
Abstract
Background:
Chronic obstructive pulmonary disease (COPD) is increasing in prevalence in our aging population in the United States, contributing to morbidity and mortality. Chronic obstructive pulmonary disease and osteoporosis have significant overlapping pathogenic risk factors, including smoke exposure, a chronic inflammatory state, poor nutritional status, immobility, and chronic steroid exposure. This study determines the use of DEXA screening, the prevalence of fragility fractures, and prescription and the use of antiresorptive medications for treatment of osteoporosis and osteopenia in patients with COPD.
Methods:
A retrospective chart review of patients at our health sciences center, including both clinics and hospital, was performed based on ICD-10 codes for COPD, chronic steroid use, and chronic oxygen support in the Cerner database from 2019 to 2023. Exclusion criteria included preexisting or alternative primary lung disease and/or cancer or if further chart review excluded them for not having severe COPD (FEV1 <50%) or not requiring oxygen therapy.
Results:
One hundred seventy-one patients of the original 203 enrolled patients qualified for further analysis after thorough review of charts for confounding diagnosis, lack of oxygen therapy, or lack of formal COPD diagnosis. Forty-one (24%) were screened for osteopenia/osteoporosis using DEXA screening. Of those, 18 (43%) had osteopenia, and 18 (43%) had osteoporosis. Of the 171 eligible patients enrolled in the analysis, 59 (35%) had a fragility fracture. Patients on both inhaled and oral systemic steroids had the highest fracture rate (39%). Overall, 14% (24/171) of patients received treatment for osteopenia/osteoporosis using antiresorptive medications. Treatment rates varied among those receiving steroids versus those who did not. Of the screened group, only 8/18 (44%) patients with osteopenia and 7/18 (39%) patients with osteoporosis received treatment.
Conclusion:
This study demonstrates the patients with severe COPD, based on oxygen requirements and/or the use of corticosteroids, do not have adequate screening for osteopenia and/or osteoporosis. This screening could lead to antiresorptive drug treatment and reduce the morbidity and mortality associated with osteoporotic and osteopenia fractures.
Introduction
Osteoporosis has become more prevalent with the aging of the American population, posing a substantial health concern. Fragility fractures not only increase morbidity and mortality but also substantially diminish the overall quality of life. Despite the medical advances in the detection and treatment of osteoporosis globally, the implementation of comprehensive screening and treatment measures remains limited. 3 Current guidelines from the USPSTF outline screening recommendations for women over 65 years, or those under 65 years with significant risk factors, that is, menopausal status, low body weight, parental history of hip fracture, cigarette smoking, and excess alcohol consumption. 10 This article provides evidence which suggests expansion of these criteria to include patients with severe oxygen dependent COPD with chronic steroid use. The American College of Rheumatology recommends initial clinical fracture risk assessment including DEXA scan within 6 months of initiation of long-term glucocorticoid treatment and treatment based on risk assessment. 13
One group that shares a significant overlap with osteoporotic patients are those patients with chronic obstructive pulmonary disorder (COPD). Recent research indicates that the frequency of osteoporosis in COPD patients is 2- to- 5 times higher than in age-matched healthy adults. 1 This increased risk is attributed to common risk factors such as smoking, reduced physical activity, low weight, sarcopenia, systemic inflammation, and the use of glucocorticoids. 1 Notably, individuals with severe COPD (FEV1 <50%) have an increased risk for lower skeletal mass index and fragility fractures compared to both healthy controls and those with less severe COPD (GOLD 1 or 2). 2 A meta-analysis of 66 papers on bone density established a robust correlation between cumulative bone density loss and oral corticosteroid use. 6
This study reports the screening rates for osteopenia and/or osteoporosis in high-risk patients in our health sciences center, specifically those with COPD currently on corticosteroid therapy, either inhaled or systemic, and assesses how these rates correlate with the disease burden, that is, fragility fractures. Balasubramanian et al 5 investigated 400 000 patients on systemic corticosteroids for multiple systemic inflammatory conditions and found that the fragility fracture rate increased with increasing cumulative doses of corticosteroids, that is, a dose response. These authors found that fracture rates increased to an incidence ratio of 17% (95% CI: 15.0-19.5) in elderly patients with cumulative doses of >5400 mg. In addition, Van Staa et al 6 investigated inhaled corticosteroids such as fluticasone and budesonide in a randomized control trials (RCTs) and observational studies. Their study found a significantly increased risk of fracture in both the RCT and the observational studies, OR of 1.27 (95% CI: 1.01-1.58) and 1.21 (95% CI: 1.12-1.32), respectively. By reviewing the use of screening measures in these vulnerable patients, our study aims to increase awareness of osteoporosis-related complications in severe COPD patients.
Second, this report will determine the use of direct active bone-strengthening drugs in patients identified to have osteoporosis by DEXA screening. Bisphosphonates such as alendronate have been proven to reduce the rate of fragility fractures in all risk categories. Amiche et al 7 reported that the prophylactic prescription of bone protective therapy was only 13% in patients on long-term oral corticosteroids. In these patients, in both men and women, there was a significant decrease in fragility fracture rates following anti-resorptive therapy. This provided substantial evidence of the benefits of prophylactic oral bisphosphonates to prevent future morbidity associated with long-term corticosteroid use. However, the results discussed in this manuscript demonstrate a substantial care gap and illustrate the need to expand our use of these anti-resorptive medications.
Methods
This retrospective chart review calculates screening rates for osteopenia and osteoporosis and treatment rates in high-risk elderly patients with severe COPD requiring oxygen supplementation and concomitant corticosteroid use. Patients of both genders were selected from the TTUHSC/UMC Cerner database between January 1, 2019, and April 27, 2023, and were identified based on the International Classification of Diseases (ICD), 10th version; required diagnosis codes included: COPD, unspecified, long-term current use of inhaled and/or systemic corticosteroids, and oxygen use. The study was approved by institutional IRB (#L23-140).
Exclusion criteria included pulmonary hypertension, chronic pulmonary embolism, pulmonary fibrosis, unspecified, and interstitial pulmonary disease, unspecified.
After patients were identified, data collection from medical records was done with systematic chart review and data extraction. Information including demographics, FEV1 percent predicted (GOLD criteria), oral corticosteroid use and dose, inhaled corticosteroid use, supplemental oxygen use, smoking status, BMI, other high-risk medications, DEXA performed, date of DEXA, DEXA result (T-score), site of worst DEXA (femur and spine), fracture status, site of fracture, date of fracture, treatment for osteoporosis, and vital status. The FEV1 percent predicted was converted into its corresponding GOLD category (I-IV), and if patients did not meet the GOLD criteria of 3 or 4 (FEV <50% or lower) or have pulmonary function testing, they were removed from study consideration. DEXA scans were reviewed to find the site of the worst T-score, and the site and T-score values were recorded. Groups were compared using Chi square and t tests; multivariable testing was not used.
Medication use was assessed by reviewing patient medication reconciliations; if the patient was taking oral corticosteroids for more than 3 months that would classify him/her as oral corticosteroid use positive. This duration of 3 months was selected to isolate patients with long term steroid use rather than pulse dose treatment for acute exacerbations. The same criteria were used for inhaled corticosteroid use. Treatment medications were noted the same way, so that if the patient received bisphosphonates, estradiol, raloxifene, teriparatide, zoledronic acid, and denosumab at all in their electronic medical records (EMR), irrespective of single-use or continuous still counted as providing treatment. Assessing for fractures including reviewing the radiology, hospital admission, and EMR search for fractures, subsequently classified as fragility fractures based on being vertebral compression or pelvic, forearm, or trochanteric fractures resulting from more traumatic instances including falling from a standing or sitting height.
Chi square testing was used to compare frequency of osteopenia and osteoporosis in various treatment groups in Table 1, the number of fractures in various treatment groups in Table 2, and the frequency of antiresorptive medications for the various treatment groups in Table 3.
DEXA Screening Rates and T-Scores Among Those Screened.

There is no difference in DEXA screening between patients in the osteopenia category and the osteoporosis category based on Chi square testing. P ≥ .05.
Fracture Incidence in Screened and Non-screened Groups.
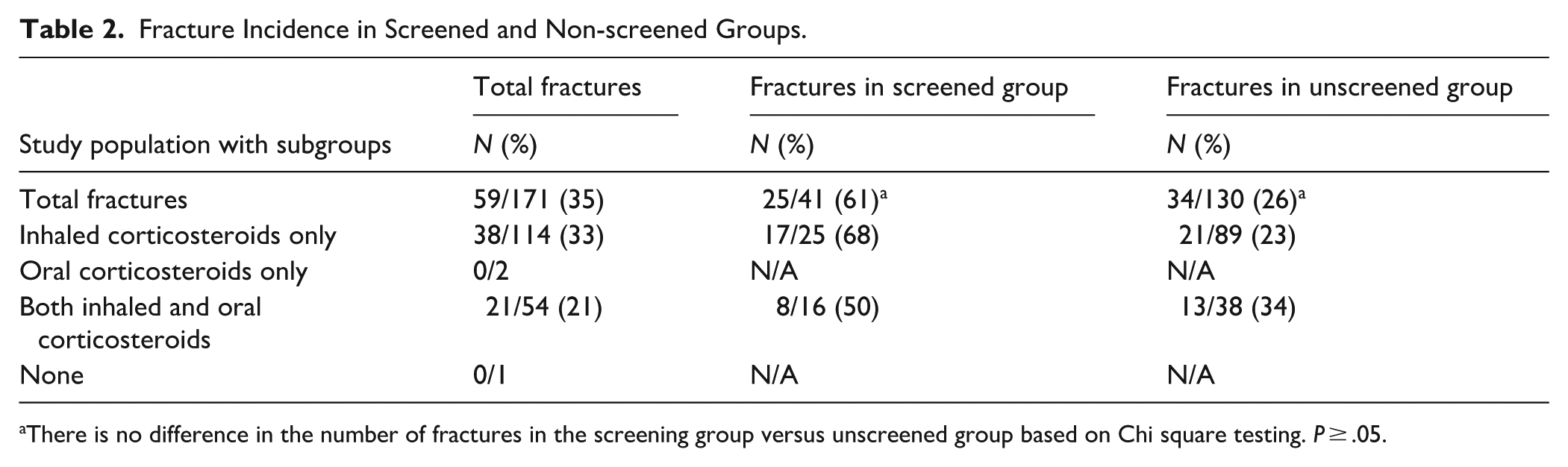
There is no difference in the number of fractures in the screening group versus unscreened group based on Chi square testing. P ≥ .05.
Rates of Treatment in Patients With BMD Scores Within Osteopenia or Osteoporosis.
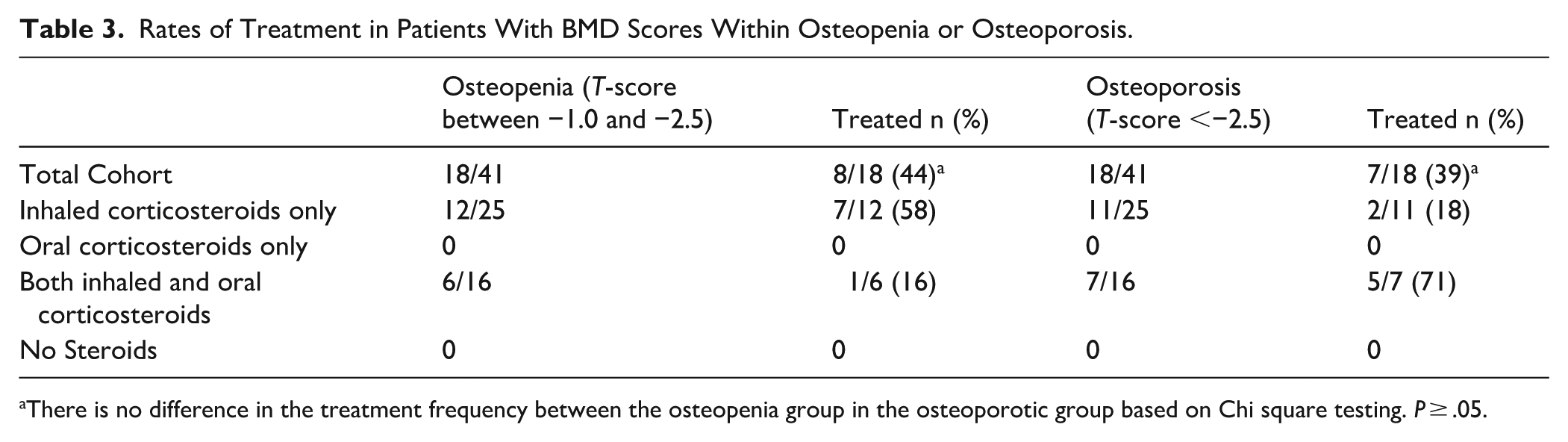
There is no difference in the treatment frequency between the osteopenia group in the osteoporotic group based on Chi square testing. P ≥ .05.
Results
Two hundred three patients were initially identified for this study; 22 patients were excluded for not having COPD based on a pulmonary function test (or having a confounding diagnosis), and 10 were excluded for not requiring oxygen supplementation based on their chart reviews. This selection of eligible patients is reflected in the attached consort diagram (Figure 1). Of the remaining 171 patients, 41 (24%) were screened for osteopenia and/or osteoporosis. of those 41 screened with DEXA scanning, 36 had a T-score of −1 or less (88%), of whom 18 had a T-score of −2.5 or less (44%). Screening rates based on steroid exposure and respective T-scores are provided in Table 1.
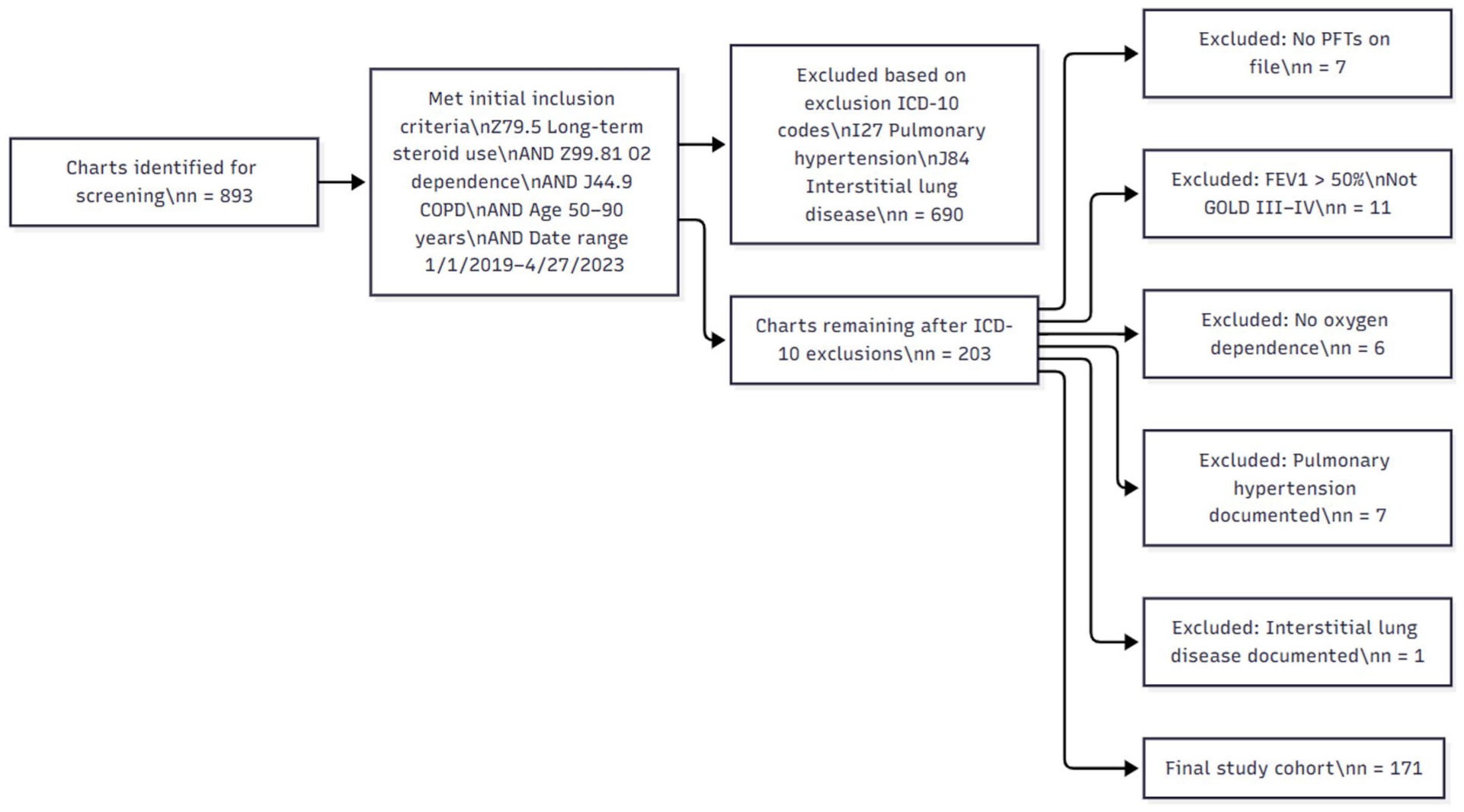
Consort diagram: patient selection criteria.
Of the 171 eligible patients enrolled in the analysis, 59 (35%) had a fragility fracture. Patients on both inhaled and systemic corticosteroids had the highest fracture rate, 21 of 54 (39%). Compared with those on only inhaled steroids, 38 of 114 (33%) had a fracture. Among the 41 patients screened, 25 (61%) had fragility fractures (Table 2).
Overall, 24 of 171 (14%) of patients received treatment for either osteopenia or osteoporosis using anti-resorptive medications (bisphosphonates; Supplemental Table 4,). No other anti-resorptive or anabolic medications were documented in our study cohort. Among the 41 patients screened with DEXA, 15 (36%) received treatment for osteopenia or osteoporosis. Among the 18 patients with osteopenia (T-score between −1.0 to −2.5), 8 received treatment. For the 18 patients with osteoporosis (T-score <−2.5), 7 received treatment (39%). Table 3 reports these results.
Discussion
The overall DEXA screening rate for these high-risk patients was 24%. Using the T-scores from these DEXA results; In this group, 43% had osteopenia, and 43% had osteoporosis. The patients with the highest screening rate included those on both inhaled and oral systemic corticosteroids, who were screened at a rate of 30% (16/54). Results showed 12% (2/16) had osteopenia and 43% (7/16) had osteoporosis.
The overall fracture rate in this high-risk population was 35% (59/171). The group with the highest fracture rate included those on both inhaled and systemic corticosteroids; 21 of the 54 patients (39%) had a fragility fracture compared to the group only on inhaled corticosteroids which had a fracture rate of 33% (38/114).
The overall treatment rate using anti-resorptive medications was 14%. The treatment rate was highest in the group on both systemic and inhaled corticosteroids at 17%. The treatment rate was lowest in the group that was on only inhaled corticosteroids; only 15 of 114 patients were treated, a rate of 13%. This, however, is not selective for patients with low BMD, but rather those who were a part of the whole group of high-risk individuals, FEV <50% predicted, oxygen dependent COPD patients (Supplemental Table 4).
The treatment rate of patients with osteopenia (screened patients with T-scores of −1 or less) in this study was 44%, and the treatment rate of osteoporotic patients (screened patients with a T-score of −2.5 or less) was 39%. The reasons for this difference are not clear. No information about FRAX score, medication intolerance or affordability was available during chart review. The highest treatment rate in osteoporotic patients was in patients on both inhaled and systemic corticosteroids at a rate of 71%. The lowest rate of treatment for osteoporotic patients was for those only on inhaled corticosteroids, who had a treatment rate of 18%, with only 2 of 11 patients receiving treatment.
The prevalence of osteoporosis and low BMD in the United States for people 50 or older is estimated to be 10.35% and 43.9% respectively, as calculated by the US Centers for Disease Control and Prevention (CDC).4,8 A retrospective review of 1.6 million Medicare Advantage enrollees found that the BMD screening rates using DEXA among women from 2008 to 2014 was 21.2%, 26.5%, and 12.8% in women aged 50 to 64, 65 to 79, and 80+ respectively. 9 These rates are similar to those found in our study, which had an overall screening rate of 23.9%, irrespective of age and gender. Since our study evaluated both men and women, it is important to recognize that the inclusion of males drastically alters the screening rates. Although the screening rate for this group is higher than the national average, it remains inadequate given the high risk of complications and morbidity. The United States Preventive Services Task Force (USPSTF) cites a number of fair-quality trials, totaling 57 000 participants, determining the reduction in hip fractures provided by screening for low BMD and found a hazard ratio of 0.72. 10 This means the screened group had a 28% lower risk of hip fractures than the non-screened group. This is the basis for a B rating provided by the USPSTF and underlines the necessity of early detection and treatment.
With regards to steroid-associated fragility fractures, 1 study that followed 1.9 million patients through the National Health Checkup program showed that over 6 months of daily high-dose systemic corticosteroids led to 2.43 times higher risk of vertebral fractures and 3.28 times higher rates of hip fractures. 11 This supports the findings in this report, in which the fracture rate among individuals, both men and women, on oral systemic corticosteroids was remarkably high at 38%. The age adjusted incidence of fragility fractures for patients within this sample age group is 7.3% when not accounting for steroid use. 15 This corresponds to a fivefold increase in incidence of fragility fractures within our sample. The same associated bone density risk has not been as universally accepted and studied for those on chronic inhaled corticosteroids. Several studies investigating the use of inhaled corticosteroids for COPD and asthma treatment have not provided congruent statistically significant findings of increased fracture risk or bone mineral density changes, with some studies showing increased risk and some finding no difference. 12 One retrospective cohort study found a statistically significant increased risk in vertebral compression fractures for those on inhaled corticosteroids, compared to a control group with a relative risk of 1.51 (95% CI: 1.22-1.85). 6 In our study, the fragility fracture rate was 33% in patients using inhaled corticosteroids and 39% in those using both inhaled and systemic, a difference of 6%. The high level of fractures in all groups within this high-risk population suggests that exposure to steroids only compounds he risk.
For our patients with identified osteoporosis or previous fragility fracture, prescription of anti-resorptive medications is low at 18% (2/11). When comparing these findings to other similar studies, 1 study found that within a group of high-risk individuals taking long-term oral corticosteroids, 9.8% underwent BMD measurement and 14.5% received anti-resorptive treatment. Our study found relatively higher screening rates (30%) but similar anti-resorptive prescription rates (17%). 14 One final point to mention is the nuance in deciding to treat patients with anti-resorptive mediations. Many factors influence this decision between the patient and provider, ones that are difficult to parse out in the medical record. These factors include: life expectancy, age, comorbidities, mobility, motivation/willingness, and financial resources.
Limitations
This study has several important limitations. These include correct ICD10 coding and the date range of our study. As a result, we may not have identified all patients in our healthcare system who would qualify for the study. It was a requirement that they were seen by a provider within the time period in order to be selected, so patients with poor follow-up were likely excluded. We were unable to tell if the patient had DEXA scanned elsewhere, as DEXA use was reviewed solely using chart review, not a national database. As for the low use of DEXA, it is typical that if patients have a negative DEXA they are not re-screened, which may contribute to the low use within our time frame. This study was also limited to patients who had pulmonary function tests that corroborated the COPD treatment regimen or ICD10 code. Ultimately, as with all retrospective chart reviews, patients may have received medication, been screened, or experienced fractures, all of which were not documented in our electronic medical records if they were seen elsewhere. Specific clinicians’ role in medical decision making, lack of documentation about medication related side effects or unaffordability limit the conclusions further.
Conclusion
Glucocorticoids are often used in the treatment of severe COPD and provide substantial symptom relief and decrease the length of hospital stay. However, the benefits of these medications are tempered by the risk and known damaging effects on bone health. This study found that in the subset of high-risk patients, the screening rates for osteoporosis are low with an overall rate of 24% being screened. Although this is higher than the average in the United States, screening should be much higher in these patients, considering that the disease risk is much greater.
The clearest indication of under-recognition is the mismatch between screening rates and the prevalence of fragility fractures. In our center’s study cohort of 171, 41 (24%) were screened, while 59 (35%) experienced a fragility fracture. This under-recognition is particularly evident among patients treated with inhaled corticosteroids alone, suggesting that clinicians may prioritize screening in the setting of systemic steroid exposure while overlooking other important contributors to fracture risk, including age, chronic inflammation, hypoxia, smoking, low body mass index, physical inactivity, and inhaled steroids. It is apparent that for most of these patients, COPD management is at the center of their medical care with the use of corticosteroids and oxygen therapy, and pulmonary follow-up and overlook critical factors such the possibility of a low bone mineral density and the devastating impact of fragility fractures. As fractures significantly increase morbidity and mortality in this population, addressing bone health must become an integral part of COPD care to improve long-term outcomes.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319261429678 – Supplemental material for Underutilization of Osteoporosis Screening in Patients With Severe COPD and Long Term Corticosteroid Use
Supplemental material, sj-docx-1-jpc-10.1177_21501319261429678 for Underutilization of Osteoporosis Screening in Patients With Severe COPD and Long Term Corticosteroid Use by Alistair Disraeli, Kenneth Nugent and Neha Mittal in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
Gilbert Berdine, MD contributed toward peer review and modification of the manuscript.
Ethical Considerations
This study was approved by institutional IRB # L23-140.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Retrospective chart review.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.