾ 50 + 8 m. We had four predictors in this study, so the minimal sample size was 84 mothers who were enrolled in the study.
Instruments
The data were collected via a questionnaire developed by Elbilgahy and Abd El Aziz,14 which was adapted to conduct structured interviews with mothers. The questionnaire was based on the prior validated instrument created by Elbilgahy and Abd El Aziz.14 To be clear and culturally appropriate, the tool was given in Arabic, the native language of the participants. Data collection was preceded by content validity reviews by experts in the fields of paediatric nursing and maternal child health. Internal consistency reliability of the questionnaire was assessed using Cronbach’s alpha coefficient. The results demonstrated acceptable reliability, with a Cronbach’s alpha of 0.86 for the knowledge scale and 0.86 for the attitude scale, indicating good internal consistency. The instrument consists of four sections:
Part 1: Demographic data and seizure characteristics
This section consisted of 10 items: maternal age, education level, child’s age, child’s gender, child’s age at the first occurrence of FS, number of children who had experienced a FS, frequency of FS, duration of FS, immediate action taken for your child during FS, and signs and symptoms pre, during, and after the FS. Socio-economic status was partially reflected through maternal educational level, which was included among the socio-demographic variables; however, detailed socio-economic indicators such as household income were not collected.
Part 2: Mothers’ knowledge about FS
This section consisted of 12 questions concerning mothers’ knowledge of FSs, including definition, signs and symptoms, incidence, and the consequences of FSs for children. The knowledge section was based on dichotomous questions (correct/incorrect answers) in order to objectively measure the factual knowledge of mothers about FSs. This scoring method is widely employed in the measurement of the knowledge-based outcomes. This section was tested for reliability via an alpha Cronbach’s test, which revealed that the reliability of this section was (alpha = 0.86), which is above the generally accepted (alpha = 0.70). To evaluate maternal knowledge, each correct response was assigned a score of one, while incorrect responses were scored zero. Subsequently, the total knowledge scores were categorised as follows: scores of 60% or higher indicated good knowledge, scores between 55% and 59% reflected average knowledge, and scores below 55% were considered indicative of poor knowledge, in accordance with the classification system proposed by Elbilgahy and Abd El Aziz.14
Part 3: Mothers’ attitudes towards FSs
This section included eight items measured using a five-point Likert scale 15 to assess mothers’ attitudes towards FS management. It was tested for reliability using an alpha Cronbach’s test. In contrast to knowledge, attitudes were measured using Likert-scale items to capture mothers’ perceptions and beliefs towards FS management. The Cronbach’s alpha for this section was (alpha = 0.86), which exceeds the generally accepted level (alpha = 0.70). These references are in accordance with the classification system proposed by Elbilgahy and Abd El Aziz.14 The distribution of the attitude scores was tested using the Kolmogorov–Smirnov test and was found to be approximately normal. Therefore, the mean attitude score of 3.32 was used as the cut-off point to classify maternal attitudes. Scores of 3.32 or higher indicated a positive attitude, while scores below 3.32 indicated a negative attitude. The questionnaire used in this study is provided as Supplemental File 1.
Data collection procedure
This study employed quantitative data collection after obtaining the Institutional Review Board (IRB) number (2021/333) from the Jordan University of Science and Technology, and official authorisation from the Royal Medical Service and the Ministry of Health. The employment of a quantitative research design facilitates the objective measurement and analysis of mothers’ knowledge and attitudes towards FSs. In addition, a quantitative design allows for the collection of numerical data, which can be statistically analysed to identify percentages, frequencies, and correlations between variables.
This research was conducted with mothers during their visits to the paediatric clinic with their child, or when accompanying their child during admission to the paediatric ward in the selected hospitals. Before the study, the researcher described the study’s purpose to the participants and explained that their participation was entirely voluntary, no harm would arise from participating, and that those who decided not to participate would not be discriminated against during treatment.
Subsequently, the researcher prepared 84 participant information packages consisting of: Arabic language questionnaires, a cover letter detailing the aims of the research, a participant confidentiality form, a participant consent form, and the researcher’s contact information. After receiving signed consent forms, 5–10-min, face-to-face structured interviews were conducted by the researcher, either in the outpatient clinic waiting room or in the paediatric ward.
Data analysis
The data was analysed using Statistical Package for the Social Sciences (SPSS) version 26 (IBM Corp., Armonk, NY, USA). Descriptive statistics (such as frequency, standard deviation, mean, median, and percentage) were used to describe the main variables in the study and compare them with other findings listed in the literature. Pearson correlation analysis was employed to test the relationship between the level of knowledge and attitudes towards the management of FSs at home. Knowledge and attitude variables were computed as sum scores and regarded as continuous variables. We tested the normality of the distributions by the Kolmogorov–Smirnov test and found it to be normal (p > 0.05). In this regard, the Pearson product-moment correlation coefficient was employed to test the relationship between the attitude and knowledge of mothers. Two multiple linear regression analyses were done. The former considered the predictors of the knowledge of mothers concerning FSs, whereby the dependent variable is the knowledge score, and the independent variables are such factors as child- and mother-related socio-demographic factors. In the second model, the predictor of attitudes of the mothers towards FSs was considered, and the attitude score was considered as the dependent variable, whereas the covariates were entered as independent variables. A stepwise backward elimination approach was conducted on the likelihood of the F statistic, with entry and removal levels being 0.05 and 0.10, respectively. To prevent the loss of data during the data collection phase, the researcher used clear and simple questions. Additionally, to ensure participant comfort, the interviews were conducted in the clinic waiting areas after the child had been admitted.
Ethical considerations
Ethical approval for this study was obtained from the IRB of Jordan University of Science and Technology (2021/333). Furthermore, official authorisation was obtained from the Royal Medical Services and the Ministry of Health to conduct the research at Previous health behaviour history and Previous related treatment history.
Results
Socio-demographic characteristics of mothers and children
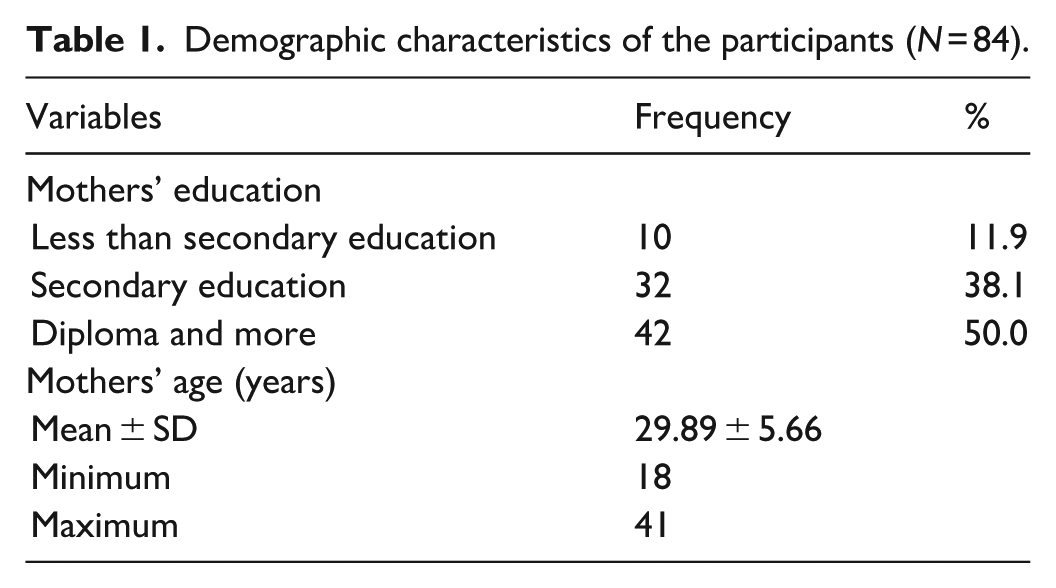
Participant recruitment and study flow are presented in Figure 1. The mean age of mothers was 29.89 ± 5.66 years, and ~50% (N = 42) of mothers had a diploma degree or higher educational level. Table 1 summarises the socio-demographic characteristics of the participating mothers.

Participant recruitment and study flow.
Demographic characteristics of the participants (N = 84).
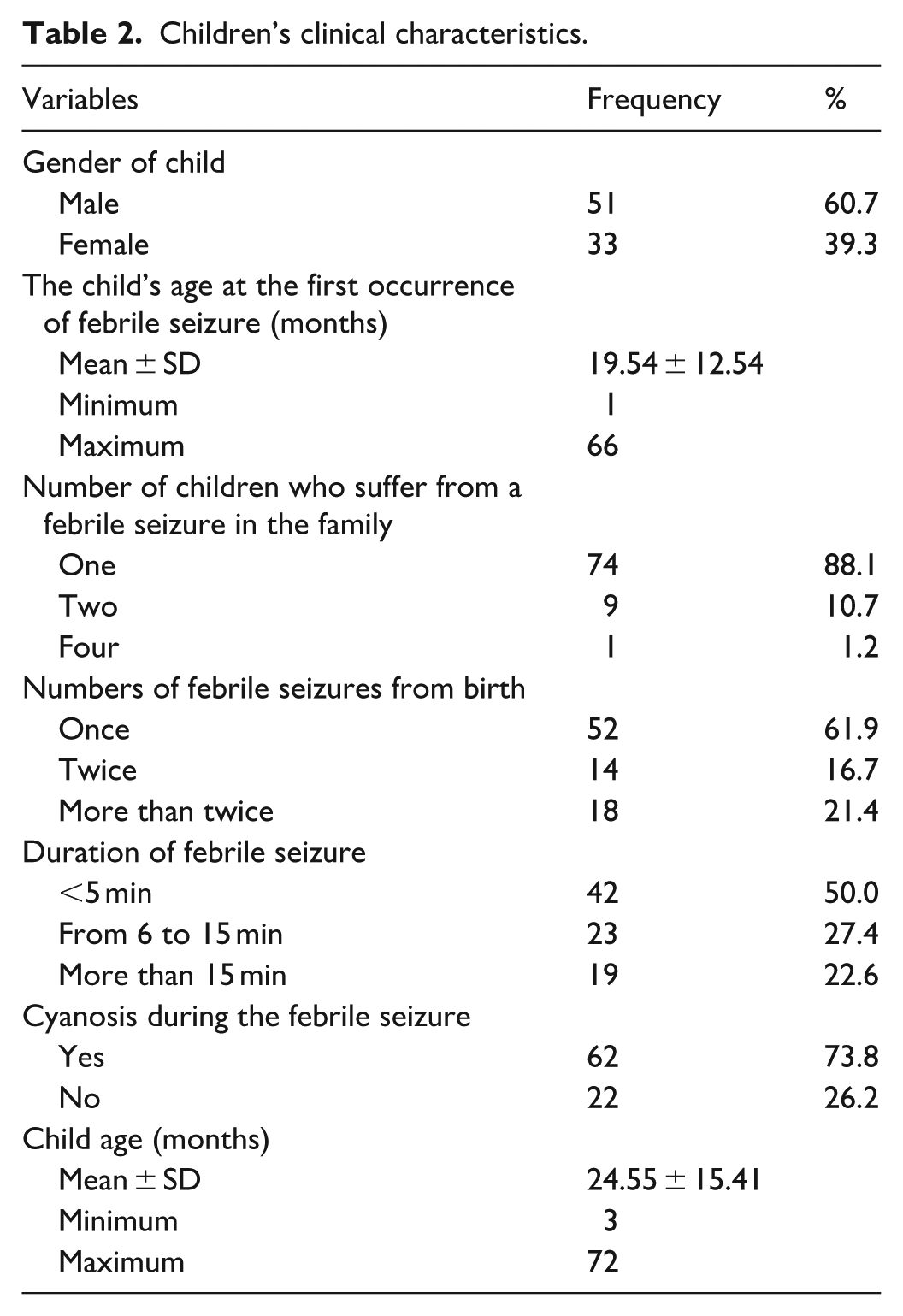
The mean age of children was 24.55 ± 15.41 months, and 60.7% of children with FS were male. The mean age of the occurrence of FS attack was 19.54 ± 12.54 months, and 61.9% of the children with FS had experienced one FS since birth. Additionally, in half of the children, 50% of FSs had lasted for <5 min, and ~73.8% of children had experienced cyanosis during a FS. The majority of mothers (88.1%) have one child who suffers from FSs. The clinical characteristics of the children with FSs are summarised in Table 2.
Children’s clinical characteristics.
Mothers’ knowledge of FSs
The majority of participating mothers (83.3%) were able to correctly define a FS, 91.7% knew the indicators and symptoms of FS, 83.3% knew that FS is rare after the age of 5 years, and 72.6% indicated that it is safe to give routine immunisation to children who had experienced a FS. However, it should be noted that only 17.9% of participants knew that FSs do not cause brain damage, and only 39.3% of participants gave correct answers concerning the measures used to prevent FSs. Approximately 54.8% of mothers answered correctly when asked about placing protective devices inside the mouth during a FS, 58.3% provided the correct answer concerning restraining the child, and 65.5% of mothers responded correctly when asked about administering cardiopulmonary resuscitation during a FS. According to the scoring criteria employed by this research, ~63.6% of participants demonstrated a ‘good’ level of knowledge about FSs. Mothers’ knowledge regarding FSs is presented in Table 3.
Mothers’ knowledge of febrile seizures.
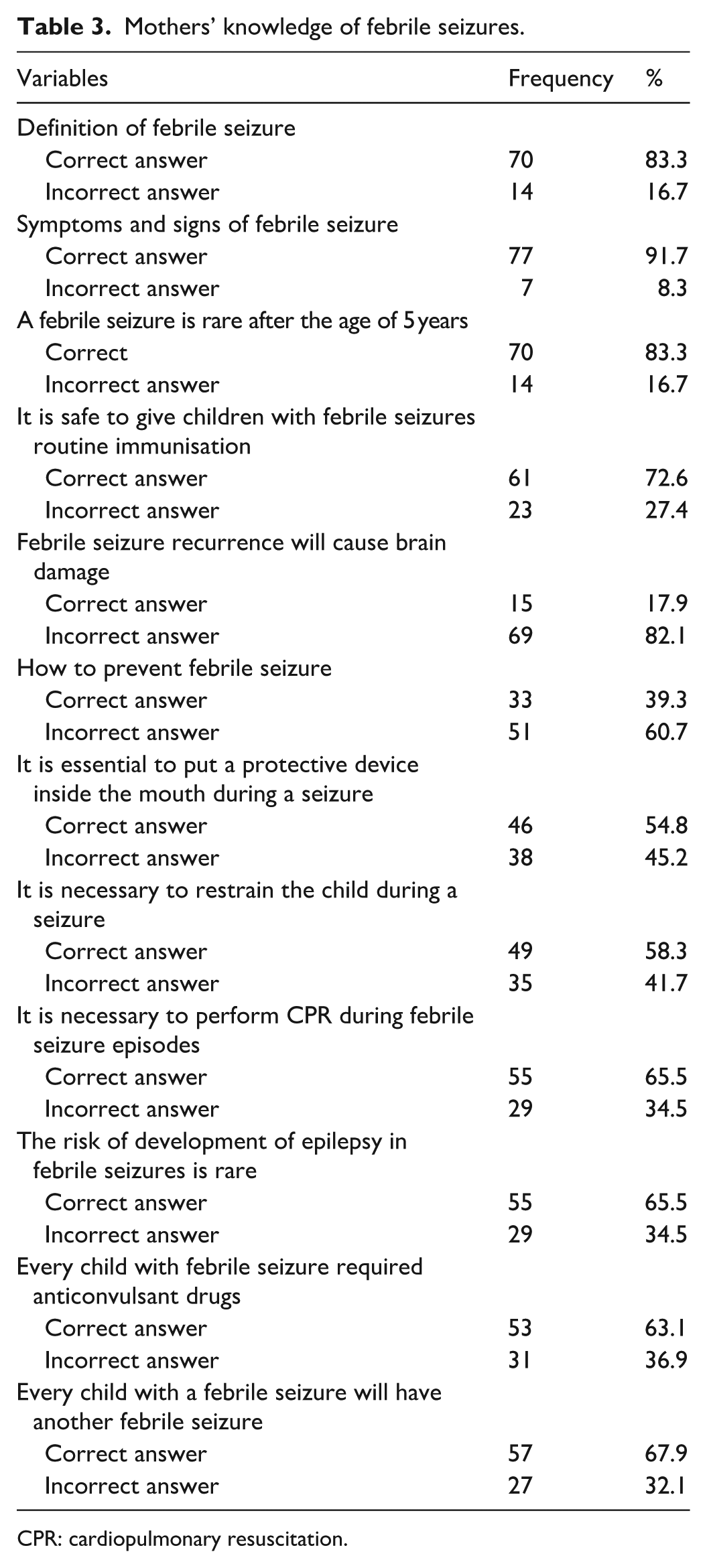
CPR: cardiopulmonary resuscitation.
Mothers’ attitudes regarding FS
Approximately 70.3% of mothers did not agree that FSs are caused by evil spirits. Additionally, when questioned about the seriousness of FSs, about 70.3% of mothers believed that FSs are life-threatening conditions, and 71.4% of mothers believed that FSs cause brain damage. Furthermore, about 95.3% of mothers agreed that they should frequently measure a child’s body temperature. Approximately 89.3% of studied mothers believed that children with FSs required more love and care. These findings revealed that 53 (63.1%) of mothers displayed a positive attitude towards FS, whereas 31 (36.9%) of mothers demonstrated a negative attitude towards the condition. Mothers’ attitudes towards FSs are shown in Table 4.
Mothers’ attitudes towards febrile seizures.

Correlation between mothers’ knowledge and attitudes
A significant weak correlation was found between the participants’ knowledge score and their attitudes score (r = 0.274, p = 0.012), implying that more positive attitudes are somewhat correlated with greater knowledge levels. Independent samples t-tests were conducted to compare knowledge and attitude scores between mothers of children with single versus recurrent FSs. No statistically significant differences were found in knowledge scores (t = 0.57, p = 0.568) or attitude scores (t = −0.57, p = 0.571) between the two groups. The correlation between mothers’ knowledge and attitude scores is presented in Table 5.
Correlation between mothers’ knowledge and attitude scores.

p < 0.05.
Associated factors of mothers’ knowledge
Knowledge of FSs was significantly predicted by maternal education. Specifically, mothers with only secondary education were associated with a lower knowledge score than mothers with a diploma or higher level of education (B = −0.821, t = −2.160, p = 0.034). The factors associated with mothers’ knowledge are presented in Table 6.
Factors associated with mothers’ knowledge. Multiple linear regression analysis of factors associated with mothers’ knowledge.

Model statistics: F = 3.193, R2 = 0.073, p = 0.046.
Associated factors of mothers’ attitudes
Mothers’ attitudes towards FSs were not found to be significantly predicted by any of the socio-demographic factors (such as the number of FS episodes, the gender of the child, or the mother’s age). Although the overall regression model was statistically significant, none of the individual socio-demographic variables showed a significant independent association with mothers’ attitude scores. The factors associated with mothers’ attitudes are shown in Table 7.
Factors associated with mothers’ attitudes towards febrile seizures (multiple linear regression).

Discussion
This study aimed to investigate mothers’ knowledge and attitudes concerning the management of FSs at home, as well as the correlation between socio-demographic variables and mothers’ knowledge and attitudes towards the management of FSs. The findings of this research indicate that mothers have a good knowledge of FSs and positive attitudes towards the management of FSs at home. In addition, this study’s findings indicate that the mothers’ knowledge demonstrates a positive correlation with their attitude, and that the mothers’ level of education is the only predictor for their knowledge.
However, this finding does not align with Almousa et al., 16 who reported that more than two-thirds of parents in Saudi Arabia demonstrated poor knowledge of FSs and less than one-quarter had positive attitudes towards the condition. Furthermore, a study conducted in Jordan reported that mothers demonstrated poor knowledge and high anxiety regarding FSs. 8
The data gathered for this research revealed that the mean age of the mothers was 29.89 ± 5.66 years, and that ~50% of them have a high level of education (i.e. a diploma or higher). Additionally, 61.9% of children with FS have had one FS since birth, 50% of these FSs lasted for <5 min, and ~73.8% of children experienced cyanosis during their FS. The majority of mothers (88.1%) have one child who suffers from FSs. These characteristic factors are essential as they provide context for knowing the mother’s knowledge and attitude towards managing FSs at home.
The current study reveals the high levels of maternal awareness regarding the definition of FSs and their occurrence after 5 years. These results are higher than those reported in a study conducted in Egypt, where mothers initially demonstrated limited knowledge regarding febrile convulsions before the implementation of an educational intervention. 14 This discrepancy in the findings may be related to the fact that over one-third of the children in the current sample had experienced recurrent FSs. Although the statistical comparison between mothers of children with single and recurrent episodes was not significant, prior exposure to seizure events may still increase maternal familiarity with the condition and contribute to higher awareness levels. In the present study, however, the difference in the level of knowledge and attitude between mothers with single and recurrent FSs was not found to be significant. This observation could be an indication that maternal knowledge or attitudes are not automatically enhanced by previous experience of seizure, and this means the need to implement structured educational interventions despite the absence or recurrence of seizures.
In addition, over half of the mothers held a diploma or higher educational level, which may have enhanced their ability to understand FSs and their management. The present study found that maternal education was associated with higher knowledge scores, suggesting that mothers with higher education levels may have greater access to health information and a better understanding of instructions provided by healthcare professionals. This finding highlights the importance of structured health education for mothers following their child’s admission. Furthermore, mothers were more knowledgeable regarding the signs and symptoms of FSs, which may be related to their direct exposure to seizure episodes, such as prolonged seizures, cyanosis, and recurrence. This finding is consistent with a study conducted in Nepal, which reported moderate levels of maternal knowledge regarding different aspects of febrile convulsions, including clinical manifestations and management. 17
This research highlights some persistent misconceptions concerning the complications of FSs. This study reveals that most mothers believe that brain damage occurs during a seizure, and this correlates with previous findings indicating that many parents perceive FSs as life-threatening events. 18 In addition, this result corresponds with a study conducted in Iran, which reported that ~90% of mothers believe that the recurrence of FSs will cause brain damage. 19 The current study indicates that most mothers perceive antipyretics as preventive, reflecting a dependence on symptomatic management, which may suggest a limited comprehension of seizure pathophysiology. This finding is consistent with Kheir et al.,20 who identified a significant reliance on paracetamol and sponging, implying that these beliefs may be regionally prevalent. 20 Furthermore, although mothers have a good knowledge of FS management, more than 40% of the participants in this study believed that it was essential to place a protective device inside the patient’s mouth and to restrain them during a seizure. This misconception can be attributed to the fact that the mothers believe that such actions are necessary to protect the child from serious harm (such as tongue biting), which reflects an overestimation of the perceived benefits of these harmful practices. Similar misconceptions have been reported in previous studies, where a considerable proportion of mothers attempted to open the child’s mouth or place objects between the teeth during a seizure. 19 These findings highlight the persistence of harmful misconceptions and emphasise the need for healthcare professionals to provide clear education on safe seizure first-aid practices.
Furthermore, the current study reveals the concerns and beliefs of mothers regarding FSs, which reflect a combination of accurate knowledge and some misconceptions. More than 70% of mothers believe that FS episodes are a life-threatening event and that the child requires more love and care. This finding can be rationalised by the perceived severity and beliefs of mothers concerning FSs, and aligns with a study conducted in Aseer, Saudi Arabia. 7 The similarity between the two studies can be attributed to similarities in the culture of the participants.
In the present study, maternal attitudes towards FSs were not significantly associated with the examined socio-demographic covariates. This finding may suggest that attitudes are influenced more by emotional responses, uncertainty, and personal perceptions rather than demographic characteristics alone. Recent evidence from Jordan has shown that mothers of children with FSs experience high levels of anxiety and uncertainty, which may shape their perceptions and reactions towards seizure management regardless of background characteristics. 8 Therefore, educational interventions should not only focus on improving factual knowledge but also address emotional concerns and misconceptions to support more positive caregiving attitudes and safer home management practices.
Contrastingly, a small percentage of mothers (21%) believed that the FSs experienced by their children were caused by evil spirits. The decline in this belief among mothers reflects improved perceived susceptibility and cues to action within the HBM, as mothers increasingly rely on scientific explanations. This shift indicates greater self-efficacy and reduced dependence on cultural myths in managing their children’s condition. Similar misconceptions related to cultural beliefs about FSs have been reported in previous studies. 21
This study revealed that almost 95% of mothers believed they should frequently take their children’s temperature. This high percentage may be reflective of robust perceived susceptibility and perceived severity, as mothers associate fever with the risk of complications (such as FSs). Additionally, the escalation in the frequency of monitoring temperature reflects mothers’ perceptions that the early detection of a fever is a preventive action to protect the child. This aligns with findings from a study in Qatar, which reported that 95.7% of parents believed untreated fever could cause harm. 22 These findings further reinforce how health education and prior caregiving experiences shape mothers’ health beliefs and drive preventive practices.
Finally, no significant differences were observed in knowledge or attitude scores between mothers of children with single versus recurrent FSs. This finding suggests that prior experience with seizure recurrence alone may not necessarily improve maternal knowledge or attitudes, highlighting the importance of structured educational interventions regardless of seizure frequency.
Clinical implications for paediatric practice
The results emphasise the need to focus on the collective role of paediatricians and nurses in assisting parents through one of the most traumatic childhood illnesses. A few mothers in the present study exhibited misconceptions about FSs, especially the fears of brain damage and dangerous first-aid measures like putting something in the mouth of the child during a seizure. Thus, it is advised to include structured nurse-led education immediately after the first encounter with FSs to correct the misconceptions, increase maternal confidence, and ensure safe practices at home. The implementation of very short, evidence-based educational programmes in paediatric clinics and hospital wards could help to minimise the number of unnecessary emergency visits, lessen parental anxiety, and improve child safety during seizure episodes.
Limitations
Although this study provides valuable insight into mothers’ knowledge and attitudes towards home management of FSs, several limitations should be acknowledged. First, the use of a convenience sample from only two public hospitals may limit the generalisability of the findings to all Jordanian mothers, especially those living in rural or remote areas with different cultural and educational backgrounds. Second, the sample size was relatively small. Stratified analyses based on the number of FS episodes or the number of affected children within the family were not performed due to the limited sample size within subgroups. In addition, the cross-sectional design limits causal interpretation. Third, data were collected through self-reported interviews, which may have introduced social desirability bias, as some mothers might have provided answers they believed were expected by the researcher. Further, because this was a cross-sectional study, it was not possible to establish cause-and-effect relationships between mothers’ knowledge, attitudes, and socio-demographic factors. Finally, the present study focussed on mothers’ knowledge and attitudes towards FSs. Practice-related items were analysed separately and will be reported in a different article to allow more detailed interpretation.
Conclusion
This research concluded that there was a reasonably good level of knowledge and positive attitude among mothers regarding the home management of FSs, although a number of misconceptions and unsafe first-aid practices were still observed. The positive correlation between knowledge and attitudes implies that maternal knowledge enhancement can help to increase the likelihood of an appropriate reaction to seizure episodes. The results highlight the significant role of nurses and paediatric healthcare professionals in the provision of structured evidence-based education to enhance safe home management, lower the anxiety of parents, and lead to better caregiving outcomes. It is advisable that future studies be conducted on larger and more diverse samples to explore more factors that affect maternal knowledge and attitudes and to determine the efficacy of specific educational interventions.
Supplemental Material
sj-docx-1-smo-10.1177_20503121261438377 – Supplemental material for Knowledge and attitude of mother towards home management of febrile seizure in children: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121261438377 for Knowledge and attitude of mother towards home management of febrile seizure in children: A cross-sectional study by Nouraldun M. Alhsenat, Huda Gharaibeh, Maha Atout and Fatimah S. Tarawneh in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank all participating mothers and the healthcare staff who facilitated data collection.
Ethical considerations
This study employed quantitative data collection after obtaining ethical approval (IRB no. 2021/333) from the Jordan University of Science and Technology Institutional Review Board. Official authorisation was also granted by the Royal Medical Service and the Ministry of Health prior to data collection.
Consent to participate
Written informed consent was obtained from all participating mothers prior to data collection.
Author contributions
N.M.A. takes responsibility for the content of the article and contributed to the study protocol, data collection, data analysis and interpretation, and writing, H.G. contributed to the study protocol, data collection, data analysis and interpretation. M.A. and F.S.T. contributed to data analysis, data interpretation, writing of the article and submission. All authors discussed the results and contributed to the final article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analysed during the current study are not publicly available due to confidentiality and ethical restrictions but are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.