
Abstract
Background:
Heart failure (HF) affects over 6 million people in the United States and is a frequent cause of hospital readmissions. While interest in individual HF interventions like digital platforms and home-based care delivered by community health workers (CHWs) has risen, few studies have explored barriers and facilitators to engaging CHWs with digital or remote monitoring devices in HF populations.
Methods:
Three virtual focus groups were conducted from December 2020 to January 2021 with 14 CHWs. Key domains included: barriers and facilitators to managing HF at home; CHW care in HF; remote monitoring and technology in HF; and CHW ability to assist with remote technology in HF.
Objective:
To explore CHW perceptions about managing HF at home relevant to the use of home-based remote monitoring.
Findings:
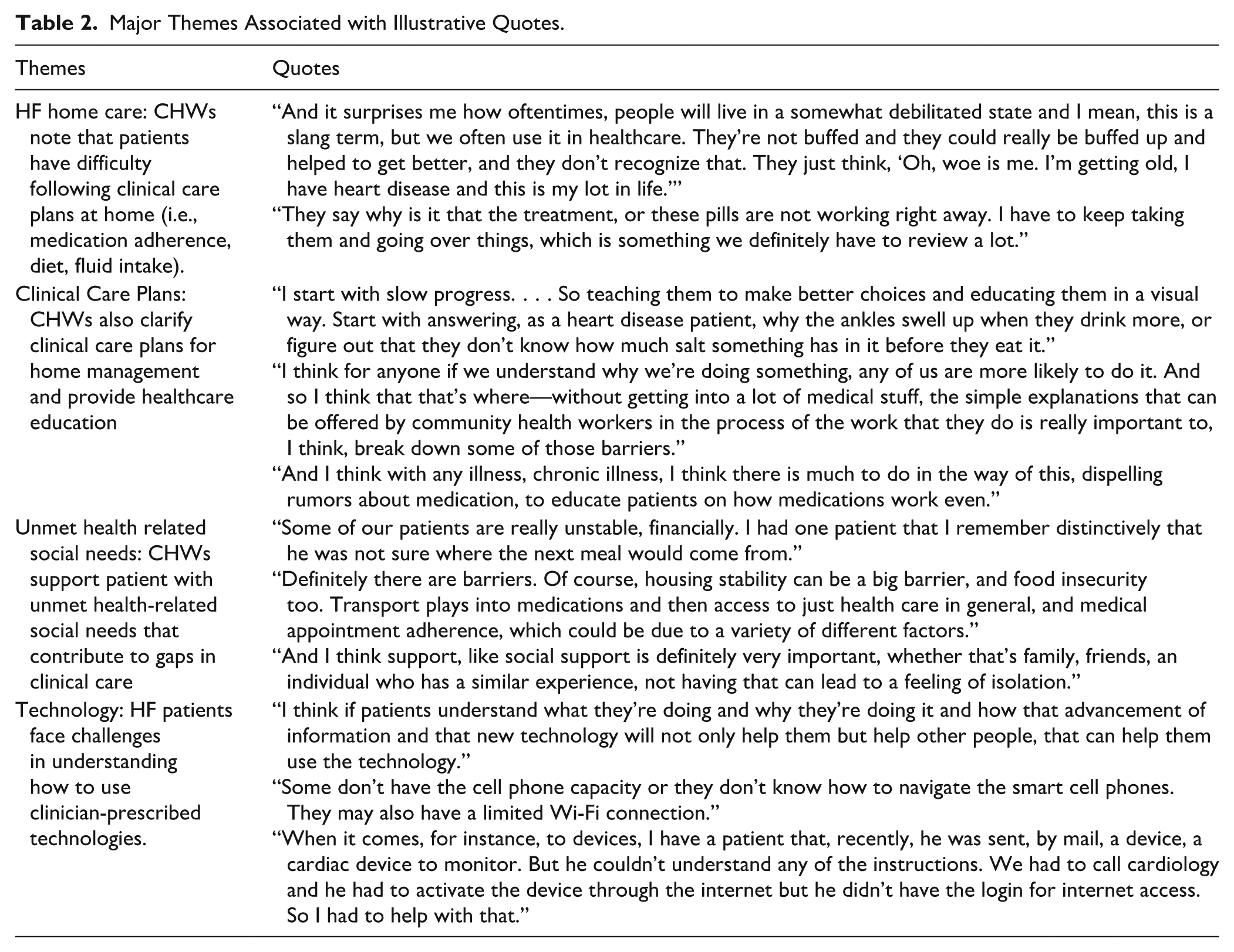
Focus groups produced 4 themes: (1) patients with HF struggle to follow clinical care plans at home (i.e., medication adherence, diet, fluid intake); (2) CHWs clarify clinical care plans and provide psychosocial support; (3) CHWs connect patients to resources addressing unmet health-related social needs (e.g., transportation, rental assistance, and other needs); (4) patients face challenges understanding how to use clinician-prescribed technologies for remote monitoring that can be resolved with CHW coaching and instruction.
Conclusions:
CHWs reported specific ways they were able to assist patients with clinical, social, and clinician-prescribed health-related technology in HF. Partnerships with CHWs are well positioned to add important value to HF home management for clinical care plan adherence and engagement, remote monitoring, and technology use.
Keywords
Introduction
Heart failure (HF) is one of the most common and costly etiologies of hospital readmissions and acute healthcare costs.1-3 Costs associated with clinician-led interventions4-6 and studies demonstrating the impact of unmet health-related social needs (e.g., transportation, food, housing, finances, and employment stability) on HF outcomes,7-9 have shifted focus to include 2 different approaches: the use of technology with remote monitoring (e.g., digital platforms, wearable devices for biometric monitoring via digital blood pressure monitors and body weight scales )10-12 for improved clinical control and home-based navigators or community health workers (CHWs) to address social needs care.13-15 Despite the promising impact and potential synergy of these 2 approaches as a combined intervention,16-19 few clinical trials or qualitative studies have focused on CHW perspectives on home HF management and remote monitoring via digital platforms, devices, or other forms of technology. Deeper understanding of these perspectives can not only help inform the home management of HF but may also demonstrate important areas where home-based navigation can improve clinical outcomes for clinically and socially complex populations.
Few studies have examined the CHW experience in caring for patients with chronic disease. CHWs, receive training in core competencies of motivational interviewing, healthcare coaching, and psychosocial support. 20 As such, CHWs enhance clinical care plan adherence (e.g., taking medications, blood pressure), address unmet health-related social needs (e.g., transport, food insecurity), improve connections to clinical care teams, and reduce readmissions in chronic disease populations like HF.16-18 A number of qualitative studies have described the challenges of managing HF with home-based care staff.21-23 However, a majority of these studies focus on agency-deployed home care workers (e.g., aids, medical assistants), 21 social workers, 24 or nurses. 25 Some qualitative studies focused on CHW perspectives have been performed with respect to CHW educational or training in local or global settings.26,27 Rarely have studies explored CHW perspectives on the challenges to managing HF at home and how CHW skillsets improve care in terms of clinical care plans, social and psychosocial support, and engagement with technology. Incorporating these domains into the design of HF interventions can answer important questions HF management at home. Specifically, understanding CHW role within the context of the use of digital platforms and other healthcare-focused technology can help inform what technology-inclusive training and support is needed to improve clinical outcomes for patients managing HF at home.
In order to address these knowledge gaps and better understand how home-based care from staff in a CHW role can contribute to HF care in an increasingly technology driven era, we performed qualitative interviews to capture the CHW experience. Interview domains included: social and cultural barriers and facilitators to managing HF care at home; the application of CHW core competencies in HF; remote monitoring and technology in HF; and CHW ability to assist with remote monitoring and technology in HF.
Methods
Setting and Study Design
We conducted three 1.5-hour focus groups with CHWs (December 2020 to February 2021) who had a history of working with adult patients with HF. All participants were employed by a single healthcare institution within the department of community health. Due to the shared professional setting, overlapping focus on clinically and socially complex patient care for a spectrum of comorbidities, and the small size of individual focus groups (n = 5, n = 5, n = 4), additional characteristic comparisons between individual CHWs and focus groups that might lead to identification were not assessed beyond what is listed in Table 1. CHW study participants listed within an internal hospital navigator network database were contacted for study participation. All participating CHWs were affiliated with an 1100-bed academic medical center serving more than 7500 patients with a diagnosis of HF per year. The center employs approximately 60 CHWs, and half provide care to general medical populations that include patients with HF. To be eligible for the study, CHWs had to have a history of caring for adult patients with HF in outpatient settings and be employed by the academic medical center.
Participant Characteristics.

Participant Recruitment
CHWs were identified by an internal hospital network database for navigators. CHWs were emailed an informational letter introducing them to the study with the permission of associated departmental leadership. CHWs interested in participating were enrolled and scheduled for a focus group by sending a calendar invitation with a virtual meeting hyperlink. Eligible CHWs were offered $50 renumeration for participation if the focus group occurred outside of normal workday hours. Participants were emailed a maximum of 3 times if no response to the initial request was received. Before each focus group, participants were asked to confirm that they had a history of caring for patients with HF in their CHW role.
Interview Protocol and Measures
The protocol and interview guide were developed with input from CHWs, CHW supervisors, HF specialists, qualitative research experts, and primary care physicians. This was coupled with a review of the literature of HF including studies focused on patient surveys, CHW experience, and consultations with experts in survey and health services research. The qualitative interview guide was based on key domains to standardize the experience across different focus groups. The interview guide was initially pre-tested in pilot interviews with 2 CHWs and no additional changes were made. The final interview guide included 18 items associated with the following domains: social and cultural facilitators and barriers to patient HF care, CHW impact on home-based care among patients with heart disease, and facilitators and barriers to the use of technology among patients with HF.
Focus groups were conducted by a faculty research team member (JC) and a research coordinator assisted with audio control and notetaking. All procedures were approved by the hospital institutional review board on August 10, 2020. All participants provided verbal informed consent prior to participation.
Analysis
Framework analysis was used to identify major themes. Coding and analysis from verbatim transcription was performed. All transcripts were uploaded in Dedoose (software version 8.3.47B, Los Angeles, CA, March 5, 2021). The analytic framework was developed based on main domains of the patient interview guide. In order to foster reliability, 2 coders (NS and JC) familiar with the transcript data independently identified major themes raised by participants and then utilized this framework to categorize themes and identify patterns and relationships. Associations between themes were then identified. This iterative process was repeated until all transcripts were analyzed. Coding session occurred during weekly meetings with discussion of emerging themes in alignment with the corresponding codes. Any discrepancies were discussed with a third researcher (KD) with specific expertise in qualitative data analysis. This use of investigator triangulation with different researchers examining the data was deployed to enhance validity and credibility of the findings. Ultimately, the research team determined that data saturation was achieved and no additional codes were identified outside of the analytic framework. These methods were consistent with COREQ checklist standards. 28
In addition to focus group participation, all CHW participants completed a semi-structured questionnaire capturing baseline characteristics including demographic information, activities and interactions with patients, as well as general practice and involvement with clinical team members. All responses were captured in REDCap.
The research team used the qualitative interview guide to standardize questions asked of participants. Probing questions were asked for any unanticipated answers in order to accurately capture the participant’s perspective. All coding decisions were tracked. The generated themes were collected from CHWs with experience caring for patients with HF at an urban academic center and may apply to others settings with similar characteristics. The small number of participants in each focus group facilitated in-depth and authentic discussions reflective of the CHW experience. Although the use of multiple focus groups conducted with the interview guide demonstrated significant overlap suggestive of replication, the research effort was focused on gathering perspectives that would add to the evidence-base for HF care in this domain.
Results
Fourteen CHWs completed focus groups. Table 1 shows the demographics and characteristics of the study participants. A total of 34 CHWs were initially contacted by email. Three CHWs declined and 17 CHWs were unable to be reached after 3 emails.
Analysis of the qualitative coding for the focus groups produced 4 emergent themes that are described below and in Table 2.
Major Themes Associated with Illustrative Quotes.
Theme 1 (Barriers and Facilitators): CHWs Noted That Patients Have Difficulty Following Clinical Care Plans at Home (i.e., Medication Adherence, Diet, Fluid Intake)
A common theme that emerged in the CHW focus groups was the difficulty patients experienced carrying out prescribed HF home care instructions. This was often expressed as a difficulty both understanding and connecting the components of their care. One participant offered, “Understanding how the connection between that shortness of breath and maybe getting a little extra Lasix is not certain.” Another participant said, “Patients are told to take medications but are less likely to be taught why.” With regard to appointments and diet, 1 CHW emphasized, “Patients don’t know why they need follow up or what heart healthy food is.”
Theme 2 (Assistance with Clinical Care Plans): CHWs Can Help Re-emphasize Clinical Care Plans for Home Management
One of the most common support modalities participants referenced was connecting patients to clinical care teams, and providing reminders and encouragement. A CHW stated, “I’m kind of the bridge between the patient and the clinical team, you know, that’s kind of how our role comes into play. Because usually I find that once we build that relationship with patients, they will call me even if it’s something small.” One participant offered that “I think it’s very, it’s helpful to give, or sort of, remind them to the way that the doctor wants to do things. Sort of, be that person to ask, have you been following this?”
CHWs also emphasized the important boundaries of their roles. One participant underlined “I’m not a cardiologist, right? I have a basic understanding but I’m not going to be the one making any decisions.”
Theme 3 (Assistance with Unmet Needs): CHWs Support Patient with Unmet Health-Related Social Needs That Contribute to Gaps in Clinical Care
CHWs underscored that some patients do not have the financial means required for transportation, food, or housing which can impact clinical care plan adherence. With regard to follow-up appointments, 1 CHW said, “People hold off of the cardiac appointment until getting the transportation they need in place.” For food insecure patients, 1 CHW said “CHWs are checking that the food items on the shelf and the what is in the food pantry sits on the healthy side.” Another CHW commented, “I’ve had so many patients and if you don’t have stable housing, how can you really be focused on getting to appointments. I mean, where will you even be at that time?”
Theme 4 (Use of Technology): HF Patients Face Challenges in Understanding How to Use Clinician-Prescribed Technologies for Remote Monitoring That Can Be Resolved with CHW Coaching and Instruction
CHWs agreed that many patients with HF have clinical care plans that include devices or digital platforms for monitoring their HF, and often, in their CHW role, they have provided technical assistance. One CHW mentioned, “They are told to do something or to monitor a device that way or this way quickly in clinic. And it looks like they did not process this instruction when they get home.” CHWs offered that the increased use of technology has contributed to CHWs getting more familiarity with cardiac devices. One CHW shared, “We sort of have to know, that’s why I think we are pretty good, my colleagues and I, in following the device instructions.”
CHWs also emphasized that, even with detailed instructions, some patients can get confused about how to use the technology. One CHW said, “Even putting on a Zio patch and mailing it back may not be easy for them.” Another point CHWs made was that many times clinical teams assume that patient are technology-savvy just because they have an email address.
Discussion
This qualitative study underlines key themes from CHWs caring for patients with HF with respect to home-based care and remote monitoring. CHWs reported specific ways they were able to assist patients with clinical, social and clinician-prescribed technology or device needs.
The study expands upon earlier research centered on HF care and highlights specific aspects of home-based support for clinical, social, and technology-focused care. A number of expected findings were seen. In general, CHWs stated that patients were challenged when adhering to care plans at home which is supported by other studies where patients with HF were surveyed.18,29,30 CHWs also detailed how clinical and unmet health-related social needs can be addressed by CHWs. While this has not been well explored in CHW studies, qualitative studies featuring the experiences of social workers and health care workers caring for patients with HF underline the impact of home-based care team outreach.25,31 In this study, CHWs also emphasized the importance of CHW core competencies (e.g., motivational interviewing, connections to care teams, and psychosocial support) in enhancing support for adherence to clinical care plans and connecting patients to needed resources.
Unexpected findings included that CHWs were accustomed to familiarizing themselves with a number of devices, digital platforms, and technologies prescribed by HF clinical teams. This support included familiarizing themselves with the device instructions prior to orienting patients. This underscores the need for technology-focused training and resources as a part of the CHW role.32,33 While the importance of mobile and wireless connectivity is a well-established component of the CHW mHealth movement in global settings,34-37 CHW training on common digital platforms or patient portals used in specific conditions like HF may provide additional value.
CHWs also emphasized that patient barriers to technology are sometimes unknown to the clinical team prescribing the technology-based device or platform. This reflects a disconnect with regard to the assumptions of clinical teams about patient access to resources required for technology or device use as well as patient capacity and familiarity with those resources.38-41 While CHWs were supportive of technology and cited its potential to improve HF home care, CHWs also recognized the need for better understanding of the patient experience on the part of clinical teams. In general, CHWs accentuated the need for tighter clinical team partnership when initiating devices or technology for clinical care. These results are underlined by the fact the comprehensive adoption and integration of emerging technologies like digital platforms for remote monitoring remains challenging. Key drivers for this include the following: logistical and resource-related barriers faced by institutions, limited clinician bandwidth for integration and monitoring; and reduced infrastructure for electronic health record integration of remote monitoring data. 42 Regardless, care for populations unfamiliar with digital and device-associated healthcare solutions or with restricted internet connectivity and other essential access to healthcare remains a concern.43-45 Pairing digital care with navigator or CHW trained home care can enhance adoption while improving both clinical outcomes (e.g., hospital readmissions, emergency department visits, missed clinic appointments)13,18-19 and important population health metrics (e.g., medication adherence, patient perceived quality of life). Additional large-scale clinical trials powered to test the impact of digitally-enabled CHW care and inform innovative care models for HF populations that can benefit most.
Our findings are novel and we were unable to find other qualitative studies focused on this area of care. These findings are suggestive of key opportunities for integration of CHW skillsets addressing gaps in clinical, social, and technology-inclusive care for patients with HF. Specifically, these findings also magnify ways technology-focused barriers can impact patient care and require both (1) better assessment of patient capabilities and engagement prior to implementing clinical care plans inclusive of technology and (2) heightened co-partnership with CHW or home-based care support to anticipate use and engagement (particularly if internet access, email use, weblinks or other specific device interaction is required). Furthermore, these findings better define how the CHW role can enhance fundamental aspects of HF care. Additional clinical trials exploring CHW mechanisms of support in HF are required to better assess patient demographic, clinical, and social factors best aligned for CHW social needs care.
Limitations
This study has a number of limitations. Given the small sample size, the generalizability of these findings is restricted. While we believe that the richness of the responses obtained from CHWs with a history of caring for HF patients provides addition depth and context to managing HF at home, we recognize that these responses were gathered from a single setting within a purposively selected sample and may not be consistent with findings in other institutions, regions, or chronic disease populations. Additional trials are needed from larger and more heterogenous samples to enhance the validity and generalizability of these findings. In addition, the structure and design of clinical care teams as well as resources available for care delivery like CHWs may differ in other settings. Despite this, our use of an interview guide designed by a diverse and multidisciplinary group of clinical and research experts helped identify useful themes that can drive useful practice change in a range of settings. These interviews also occurred during the COVID-19 pandemic which may have created sampling bias with certain CHWs being more available for participation while working remotely from home while others who were deployed and providing patient care may not have had the opportunity to participate.
Conclusion
CHWs caring for patients with HF reported that CHWs support adherence to clinical care plans, connect patients to key resources for social support, and assist in orienting, teaching, and developing solutions for patients facing barriers to technology prescribed by clinical care team. Further research is needed to understand how support from a CHW in combination with remote monitoring could impact clinical outcomes. These findings may be helpful for HF and primary care teams involved in management of HF in outpatient settings.
Footnotes
Acknowledgements
The authors thank MGH Department of Medicine, the Division of General Internal Medicine and the study unit medicine staff.
Ethical Considerations
Ethical approval for this study was obtained from the Partners Human Research Board, approval ID# 2017A050810.
Consent to Participate
All participants provided verbal informed consent prior to study participation.
Consent for Publication
Consent was obtained.
Author Contributions
All authors contributed to the manuscript conception and design. JC wrote the initial manuscript and performed the analysis. AT and KD completed extensive revisions. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Institutes of Health, National Heart, Lung, and Blood Institute (NHLBI): [1K23HL150287-01] awarded to JC. AT was also supported by NHLBI grant K24 HL163073. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Any data requests will be reviewed and carefully considered after publication.