
Abstract
Objective:
Using State-level surveillance records we assessed disparities in premature mortality among people with HIV (PWH) in Florida during pre- (2019) and early COVID-19 pandemic (2020).
Methods:
We calculated age-standardized rates of years of potential life lost per 100 persons (aYPLL) stratified by sex, race and ethnicity, rural/urban residence, and social vulnerability index (SVI).
Results:
PWH in Florida during 2020 experienced a significant increase in aYPLL (2019: 29.0, 95% CI [28.1, 30.0]; 2020: 32.8, 95% CI [31.8, 33.9]). HIV/AIDS contributed the most aYPLL in 2020 (13.4, 95% CI [12.4, 14.4]), especially among females (15.8, 95% CI [15.2, 16.4]), rural communities (14.5, 95% CI [12.7, 17.6]), and high SVI communities (12.5, 95% CI [11.9, 13.2]). aYPLL due to external causes increased significantly from 2019 to 2020 (4.1, 95% CI [4.0, 4.3] vs 5.4, 95% CI [5.2, 5.5]), especially for females (3.6, 95% CI [3.3, 3.9] vs 7.8, 95% CI [7.4, 8.3]) and those living in low SVI communities (3.1, 95% CI [2.7, 3.8] vs 7.1, 95% CI [6.5, 8.1]). aYPLL due to COVID-19 was greatest for females (2.3, 95% CI [2.1, 2.6]) and residents of high SVI communities (2.0, 95% CI [1.9, 2.1]).
Conclusions:
PWH experienced increased individual- and neighborhood-level disparities in premature mortality from HIV/AIDS from 2019 to 2020, especially among females and those in rural and socially vulnerable communities. External causes and COVID-19 were also associated with an increased premature mortality during this time frame, with disparities noted by sex and community social vulnerability. Pandemic planning should include targeted outreach programs which prepare for vulnerable populations’ healthcare needs and mitigate mortality.
Introduction
The United States (US) experienced the largest reduction in life expectancy in 2020 due to COVID-19 pandemic conditions which disproportionately affected minority populations.1,2 Hispanic/Latino, Non-Hispanic Black, American Indian/Alaskan Native, and Native Hawaiian/Pacific Islanders faced significantly higher mortality risks than Non-Hispanic Whites.1,3 Additionally, minority and economically disadvantaged communities suffered greater mortality than non-disadvantaged communities.4,5 These differences are partly attributable to systemic inequities which have left these communities vulnerable to pandemic stress.3,6 People with HIV (PWH), who are disproportionately represented within the intersections of these groups, face compounding disadvantage and premature death which few studies have addressed.7-9
Results from limited studies which compare change in mortality trends among PWH prior to and during the pandemic indicate that PWH likely experienced increased mortality in 2020 compared to pre-pandemic years (2018-2019).8-10 However, these studies do not characterize the severity of the early COVID-19 pandemic’s impact on premature mortality. By employing years of potential life lost (YPLL), a measure that calculates the expected number of years a person would have lived had they not experienced a fatal event, we may better illustrate premature mortality from unnecessary and avoidable deaths among PWH. 11
We aim to compare premature mortality among PWH in Florida during the early stages (2020) of the COVID-19 pandemic to premature mortality before the pandemic (2019) employing YPLL prior to availability of vaccines and pharmaceuticals which improved survivability. Additionally, we examine variations in cause-specific mortality across sex, race and ethnicity, rural/urban residence, and neighborhood social vulnerability to characterize disparities and inform future policy-making and pandemic planning which prepare for the healthcare needs of PWH.
Methods
De-identified records for Florida residents alive and diagnosed with HIV as of December 31, 2018, were obtained from the Florida Department of Health (DOH) enhanced HIV/AIDS Reporting System (eHARS). This includes data from Florida DOH Vital Records linked with the Social Security Administration’s Death Master File and the National Death Index (merged June 2021). Variables included date of HIV diagnosis and death (if applicable), age in 2019, age in 2020, sex, race and ethnicity, HIV transmission mode, ZIP Code and State of residence (2018-2020 and at death, if applicable), place of birth, and underlying cause of death (if applicable).
Underlying causes of death were classified using the International Classification of Diseases, Tenth Revision (ICD-10) codes from the primary cause of death and categorized as follows: (1) deaths attributable to HIV/AIDS (B20-B24); (2) COVID-19 (U07-U12); (3) cardiovascular disease (CVD; I00-I99); (4) diabetes (E10-E14.9); (5) cancer (C00-16, C18-C22, C25, C32-C34, C43, C46, C50, C53-C56, C61, C64-C67, C70-C72, C81-C96); (6) external causes (S09-S09.9, T01-T71, U01-U03, V01-Y09, Y85.0-Y87.1); (7) liver disease (K70-K77); (8) renal failure (N17-N19); (9) respiratory disease (J00-J47); (10) other causes (all other codes); and (11) unknown causes (no code). 12 These specific categories were chosen based on previous research indicating that the COVID-19 pandemic exacerbated pre-existing conditions contributing to premature mortality.
Neighborhood social vulnerability was assessed by replicating methodology developed by the CDC for the 2020 Social Vulnerability Index (SVI) to rank ZIP Code Tabulation Areas (ZCTA) in Florida based on 4 vulnerability themes. 13 The 4 themes include socioeconomic status, housing composition, minority status/language, and housing type/transportation. Each theme was scored individually and then summed to provide a total score. This score was then ranked on a scale of 0 to 100 to obtain an overall SVI score, where higher values denote higher levels of vulnerability. These combined SVI scores were then categorized into tertials of low, medium, and high SVI. Variables needed to calculate SVI were obtained from the 2020 5-year American Community Survey (ACS) at the ZCTA level, which approximates ZIP Codes by aggregating US Census block data based on postal addresses. ZIP Code-level designations of rurality were obtained from the Health Resources and Service Administration (HRSA) Federal Office of Rural Health Policy, which uses the US Census Bureau’s rural-urban classification (UA/UC), Rural-Urban Commuting Area (RUCA) codes, and Office of Management and Budget definition (OMB) to determine rural designation. 14 ZIP Code level data were merged with individual level eHARS data using the persons’ most recent ZIP Code of residence either at death or at years end (2019 and 2020). For each analysis, if the residence at years end was missing, the previous year’s residence was carried forward. Individuals with unknown ZIP Codes of residence either at years end for the current or previous year, or at death were excluded from the analysis. Additionally, individuals whose ZIP Code level data could not be calculated due to invalid ZIP Code data or missing social vulnerability score for any of the themes were also excluded.
Methods previously described by Trepka et al. (2015) were used to calculate YPLL, which is the expected number of years of life a person is estimated to achieve, given their current age and sex. 15 Using a uniform cut off for all individuals would lead to an undercounting of YPLL for older individuals and therefore lead to biased estimates in YPLL. 15 Thus sex-specific US life tables for the year 2020, which account for differences in life expectancy by sex, were used to estimate the number of years individuals would have lived if they had not experienced premature death. 16 Age-standardized rates of premature mortality, both for all causes and specific causes of death, were calculated as age-standardized years of potential life lost per 100 persons (aYPLL) using direct standardization with the 2000 US standard population, and stratified by sex, race and ethnic group, rural/urban residence, and neighborhood social vulnerability (SVI). Factor phi was used in calculating the 95% confidence intervals (CIs) to address overdispersion of the gamma distribution. Rates were considered statistically significant if CIs did not overlap. All analyses were conducted using SAS 9.4 (Cary, NC).
Ethical Considerations
This cross-sectional retrospective study was approved by the Florida Department of Health (2021-491) and Florida International University (IRB-21-0256-AM03) Institutional Review Boards. As the data received was deidentified, the study was exempt from informed consent.
Results
A total of 117 174 and 118 572 individuals were reported living with HIV in Florida as of December 31, 2018 and December 31, 2019, respectively, of whom 114 700 (2019) and 113 757 (2020) met inclusion criteria. Excluded individuals consisted of those with missing or invalid Florida ZIP Code residence at year’s end or at death (2019: 2373; 2020: 4792). Additionally, individuals older than 89 years of age (2019: 101; 2020: 113) were excluded from the analysis due to the high likelihood of unreported death not captured by the surveillance system as most (90%) had no evidence of viral suppression in the 4-years prior to 2020. Across both years, most PWH in Florida were 40 to 59 years (2019: 54.5% for females and 50.8% for males; 2020: 53.8% for females and 49.2%, for males), male (2019: 72.8%; 2020: 73.3%), and US born (2019: 73.3% for females and 71.5% for males; 2020: 72.5% for females and 70.7% for males). Most people resided in urban communities (>95% for females and males) and lived in high SVI communities (2019: 75.2% for females and 65.7% for males; 2020: 74.7% and 65.6%, respectively; Table 1 and 2).
Characteristics of Florida Residents With HIV by Sex and Race/Ethnicity in 2019 (N = 114 700).

Abbreviations: AIDS, acquired immunodeficiency syndrome; HIV, human immunodeficiency virus; IDU, injection drug use; MSM, men who have sex with men.
P-value for all variables < .0001.
Characteristics of Florida residents with HIV by sex and race/ethnicity in 2020 (N=113,757).

Abbreviations: AIDS, acquired immunodeficiency syndrome; HIV, human immunodeficiency virus; IDU, injection drug use; MSM, men who have sex with men.
P-value for all variables < .0001.
Age-standardized years of potential life lost per 100 persons (aYPLL) due to all-causes of death in 2020 was 32.8 years compared to 29.0 years in 2019. Females had significantly higher aYPLL than males in 2020, but not in 2019 (2020: 41.5 vs 27.5 years, respectively; 2019: 31.3 vs 30.1 years; Table 3 and 4). There was no significant difference in aYPLL among rural residents compared to urban residents for either year. PWH living in low or medium SVI communities experienced a significant increase in all-cause aYPLL from 2019 to 2020 (low SVI: 26.2 vs 22.1 years, respectively; medium SVI: 27.2 vs 22.7 years, respectively). However, PWH living in high SVI communities sustained significantly higher aYPLL compared to those living in low or medium SVI communities across both years (32.2 both years; Table 5). The contributors to this increase in premature mortality for 2020 were HIV/AIDS, COVID-19, external causes of death, and cardiovascular diseases (CVD). Cancer, diabetes, renal, liver, respiratory diseases excluding COVID-19, other, and unknown underlying causes of death did not significantly increase aYPLL among PWH between 2019 and 2020 (Table 3 and 4).
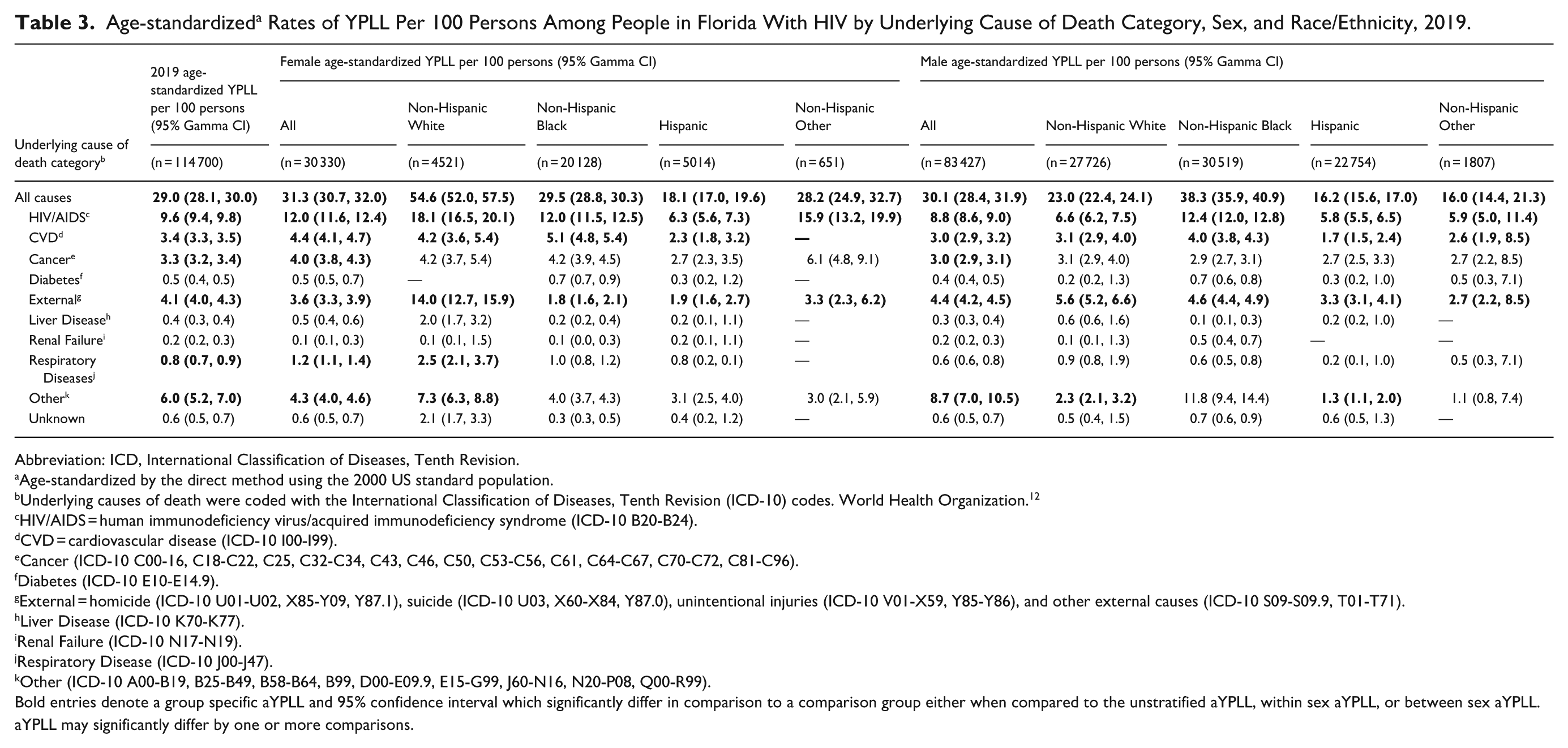
Age-standardized a Rates of YPLL Per 100 Persons Among People in Florida With HIV by Underlying Cause of Death Category, Sex, and Race/Ethnicity, 2019.
Abbreviation: ICD, International Classification of Diseases, Tenth Revision.
Age-standardized by the direct method using the 2000 US standard population.
Underlying causes of death were coded with the International Classification of Diseases, Tenth Revision (ICD-10) codes. World Health Organization. 12
HIV/AIDS = human immunodeficiency virus/acquired immunodeficiency syndrome (ICD-10 B20-B24).
CVD = cardiovascular disease (ICD-10 I00-I99).
Cancer (ICD-10 C00-16, C18-C22, C25, C32-C34, C43, C46, C50, C53-C56, C61, C64-C67, C70-C72, C81-C96).
Diabetes (ICD-10 E10-E14.9).
External = homicide (ICD-10 U01-U02, X85-Y09, Y87.1), suicide (ICD-10 U03, X60-X84, Y87.0), unintentional injuries (ICD-10 V01-X59, Y85-Y86), and other external causes (ICD-10 S09-S09.9, T01-T71).
Liver Disease (ICD-10 K70-K77).
Renal Failure (ICD-10 N17-N19).
Respiratory Disease (ICD-10 J00-J47).
Other (ICD-10 A00-B19, B25-B49, B58-B64, B99, D00-E09.9, E15-G99, J60-N16, N20-P08, Q00-R99).
Bold entries denote a group specific aYPLL and 95% confidence interval which significantly differ in comparison to a comparison group either when compared to the unstratified aYPLL, within sex aYPLL, or between sex aYPLL. aYPLL may significantly differ by one or more comparisons.
Age-standardized a Rates of YPLL per 100 Persons Among People in Florida With HIV by Underlying Cause of Death Category, Sex, and Race/Ethnicity, 2020.

Abbreviations: ICD, International Classification of Diseases, Tenth Revision.
Age-standardized by the direct method using the 2000 US standard population.
Underlying causes of death were coded with the International Classification of Diseases, Tenth Revision (ICD-10) codes. World Health Organization. 12
HIV/AIDS = human immunodeficiency virus/acquired immunodeficiency syndrome (ICD-10 B20-B24).
CVD = cardiovascular disease (ICD-10 I00-I99).
Cancer (ICD-10 C00-16, C18-C22, C25, C32-C34, C43, C46, C50, C53-C56, C61, C64-C67, C70-C72, C81-C96).
Diabetes (ICD-10 E10-E14.9).
External = Homicide (ICD-10 U01-U02, X85-Y09, Y87.1), suicide (ICD-10 U03, X60-X84, Y87.0), unintentional injuries (ICD-10 V01-X59, Y85-Y86), and other external causes (ICD-10 S09-S09.9, T01-T71).
Liver Disease (ICD-10 K70-K77).
Renal Failure (ICD-10 N17-N19).
Respiratory only (ICD-10 J00-J47).
COVID-19 (ICD-10 U07-U12).
Other (ICD-10 A00-B19, B25-B49, B58-B64, B99, D00-E09.9, E15-G99, J60-N16, N20-P08, Q00-R99).
Bold entries denote a group specific aYPLL and 95% confidence interval which significantly differ in comparison to a comparison group either when compared to the unstratified aYPLL, within sex aYPLL, or between sex aYPLL. aYPLL may significantly differ by one or more comparisons.
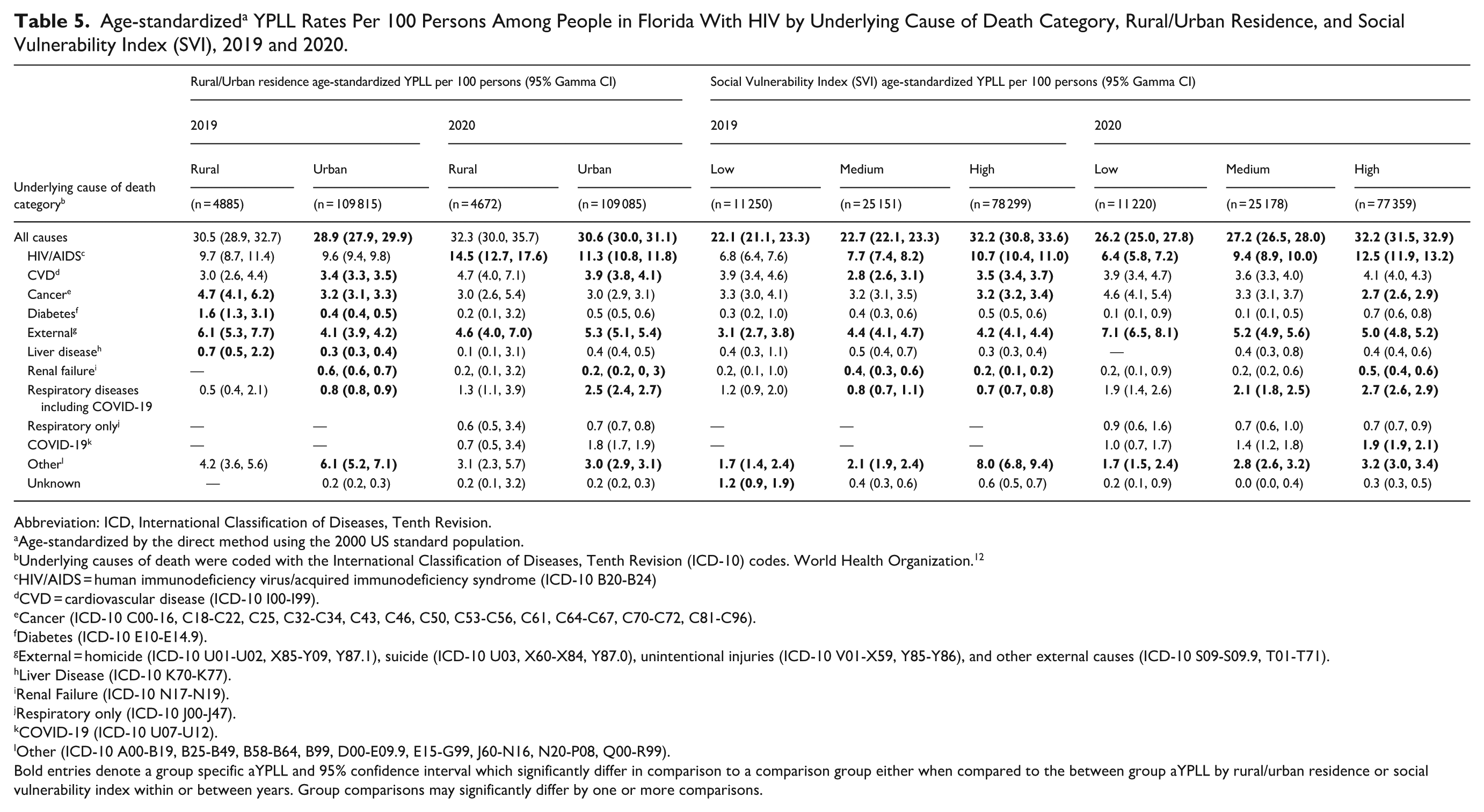
Age-standardized a YPLL Rates Per 100 Persons Among People in Florida With HIV by Underlying Cause of Death Category, Rural/Urban Residence, and Social Vulnerability Index (SVI), 2019 and 2020.
Abbreviation: ICD, International Classification of Diseases, Tenth Revision.
Age-standardized by the direct method using the 2000 US standard population.
Underlying causes of death were coded with the International Classification of Diseases, Tenth Revision (ICD-10) codes. World Health Organization. 12
HIV/AIDS = human immunodeficiency virus/acquired immunodeficiency syndrome (ICD-10 B20-B24)
CVD = cardiovascular disease (ICD-10 I00-I99).
Cancer (ICD-10 C00-16, C18-C22, C25, C32-C34, C43, C46, C50, C53-C56, C61, C64-C67, C70-C72, C81-C96).
Diabetes (ICD-10 E10-E14.9).
External = homicide (ICD-10 U01-U02, X85-Y09, Y87.1), suicide (ICD-10 U03, X60-X84, Y87.0), unintentional injuries (ICD-10 V01-X59, Y85-Y86), and other external causes (ICD-10 S09-S09.9, T01-T71).
Liver Disease (ICD-10 K70-K77).
Renal Failure (ICD-10 N17-N19).
Respiratory only (ICD-10 J00-J47).
COVID-19 (ICD-10 U07-U12).
Other (ICD-10 A00-B19, B25-B49, B58-B64, B99, D00-E09.9, E15-G99, J60-N16, N20-P08, Q00-R99).
Bold entries denote a group specific aYPLL and 95% confidence interval which significantly differ in comparison to a comparison group either when compared to the between group aYPLL by rural/urban residence or social vulnerability index within or between years. Group comparisons may significantly differ by one or more comparisons.
HIV/AIDS was the largest contributor to aYPLL for both females and males across all race and ethnic classifications in both years (2020: 15.8 vs 10.3 years, respectively; 2019: 12.0 vs 8.8 years, respectively; Table 3 and 4). In 2020, Non-Hispanic Other (NHO) females had 9-times the aYPLL of their male counterparts (48.3 vs 5.3 years) and the highest aYPLL among female PWH. This was also nearly double the aYPLL identified in 2019 (28.2 years). Non-Hispanic White (NHW) females sustained more than double the aYPLL due to HIV/AIDS of their male counterparts (18.1 vs 6.8 years). NHB females and males had similar aYPLL in 2019 (12.0 vs 12.4 years), but in 2020, NHB females had significantly higher aYPLL due to HIV/AIDS compared to their male counterparts (16.8 vs 11.5 years). Lastly, Hispanic females in 2020 experienced the fewest aYPLL (3.8 years) due to HIV/AIDS compared to all sex and race and ethnic groups. They also experienced less than half the aYPLL experienced by their male counterparts whose aYPLL significantly increased from 5.8 years in 2019 to 17.0 years in 2020; a reversal of the relationship seen in 2019 (Table 3 and 4). Both rural and urban residents experienced increases in aYPLL due to HIV/AIDS during 2020. However, while there was no difference in the aYPLL between rural and urban residents during 2019, in 2020 rural residents experienced significantly higher aYPLL compared to urban residents (14.5 vs 11.3 years). When comparing social vulnerability in both 2019 and 2020, aYPLL due to HIV/AIDS increased as social vulnerability increased. PWH living in medium and high SVI communities experienced a significant increase from 2019 to 2020 while those living in low SVI communities did not (high: 10.7 vs 12.5 years; medium: 7.7 vs 9.4 years; low: 6.8 vs 6.4 years; Table 5).
Premature mortality across all PWH significantly increased from external causes of death between 2019 and 2020 (4.1 vs 5.4 years, respectively). Female PWH experienced more than double the aYPLL during 2020 compared to 2019 (7.8 vs 4.1 years), while PWH males didn’t experience a significant increase between years (2019: 4.4 years; 2020: 4.7 years; Table 3 and 4). In 2020, NHW females sustained significantly higher aYPLL due to external causes of death than their male counterparts (15.1 vs 7.5 years) and the highest aYPLL across all sex, race, and ethnic groups. While all racial and ethnic minority females experienced increased aYPLL in 2020 compared to 2019 (NHB: 4.5 vs 1.8 years, respectively; Hispanic: 14.8 vs 1.9 years; NHO: 8.1 vs 3.3 years), only Hispanic females experienced significantly more aYPLL due to external causes of death compared to their male counterpart in 2020 (Hispanic males: 2.3 years); a reversal of the relationship seen in 2019 (Table 3 and 4). While external causes of death didn’t significantly increase aYPLL for rural (2019: 6.1 years; 2020: 4.6 years) or urban inhabitants (2019: 4.1 years; 2020: 5.3 years) between years, urban inhabitants experienced more aYPLL compared to rural inhabitants in 2020, another reversal of the previous year’s relationship. When comparing community social vulnerability, aYPLL due to external causes of death increased as SVI scores decreased (low: 7.1 years; medium: 5.2 years; high: 5.0 years; Table 5).
While premature mortality due to respiratory diseases excluding COVID-19 did not increase between 2019 and 2020, the added burden of COVID-19 increased aYPLL across all PWH between 2019 and 2020 (respiratory diseases including COVID-19: 0.8 years in 2019 vs 2.4 years in 2020; Table 3 and 4). Females experienced more aYPLL due to COVID-19 than their male counterparts (2.3 vs 1.5 years). However, there were no significant racial and ethnic differences in aYPLL by sex (Table 4). Similarly, there were also no significant differences in aYPLL by rural/urban residence. Conversely, as social vulnerability increased, so too did aYPLL due to COVID-19 (low: 1.0 years; medium: 1.4 years; high 1.9 years). PWH living in high SVI communities had significantly higher aYPLL due to COVID-19 compared to those living in low or medium SVI communities (Table 5).
Finally, PWH experienced a smaller but significant increase in mortality from CVD between 2019 and 2020 (3.4 vs 4.0 years, respectively). While female PWH experienced significantly higher aYPLL in both years compared to their male counterparts (females 2019: 4.4 years vs males: 3.0 years; females 2020: 4.8 years vs males: 3.8 years), only male PWH experienced a significant increase in aYPLL between years (Table 3 and 4). Only NHW females experienced significantly more aYPLL compared to their male counterparts (5.2 vs 3.0 years) in 2020. While NHB females had significantly higher aYPLL due to CVD in 2019 compared to their male counterparts (5.1 vs 4.0), this did not persist in 2020 (Table 3 and 4). Urban inhabitants experienced significantly greater aYPLL in 2020 (3.9 years) compared to 2019 (3.4 years). Lastly, in 2020 there were no significant differences in premature mortality by community social vulnerability, despite PWH residing in high SVI communities experiencing more aYPLL from CVD in 2019 compared to PWH residing in medium SVI communities (3.5 vs 2.8 years, respectively; Table 5).
Discussion
We had 4 notable findings. First, PWH in the early pandemic (2020) experienced significantly more YPLL than pre-pandemic (2019), largely due to HIV/AIDS and external causes of disease as opposed to COVID-19. Second, females had a greater burden of YPLL than males, especially NHW females. Third, high neighborhood social vulnerability was associated with increased YPLL due to all-causes, HIV/AIDS, and COVID-19. Lastly, residents of rural communities suffered greater YPLL in 2020, driven by increased premature mortality from HIV/AIDS.
PWH in Florida experienced nearly 4 additional years of life lost per 100 persons in 2020 than in 2019 attributable to increases in premature mortality from HIV/AIDS, external causes of death, COVID-19, and CVD. HIV/AIDS was the largest contributor to premature mortality across most sex, race, and ethnic groups. However, among Hispanic females, external causes, which include suicide and accidental overdose, accounted for the most aYPLL (Supplemental Figure 1). The limited contribution of COVID-19 to greater mortality could be attributed to antiretroviral therapy, which reduced immunosuppression, and increased vigilance to COVID-19 prevention, such as quarantine, masking, and social distancing among PWH.17,18 One study which assessed compliance with COVID-19 prevention strategies found that some Black MSM in Atlanta modified their behaviors during the early pandemic to prevent possible exposures to COVID-19. 17 However, further research is warranted to understand compliance with health messaging among PWH during outbreaks and epidemics.
Female PWH living in Florida have a lower proportion of viral suppression which may explain sex-differences in premature mortality (Table 1 and 2). Furthermore, while premature mortality has improved since 2009, all-cause premature mortality for both NHW and NHO females was significantly higher than their peers. 15 A greater percentage of NHW females had intravenous drug use (IDU) as the recorded HIV acquisition mode (Tables 1 and 2). Post-hoc analysis revealed that intentional and unintentional poisonings accounted for most of the deaths (Supplemental Figure 2) and IDU transmission accounted for the highest aYPLL (35.8 years) among NHW females (Supplemental Table 1). A recent study which compared pre-pandemic mortality by HIV acquisition mode found that women who likely acquired HIV through IDU experienced greater mortality. 19 Further research is required to understand the current shift in premature mortality rates seen in NHW females. We also note that NHO females also appeared to have increased rates of YPLL; however, due to small numbers, caution is warranted when interpreting results for this group (Supplemental Table 2). When we investigated this category further, we noted that deaths mostly occurred among individuals who identified as multiracial. Increased negative health outcomes may be attributable to racism and discrimination due to social perception of skin tone—perceived darker skin tones have been associated with discrimination, poor mental health outcomes, and stress.3,20 Although the limitations of our data prevent identifying definitive reasons for premature mortality in this group, clinicians and policymakers should still consider that these communities may experience disproportionate health risks and vulnerabilities. This underscores the importance of mixed-methods and community-based participatory research approaches for understanding the mechanisms that may drive mortality disparities in difficult-to-measure populations.
Higher social vulnerability accounted for increased premature mortality for all-causes and specific conditions of death such as HIV/AIDS and COVID-19. Most PWH in Florida live in highly vulnerable communities (Table 1 and 2). Disadvantaged communities often suffer from fewer protective factors such as community and healthcare resources, political power, and beneficial social networks, which drive health inequities. 15 Increased presence of structural and systematic community inequities negatively impacts individual health, especially in minority communities. 3 Additionally, while our findings did not suggest significant premature all-cause or COVID-19 mortality between urban and rural residents, YPLL due to HIV premature mortality remains higher for rural residents. Limited resources, transportation, and increased stigma may play a role in accessing care, especially for HIV, in rural communities. 21 Telemedicine has been an essential tool for making healthcare more accessible and convenient during the pandemic.22,23 However, there remain significant barriers for rural communities due to limited broadband and device accessibility. 3 Programs which provided video capable devices to participants saw promising results in patient satisfaction and healthcare utilization and retention. 24 Continued effort to make HIV care accessible is important in reducing the disparities in HIV mortality for residents of rural and disadvantaged communities.
Our study findings are limited by the analyses and data sources employed. We were unable to control for adherence to ART and viral suppression, which may impact likelihood of mortality, due to the nature of our descriptive analysis. Additionally, premature mortality due to any specific cause of disease is subject to competing causes or misclassification of death. Similarly, we didn’t assess the extent to which contributing causes of death, including COVID-19, contributed to premature mortality from the primary underlying cause of death. While we could not control for these factors within our analysis, we included a comparison of all-cause premature mortality to elucidate differences in sex, racial, ethnic, and community characteristics across all possible causes of death. Finally, we were unable to include some records in our analysis due to missing/incomplete information such as those experiencing incarceration or housing instability. While it is likely that these populations suffered worse outcomes, their unique circumstances would be best suited for studies which do not attempt to generalize the mortality experience for PWH.
Conclusion
Disparities in premature mortality across sex, race and ethnic groups, and community disadvantage persist for PWH. Demographic- and community- specific factors should be considered in pandemic response planning to reduce disparities in burden of premature mortality, especially for females and vulnerable communities.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319261422872 – Supplemental material for Comparison of Premature Cause-Specific Mortality Among People With HIV in Florida Pre-(2019) and Early (2020) COVID-19 Pandemic: Disparities by Race and Ethnicity, Sex, Rurality, and Social Vulnerability
Supplemental material, sj-docx-1-jpc-10.1177_21501319261422872 for Comparison of Premature Cause-Specific Mortality Among People With HIV in Florida Pre-(2019) and Early (2020) COVID-19 Pandemic: Disparities by Race and Ethnicity, Sex, Rurality, and Social Vulnerability by Giselle A. Barreto, Tan Li, Tendai Gwanzura, Diana M. Sheehan and Mary Jo Trepka in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We are grateful to Colby Cohen and Lorene M. Maddox, HIV/AIDS Section, Florida Department of Health for preparing the de-identified HIV surveillance data. We are also grateful to Joseph Muller, now at the Viral Hepatitis and Outbreak Response Section, Florida Department of Health, for his assistance in the development of this manuscript. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Florida Department of Health. Additional tables and figures may be found online.
Ethical Considerations
Study was approved by the Florida International University (IRB-21-0256-AM03) and Florida Department of Health (2021-491) Institutional Review Boards.
Author Contributions
GAB was responsible for assisting in the conceptualization and project planning, software coding and analysis, resource acquisition and data curation, original draft writing, and visualization. TL was involved in the conceptualization, methodological development, validation, resource acquisition, and manuscript review and editing. DMS was involved in the conceptualization, methodological development, validation, resource acquisition for the project, and manuscript review and editing. TG was involved in the data curation, resource acquisition, software coding development, and manuscript review and editing. MJT provided supervision, conceptualization, methodological development, validation, resource acquisition, and manuscript review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this abstract was supported in part by the National Institute on Minority Health and Health Disparities of the National Institutes of Health under Award Number U54MD012393. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or National Institute on Minority Health and Health Disparities.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.