
Abstract
Introduction:
Primary care clinics often undertake quality improvement (QI) projects to enhance care delivery. Disruptions to clinical practice, such as staffing changes, can hinder QI efforts. Limited research examines how primary care clinics experience and respond to disruptions. This study explores the types and impacts of disruptions and factors linked to resilience for rural clinics during a Human Papillomavirus (HPV) vaccination QI study.
Methods:
We used a mixed-methods, longitudinal design to assess disruption frequency and type alongside clinic-level vaccination outcomes. Qualitative case studies explored how disruptions influenced QI participation and resilience factors.
Results:
Among 41 rural clinics studied, all reported at least 1 disruption during QI implementation, including staffing loss (37 clinics, 90%), EHR implementation (10 clinics, 24%), and organizational changes (4 clinics, 9%). Disruption frequency and type did not differ across quartiles of HPV vaccination improvement. Eight clinics were selected for in-depth case study analysis, which revealed factors shaping resilience: (1) clinic characteristics, (2) practice facilitator support, and (3) disruption characteristics.
Conclusion:
Disruption type or number did not explain differences in vaccination improvement. Multiple factors were found to influence resilience and continued QI. Identifying and enhancing these facilitators is critical to supporting primary care clinics through inevitable challenges.
Keywords
Background
Primary care clinics take on quality improvement (QI) projects to enhance patient experience, improve population health outcomes, reduce cost, and ensure provider wellbeing. 1 Significant variation exists among clinics’ experience and structure surrounding QI efforts. This may vary from no formal experience or structure to dedicated improvement teams tasked with improving specific metrics. 2 Studies have shown that many barriers exist to making and sustaining QI changes,3-5 and primary care clinics are often under-resourced to support this work. Rural clinics in particular experience more barriers to making and sustaining QI changes. 6
Disruptions can pose a significant challenge for clinics participating in QI, including unexpected events like natural disasters, or chronic challenges like financial strain. 7 Common primary care disruptions include staff turnover, implementing a new electronic heath record (EHR), and organizational changes like merging with another health system.8-11 These disruptions can negatively affect clinical care as well as QI. 9 Understanding resilience—how health systems adapt and transform to recover from disruptions—is critical to ensuring long-term participation in QI, but little research describes the impact and response to disruptions among primary care clinics. 12
The Rural Adolescent Vaccine Enterprise (RAVE) study utilized a practice facilitator led QI intervention during a period of extreme healthcare disruption, the COVID-19 pandemic (2020-2022), making RAVE an ideal setting to explore the impact of a variety of disruptions on QI. This manuscript aims to describe clinic disruptions experienced during RAVE, demonstrate the impacts of disruptions on QI efforts, and describe factors associated with resilience.
Methods
We used a mixed-methods, longitudinal design to examine disruption frequency and type alongside clinic-level HPV vaccination improvement. Qualitative collective case studies explored how disruptions influenced QI and identified factors that mitigated their impact on RAVE QI efforts. 13 Oregon Health & Science University’s Institutional Review Board (IRB# 18660) approved all study activities.
Study Setting
RAVE was conducted through the Oregon Health & Science University. 14 Eligible clinics were located in rural areas (defined by Oregon Office of Rural Health as any geographic area in Oregon that is 10 or more miles from a population center of > 40,000 people), participated in the Vaccines for Children program, and had at least 20 adolescents aged 13 to 17 and 10 aged 11 to 12. From April 2019 to March 2021, participating clinics received 18 months of practice facilitation to improve HPV vaccination. Support included monthly meetings with a facilitator and QI-based strategies to enhance HPV vaccination rates. 15
Data Collection and Variables
This analysis drew from 3 primary data sources: (1) clinic-reported data, (2) the ALERT Immunization Information System (IIS), and (3) practice facilitator fieldnotes.
Descriptive Analysis
Descriptive statistics were used to summarize clinic characteristics, changes in HPV vaccine completion rates, and types of disruptions experienced. Disruptions are reported by quartile of HPV vaccine improvement. Due to small sample sizes per quartile and frequent overlap in disruption types, no between-group statistical analyses were conducted. Stratified data are presented to illustrate observed trends only.
Case Study Analysis
Case study clinics were selected using a maximum-variation approach to capture heterogeneity in clinic context, experience, and outcomes. 19 This approach allowed for analytic comparison across contrasting cases to examine how similar factors did or did not manifest across different conditions. Clinics were chosen to reflect diverse disruption experiences: those with unique or infrequent disruptions, high or low disruption frequency, and those facing common disruptions to ensure representativeness. Selection also considered disruption impact on project participation, categorized inductively from facilitator fieldnotes as: continued participation (minimal change), reduced participation (delayed or scaled-back efforts), or halted QI (ended implementation). Clinics with poor data quality were excluded. Case study data were analyzed using latent projective content analysis to explore patterns and nuance in disruption impact. 20 Two qualitative analysts reviewed fieldnotes to identify meaningful units, then abstracted case study data from REDCap into Atlas.ti 23 for auto-coding using an a priori codebook (disruption description, impact, response plans, follow-up). Coded data were then organized into a matrix (by disruption type, response, impact, actor, timing, and outcome) by 1 analyst and reviewed by the second for accuracy. Both analysts reviewed the matrix to group similar cases and identify factors related to clinic resilience via analytical memos. Memos were discussed with the analytic team, project manager, and a RAVE facilitator to develop and refine themes through group consensus over 3 meetings. Final themes were validated with the full study team.
Results
Of the 46 clinics randomized in the RAVE project, 1 was deemed ineligible, leaving 45 participating clinics. Four clinics did not launch RAVE activities and lacked required disruption data, resulting in 41 clinics included in the HPV completion rate quartile analysis. Of the 41 included clinics, 8 were selected as case studies for further exploration. Clinic characteristics are shown in Table 1.
Characteristics of RAVE Clinics.
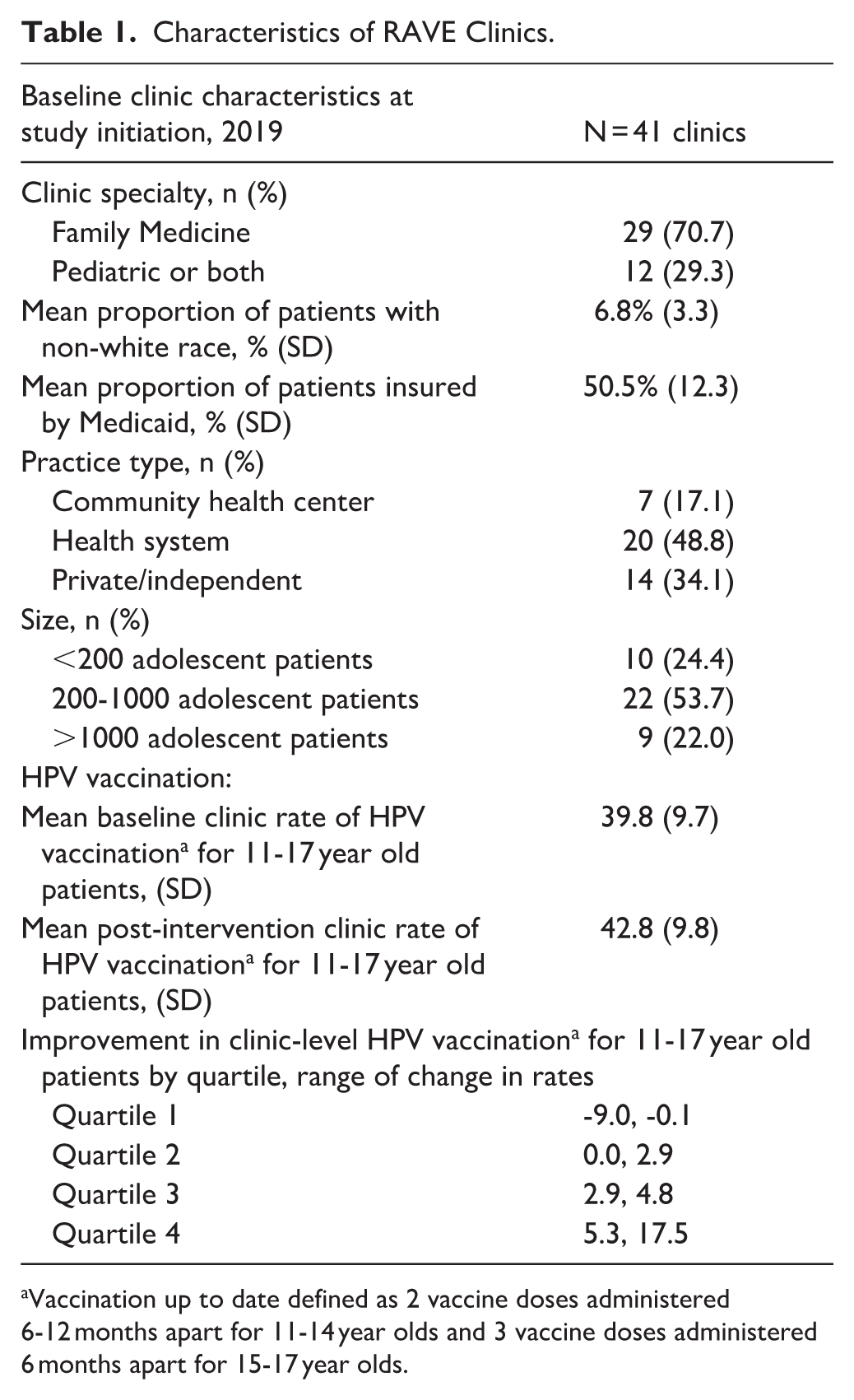
Vaccination up to date defined as 2 vaccine doses administered 6-12 months apart for 11-14 year olds and 3 vaccine doses administered 6 months apart for 15-17 year olds.
Quantitative Findings
HPV vaccination rate changes ranged from a 9 percentage point decrease to a 17.5 point increase. Clinics in the lowest improvement quartile saw changes from −9.0 to −0.1 points, while those in the highest quartile improved by 5.3 to 17.5 points. Disruption characteristics were summarized by HPV rate change quartile (Table 2). All 41 clinics reported at least 1 disruption during RAVE implementation. Staffing loss was most common (37 clinics, 90%), followed by new EHR implementation (10 clinics, 24%) and new organizational structures (4 clinics, 9%). “Other” disruptions, reported by 37 clinics (90%), were mostly related to COVID-19 but also included natural disasters. Disruption frequency and type were similar across quartiles, with no clear pattern linking disruption type or number to HPV rate change.
Summary of Disruptions Experienced, Overall and by HPV Vaccination improvement Quartiles.

Disruptions in the other category mostly included COVID-19 modified operations.
Qualitative Findings
The 8 clinic case studies analyzed qualitatively are summarized in Table 3. Of the 8 case studies, 3 were able to continue with their QI efforts despite disruptions (Case study 25, 1, 3). All 3 of these clinics were also able to improve their HPV completion rates. Three of the case clinics continued QI through disruptions, but at a reduced capacity, either delaying efforts or scaling down to accommodate changes caused by disruptions (Case study 33, 13, 42). Of the 3 clinics that reduced their QI efforts, only 1 was able to improve their HPV completion rates (Case study 33). Finally, 2 clinics had to stop their RAVE QI efforts due to disruptions (Case study 19, 5). Of these 2 clinics, 1 was able to improve their HPV rates (Case study 5), and 1 was not (Case study 19).
Case Study Clinic Summaries and Outcomes.

Cross-case comparison produced with-in case understanding and cross-case pattern identification that led to the identification of 3 categories of factors that impacted resilience from disruptions. These categories included: (1) clinic characteristics; (2) supports from practice facilitators; and (3) disruption characteristics. For most clinics, a combination of factors were present, which had both positive and negative influences on resilience. No one factor stood out as exclusively protective. However, clinic factors that influenced engagement in QI during disruption, namely clinic staff mindset, did appear to often buffer other factors that had a prohibitive influence on continued QI.
Clinic characteristics that influenced engagement in QI during disruptions
Clinic Staffing: Staffing significantly influenced clinic engagement in QI during disruptions. Clinics with sufficient or flexible staffing (i.e., float staff) were better able to adapt and maintain QI when disruptions affected team structure, roles, or staffing levels. For instance, clinic case study 25 experienced major staffing losses across multiple roles during implementation. As a health system-based clinic, they accessed float staff like medical assistants and triage nurses from other departments. This flexibility helped them sustain RAVE implementation and improve HPV completion rates. Alternatively, clinic case study 5 lost staff roles to restructuring, which included QI specific roles. Without QI staff, the clinic halted participation in RAVE QI and ultimately decided to no longer participate.
QI Experience & Structure: Prior QI experience and structure influenced clinic engagement during disruptions. Clinics with limited QI experience or lacking formal structures often struggled to continue implementation. In contrast, those using a team-based approach had greater capacity to share workloads or absorb staff loss. Clinics relying on a single person, like clinic 19 with only 1 engaged provider, often stalled when that person left. Clinics without formal QI teams lost momentum, especially when implementing QI ad hoc and responding to competing demands like COVID-19. Lack of leadership support further hindered efforts; for example, clinic 42 had to justify RAVE participation to unsupportive system leadership. Finally, clinics with an established QI culture—where QI was routine and valued—were better able to sustain efforts during disruption.
Clinic Staff Mindset: Staff mindset played a critical role in QI efforts during disruption. Clinics that embraced change, viewed disruptions as opportunities, and demonstrated determination were more likely to sustain QI. For example, clinic 1, a small clinic with limited resources, implemented RAVE and improved QI rates despite staff loss and COVID-19 by normalizing change and persisting through challenges. Clinic 13, facing reduced visits and staff hours, used the extra time to focus on HPV vaccine initiatives, turning disruption into progress. Similarly, clinics that used creative problem-solving, assessed capacity, and communicated needs were better able to adapt implementation plans. Strong motivation to improve vaccine rates or engage in QI also helped clinics persevere through adversity.
Practice Facilitator Strategies that Moderated Disruptions Effects on QI
Accountability: Practice facilitation supported QI by providing accountability, especially during disruptions. Facilitators helped clinics stay on track with RAVE by adjusting plans to match capacity, reminding teams of action items, and checking on progress. This was especially valuable when disruptions diverted attention from QI. For example, clinic 33 credited their facilitator’s accountability as the key reason they continued implementation during COVID-19.
Adapting Implementation Plans: Practice facilitators helped clinics revise implementation plans during disruptions by assessing needs, revisiting goals, and identifying new, flexible paths forward. This adaptability allowed clinics to continue QI, even at a smaller scale or with a different focus. In some cases, it was key to sustaining RAVE efforts despite challenges. It also gave clinics space to recover without losing momentum, making it easier to resume progress as capacity returned.
Disruption Characteristics that Influenced QI Impact
Anticipated vs. Unexpected Disruptions: The ability to continue QI often depended on whether disruptions were expected. Planned changes (i.e., EHR transitions or staff retirements) allowed clinics to prepare and minimize impact. For example, clinic 3 faced staff loss and an EHR change but maintained RAVE efforts due to proactive planning. In contrast, unanticipated disruptions, such as natural disasters or sudden COVID-19 illnesses, made it harder to sustain QI, as clinics had to balance immediate needs with long-term solutions like hiring, often leading to greater struggle.
Disruption Acuity: The duration and severity of disruptions shaped clinic engagement in QI. Short but severe disruptions often paused implementation but had minimal long-term impact, as clinics resumed QI quickly afterward. In contrast, persistent but less severe disruptions (lasting months) created greater barriers. Some clinics continued QI by leveraging other supports, but others experienced significant delays or cessation. For example, clinic 19 briefly halted RAVE due to a wildfire evacuation but resumed operations within a month. However, ongoing staffing losses afterward ultimately led them to stop implementation and not complete RAVE.
Concurrent Disruptions: Experiencing multiple disruptions simultaneously made it harder for clinics to sustain QI. This was especially challenging when staffing shortages coincided with other issues, like a COVID-19 surge. For example, clinic 33 faced 9 months of reduced staffing while also managing increased sick visits due to COVID-19. The compounding disruptions led the clinic to scale back their RAVE QI efforts.
Discussion
In this study, we found no clear patterns between HPV completion rate quartiles and reported disruptions, suggesting no specific disruption type consistently influenced QI performance. However, qualitative analysis identified several key factors supporting QI continuity during disruptions. The level of anticipation and acuity of disruptions affected clinics’ capacity for change. Case studies highlighted the importance of staffing, QI experience and structure, staff mindset, and the role of practice facilitators in providing accountability and adapting implementation plans. These findings align with prior research showing that disruption type and number did not significantly affect clinics’ capacity for facilitated QI, while internal QI structures, mindset, and facilitator adaptations supported resilience and sustained engagement. 9
Historical research on organizational disruption focused on absorbing change to maintain a steady state. 12 However, disruptions observed in this study—such as the COVID-19 pandemic—support emerging views that emphasize organizational transformation to establish a new operational norm and reduce disruption impact. 7 Our qualitative findings reinforce this, showing that clinic mindset and perception of disruption influenced continued QI. As the healthcare landscape evolves, the nature and impact of disruptions are also shifting, highlighting the need for an adaptive, evolutionary approach to supporting clinic QI.21-24
Disruptions—both anticipated and unanticipated—are inevitable in primary care and are expected to increase due to rising pandemics and natural disasters. 8 Projected healthcare worker shortages may worsen this challenge, especially as this study highlights the importance of sufficient and flexible staffing for sustaining QI during disruptions. 25 These findings align with Thomas et al., who identified key health system functions for clinics facing disruption: (1) governance—strong, participatory leadership; (2) financing—adequate resources; (3) resources—sufficient and well-distributed staff and infrastructure; and (4) service delivery—flexible care models. 26 Future research should examine strategies to help clinics strengthen modifiable factors that support QI resilience.
Limitations
This study has several limitations. First, the small sample of clinics in each quartile limited analyses to observational trends only. In addition, the number of clinics included in the case study favored in-depth analysis of cases over representativeness or enumeration of all available cases. Further, research with a larger sample could provide more nuance into how disruption influences clinic performance. Second, this study was a part of a randomized trial using QI to improve 1 clinical performance outcome. Though our findings are likely relevant to QI for other areas of clinical care, further research is needed to determine if results of this study are the same for a variety of QI projects. Further, the clinics in the study were all located in rural areas of 1 state and may not be representative of the experiences of urban clinics or rural clinics in other regions. Finally, qualitative data collected for this study were collected and recorded systematically, but reflect the point of view of practice facilitators, which is subject to bias based on their role and individual perceptions.
Conclusion
Disruptions are inevitable in primary care, and how clinics respond significantly affects their engagement in improvement activities. Understanding disruptions and identifying intervention opportunities is essential for developing strategies that support consistent, sustainable QI in changing contexts. Since resilience is modifiable, further research is needed to optimize it amid ongoing uncertainty.
Footnotes
Acknowledgements
The authors would like to acknowledge the 45 rural primary care clinics and their staff for their work in this research study and beyond to improve the health of their patients and communities. The authors would also like to acknowledge the ORPRN Practice Facilitators who supported the participating clinics through RAVE implementation.
ORCID iDs
Ethical Considerations
Oregon Health & Science University’s Institutional Review Board (IRB# 18660) approved all study activities.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was funded by the American Cancer Society, RSG-18-022-010.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data used in this study may be made available upon reasonable request pending institutional approvals.