
Abstract
The Screen Dependency Scale (SDS) is a parent-report tool designed to assess screen media dependency in preschool children which was originally developed in Malay within the Malaysian community. This study aimed to translate and validate the English version of the Screen Dependency Scale (SDS) to enable broader participation, particularly in urban areas where English is widely used. Phase 1 involved forward and backward translation by 2 language experts. An addiction specialist reviewed the back-translated version against the original followed by Face Validity by 14 parents. Phase 2 consisted of a cross-sectional study involving 195 parents of children aged 4 to 6 years. Construct validity was tested using exploratory factor analysis (EFA) followed by confirmatory factor analysis (CFA). CFA showed all items had factor loadings of 0.50 or higher. Model fit indices (RMSEA = 0.08; CFI = 0.92) indicated a good fit. The English SDS demonstrated excellent internal consistency (Cronbach’s alpha = .89). Thus, the English version is a valid and reliable tool for assessing screen dependency in Malaysian preschoolers.
Keywords
What We Already Know
Excessive screen time in preschool children is associated with negative cognitive, behavioural, and developmental outcomes.
Screen Dependency Scale (SDS) is a validated parent-report tool originally developed in Malay for assessing screen media dependency in Malaysian preschoolers.
English is widely spoken in Malaysia, especially in urban areas, yet a validated English version of the SDS was previously unavailable.
What This Article Adds?
Provides a rigorously translated and culturally adapted English version of the SDS, validated through expert review, face validity, and pilot testing.
Demonstrates strong psychometric properties of the English SDS, including good model fit (RMSEA = 0.08, CFI = 0.92) and high internal consistency (Cronbach’s α = .89).
Offers a practical and reliable tool for screening screen dependency among English-speaking Malaysian preschool children aged 4 to 6 years.
Introduction
Modern life is closely tied to electronic devices, which have become essential for work, shopping, learning, banking, and entertainment, especially since the COVID-19 era. 1 With improved internet access, device use has surged, even among young children. Parents often rely on screens for education, entertainment, and distraction, making screen use common during meals and family time. 1 While screen media offers many benefits, excessive use can be harmful. Screen time spent on devices like TVs, computers, smartphones, and tablets can negatively affect children if not properly managed. 2 The World Health Organisation (WHO) and American Academy of Paediatrics (AAP) recommend no screen time for children under 2 (except for video calls) and a limit of 1 h per day for those aged 2 to 5 years.3,4 Excessive screen use may lead to behavioural, social, mental, and health issues, and can hinder development. Early childhood, especially the first 3 years is critical for brain development, as the brain is highly responsive to external stimuli. Like substance addiction, excessive screen exposure in this stage may cause neurological and genetic changes, leading to screen dependency, problematic, and prolonged engagement with screen activities.2,3,5-10
While many tools assess screen media addiction in adults and adolescents, few exist for children. A recent narrative review identified 3 tools available for children below 10 years old: the Videogame Addiction Scale for Children (VASC), the Digital Addiction Scale for Children (DASC), and the Problematic Media Use Measure (PMUM). 11 However, the VASC was developed in Turkish and is limited to videogame-specific behaviours, while the DASC, though available in English, targets children aged 9 to 12 years and focusses primarily on digital or gaming addiction. The PMUM is the only parent-report measure designed for younger children (aged 4-11 years) and available in English, but it was developed in a Western context and has yet to be validated among Malaysian preschoolers. 11 These tools differ in conceptual frameworks, target age groups, linguistic suitability, and cultural relevance, and none are specifically tailored for preschool children in Malaysia.
The Screen Dependency Scale (SDS) is a parent-reported tool assessing screen media dependency in preschool children. It was developed in the Malay language and validated in Malaysia. 12 However, given Malaysia’s multicultural context where English is widely used, an English version is necessary. This is to ensure a developmentally appropriate and culturally relevant tool for the early identification of screen dependency among Malaysian preschoolers.
The SDS contains 15 items across 4 domains: preoccupation, behavioural issues, impact on daily activities, and parental perception of screen tolerance. It has shown strong reliability (Cronbach’s alpha = .9) and good model fit (RMSEA = 0.085, CFI = 0.93). 12 The possible lowest score for the SDS is 15 and the maximum is 60, the higher the score indicates higher dependence. 12 The receiver operating characteristic (ROC) curve was used to define the best sensitivity and specificity of a cut-off point in the scores. Meanwhile, the cut-off score for the SDS was determined by using the Youden index. A score of 24.50 was the cut-off score in which the SDS differentiates non-dependence versus dependence on the screen, with a sensitivity of 55% and specificity of 80%. The area under the curve (AUC) was acceptable, which is 0.7. 12 Using tertile percentile analysis, the scores were categorised as: no dependency (<24), mild (24.5-29.0), moderate (29.5-35.0), and severe (35.5-60.0). 13
The SDS was identified as the most suitable instrument for this purpose, and its translation into English facilitates wider application in multicultural populations and global research settings. This study aims to translate and validate the English version of the SDS.12,13
Methodology
Population
This study involved parents or guardians of Malaysian preschoolers aged 4 to 6 from selected registered preschools in Seremban, Negeri Sembilan. Participants were English-literate and had children using screen media. Children with psychiatric conditions (eg, ADHD and autism) or multiple siblings in the same age range were excluded. The study had 2 phases; Phase 1 forward and backward translated the Malay Screen Dependency Scale (SDS) into English by 2 language experts followed by face validation and Phase 2 was a cross-sectional study to assess the validity and reliability of the English SDS (Figure 1). For Phase 2, based on Nunnally’s rule of 10 subjects per item for validation, a minimum of 150 participants was required for the 15-item SDS1. 14 Accounting for a 20% dropout, the target sample size was 180. A total 195 respondents participated in this study.

Study flowchart.
Study Instrument
The study instrument consisted of 2 sections: sociodemographic data and the Screen Dependency Scale (SDS). The sociodemographic section collected details about the parent/guardian-child relationship, the child’s age, gender, ethnicity, parental mediation practices, and environmental factors. This study used the English-translated version of the SDS.
Data Collection Procedure
To minimise selection bias, preschools were selected using computer-generated simple random sampling from the official list provided by the Negeri Sembilan Education Office. Subsequently, all eligible children in these preschools were included through universal sampling, reducing the risk of systematic exclusion. With teachers’ assistance, consent was gathered from respondents before distributing the questionnaire through Google Forms via WhatsApp. Sampling continued until the target sample size was reached.
Data Analysis Procedure
Data was collected via Google Form from June to November 2022 and analysed using IBM SPSS Statistics Version 25.0. Descriptive statistics were used to summarise sociodemographic data (frequency, percentage, mean, and standard deviation). In Phase 1, back translation was compared with the original SDS to ensure content validity. Face validity was assessed by reviewing the translated version for clarity and readability, with adjustments made as needed. Once finalised, construct validity was tested using exploratory factor analysis (EFA) followed by confirmatory factor analysis (CFA) with IBM SPSS AMOS. Reliability was assessed using Cronbach’s alpha to measure internal consistency.
Results
Sociodemographic Data
This study involved 195 respondents, mostly mothers (78.5%), with the majority being Malay (70.3%) and Muslim (70.3%). The average age was 36.1 years, with most having a university education (68.7%) and being employed (80%). All respondents allowed their children to use screen media, mainly to occupy them (32.8%), manage boredom (30.3%), or during meals (22.1%). While most parents monitored content (63.1%) and set limits (57.4%), 20.5% had no rules, and 1.5% never discussed media content.
Among the children, most were aged 4 to 6 years, and had 2 or 3 siblings. None were reported to have autism or ADHD. Most families lived in urban areas (83.1%) and had access to internet (90.8%) and mobile internet (95.4%). Nearly all parents used devices around their children (97.4%), and 19.5% admitted to leaving the TV on without watching.
TVs (81.0%) and smartphones (72.3%) were the most used devices. Activities included video streaming (80.5%), games (51.8%), educational apps (51.8%), and animation (8.2%). On weekdays, 57.4% used screens for over an hour; this rose to 76.4% on weekends. Physical effects of excessive screen use included eye strain, sleep problems, and fatigue (25.6%), with behavioural issues like poor attention (57.9%), tantrums (30.8%), and anger (27.2%; Table 1).
Sociodemographic of Parents/Guardians, Children, Home Environments, and Children Screen Media Usage.

Translation and Face Validation
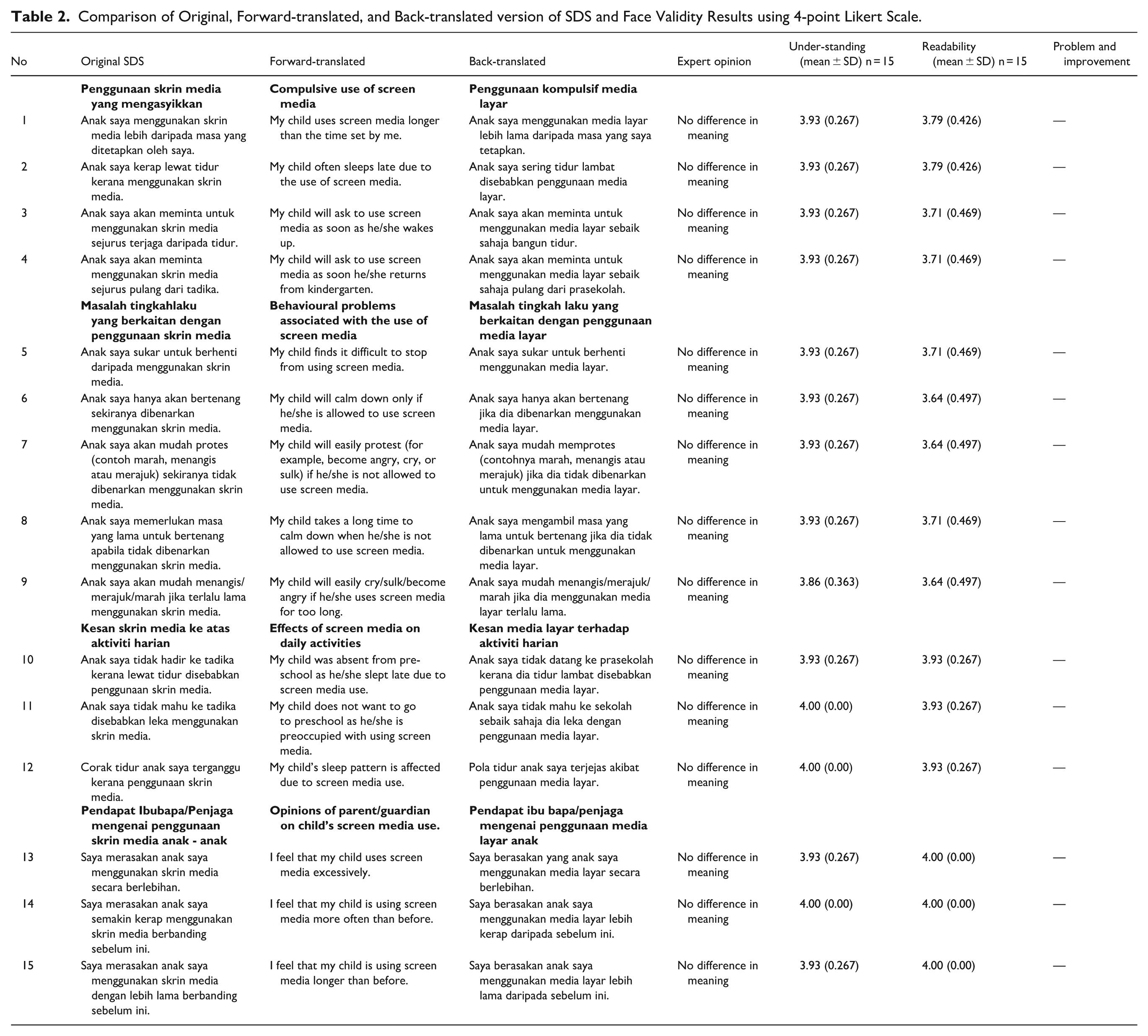
Table 2 compares the original SDS with its forward and backward translations by 2 language experts, showing that the English version closely aligned with the original Malay version. An expert in addiction agreed there were no differences in meaning. Fourteen eligible participants, who were separate from the 195 respondents in the main study, reviewed and assessed each construct. Face validity was evaluated using a 4-point Likert scale to measure readability and clarity. All items scored above 3.5 out of 4, indicating that the translated items were easy to understand and suitable for the target population (Table 2). The questionnaire took 15 to 20 min to complete.
Comparison of Original, Forward-translated, and Back-translated version of SDS and Face Validity Results using 4-point Likert Scale.
Exploratory Factor Analysis (EFA)
To assess factorial validity, both the Kaiser-Meyer-Olkin (KMO) test and Bartlett’s Test of Sphericity were conducted. The KMO value of 0.853 indicated strong sampling adequacy, and the highly significant result from Bartlett’s Test (P < .001) confirmed that the correlations among variables were sufficient to proceed with factor analysis. Principal Component Analysis (PCA) was then applied to the 15 items, and 4 components with eigenvalues greater than one were retained, following the Kaiser criterion. These 4 components accounted for 68.49% of the total variance, suggesting that they captured most of the important patterns in the data and reflected the intended structure of the original SDS.
Further analysis using Varimax rotation helped clarify the groupings of the items. The first component, labelled Behaviour, included items i6 to i9. The second; Tolerance, comprised items i13 to i15. The third component; Preoccupation, was represented by items i1 to i4, while the fourth; Activity, included items i10 to i12. One item, i5, showed notable loadings on both the Behaviour and Preoccupation components, indicating it may relate to both constructs. Overall, the factor structure aligned well with theoretical expectations and supported the instrument’s construct validity.
Confirmatory Factor Analysis (CFA)
CFA was performed to validate the 4-factor structure of the SDS (preoccupation, behaviour, activity, and tolerance). The model showed an acceptable fit, with fit indices meeting the required thresholds; RMSEA was 0.08, CFI was 0.92, and the Chi-square/df ratio was 2.36, all indicating a good model fit. Factor loadings for all items exceeded 0.50, supporting unidimensionality. While most constructs met the required Average Variance Extracted (AVE ≥0.50), the preoccupation factor had a slightly lower AVE (0.40). Nonetheless, Composite Reliability (CR) values for all factors were above .60, confirming adequate convergent validity and internal consistency (Figure 2).

CFA model.
Reliability—Internal Consistency
The SDS English version demonstrated strong internal consistency, with an overall Cronbach’s alpha of .891. Each domain showed acceptable reliability, with alpha values above .7. Preoccupation (compulsive use) had an alpha of .712, behaviour .842, activity .810, and tolerance .884. These results indicate the scale is consistently measuring the intended constructs.
Result of SDS English Version
Using the established cut-off score of 24.5 from the Malay SDS, the English version classified 74.4% of preschool children in the sample as screen media dependent. Among them, 23.1% had mild dependency, 33.8% moderate, and 17.4% severe. This rate is notably higher than in the original Malay SDS study, suggesting a concerning level of screen media dependency among the children surveyed.
Discussion
This study found high access to internet (90.8%) and mobile data (95.4%), similar to findings in Kuantan (86.7%) and Kuala Lumpur (98%).12,13 TVs were the most used devices (81.0%), followed by smartphones (72.3%), differing from other studies where smartphones were dominant.12,13,15 Streaming videos was the main activity (80.5%), consistent with studies in Kuantan and Kuala Lumpur, though in Kedah, smartphones were mainly used for education. 15 WHO and AAP recommend limiting screen time to under 1 h daily for children aged 2 to 5 years.3,4 However, this study found that most children exceeded these guidelines, consistent with previous Malaysian.12,13,16 and global studies.12,13,16-20 On weekdays, 57.4% of children surpassed the limit, rising to 76.4% on weekends. This reflects a notable increase in screen time during weekends, a trend observed both locally and internationally. 21
Excessive screen time can negatively impact children’s physical health, mental well-being, and overall development, including neurological function and gene expression.3,10,22-25 In this study, common physical symptoms reported included eye strain, poor sleep, and fatigue (25.6% each), followed by poor eating habits (21.5%), sedentary lifestyle (12.8%), headaches (7.7%), and musculoskeletal pain (5.6%). Behaviourally, poor attention was most frequent (57.9%), consistent with earlier findings.5,24,26 Other symptoms included tantrums (30.8%), anger (27.2%), tearfulness (13.3%), lying (7.2%), and anxiety (4.6%).10,22 Given the potential harms of excessive or unsupervised screen time on child development, it is important for parents to engage in open discussions about media, set appropriate time limits, and co-view content. Parental mediation plays a key role in fostering healthy media habits in children.
The rising screen dependency among preschoolers globally, including in Malaysia, is shaped by technological, cultural, and social factors. Addressing this requires effective screening tools that are both culturally and linguistically appropriate. Such tools can be adapted from existing questionnaires or newly developed based on expert input, literature, and focus group discussions. The original Malay SDS developed by Abdul Hadi 12 in 2022, was the first tool of its kind in Malaysia. An English version is crucial for use in the country’s multilingual context. Cross-cultural adaptation involves more than direct translation, ensures the tool’s relevance across different cultures and languages.
This study aimed to adapt the Malay SDS into English using forward and backward translation methods, as outlined by Cheung in their study. 27 Translators with expertise in addiction, language, and English proficiency were involved. Linguistic experts and investigators collaborated to ensure the translated version maintained the original meaning. Expert validation confirmed that the content was clear and understandable, with only minor revisions needed. Face validity testing showed the questionnaire was easy to read, with all items scoring above 3.5 on a 4-point Likert scale. 28 Pilot testing with randomly selected parents of preschoolers further supported the questionnaire’s suitability for English-speaking populations, helping to minimise selection bias. 28
The study followed Nunnally’s rule of thumb (10:1 ratio), targeting 195 respondents for the 15-item SDS, including an allowance for dropout. The sample size was confirmed suitable for factor analysis through a high KMO value of 0.853 and a significant Bartlett’s Test (P < .001), indicating sufficient inter-item correlations. 29 A scree plot and PCA revealed 4 components with eigenvalues above 1, explaining 68.49% of total variance, consistent with the original SDS. PCA with Varimax rotation grouped items into 4 domains: Behaviour (i6-i9), Tolerance (i13-i15), Preoccupation (i1-i4), and Activity (i10-i12). Item i5 showed cross-loading (0.492 and 0.517) but was classified under Behaviour based on expert consensus. Further qualitative research may support this classification.
The CFA assessed construct validity using factor loadings, AVE, and Composite Reliability (CR). All factor loadings exceeded 0.50, supporting item reliability. AVE values were 0.563, 0.735, 0.396, and 0.653 for compulsive use, behavioural issues, activity disruption, and parental opinion domains, respectively. While 3 constructs met the AVE ≥0.50 threshold, the activity domain (0.396) fell short. However, as AVE is conservative, CR was relied upon, with all domains exceeding .60 (.835-.892), indicating good internal consistency.16,30 Model fit indices were RMSEA = 0.080, CFI = 0.923, and Chi-square/df = 2.307, reflecting an acceptable fit 30 similar to the original SDS. 12 Overall, the English SDS version shows strong construct validity and reliability, with minor refinements needed in the activity domain.
Reliability is key in behavioural scales, reflecting the consistency of measurements. Cronbach’s Alpha, a widely used metric, was applied to assess the internal consistency of the English SDS, which is based on DSM-V substance use disorder criteria. Alpha values range from 0 to 1, with >.7 considered acceptable, >.8 good, and >.9 excellent.31,32 The overall Cronbach’s alpha for the English SDS was .891 (95% CI), closely matching the original Malay version (.899). 12 Domain-specific alphas were .712 (compulsive use), .842 (behavioural problems), .810 (effects on daily activities), and .884 (parental opinions), all indicating acceptable to excellent reliability. No item deletion improved the total alpha, confirming each item’s contribution to the scale. Although the compulsive use domain showed a wider CI (0.639-0.772), its alpha of .712 remains acceptable. The overall reliability is strong, supported by adequate sample size per KMO standards, with the other domains showing solid internal consistency.
The SDS scores range from 15 to 60, with scores above 24.5 indicating screen media dependency. In this study, 74.4% of preschoolers in Seremban were found to be dependent. Among them, 23.1% had mild, 33.8% moderate, and 17.4% severe dependency. Those with moderate to severe scores were referred for further assessment. This prevalence is higher than previous studies in Kuantan (49.2%) and Kuala Lumpur (65.7%), reflecting a rising trend in screen dependency among Malaysian preschoolers and globally.5,12,13,33,34
Although the study involves translation and validation, it provides the first English version of the SDS for preschool children in Malaysia.12,13 In a multilingual country where English is widely used in healthcare and education, this validated tool fills an important gap by enabling bilingual assessment, supporting cross-cultural comparisons, and facilitating broader research and clinical use.
The SDS-English version can be used in primary care, paediatric clinics, preschools, community programmes, and digital parenting interventions. 11 Its brevity makes it suitable for routine screening, early identification of at-risk children, and guiding behavioural counselling or referral.
Limitations of Studies
While this study offers valuable insights through the translation and validation of the English version of the SDS, several limitations must be acknowledged. Since the original SDS was based on Malaysian cultural values, the English version may not fully reflect the diverse cultural contexts within Malaysia. Respondents less fluent in English might face comprehension issues, potentially affecting the results.
The study sample was limited to English-literate parents from 1 district, which may limit generalisability. Future studies should validate the tool in other Malaysian regions and translate the SDS into Mandarin and Tamil to better represent Malaysia’s multiethnic population.
As a parent-reported tool, the SDS is subject to recall and social desirability biases. Many children spend their day in kindergarten or with maids, so parents may rely on second-hand information, leading to inaccuracies. Incorporating caregiver logs or direct observations could improve the accuracy of screen time reporting.
The construct validity was assessed using a sample of 195, which may limit the generalisability of the findings. Future studies should include larger and more diverse samples and consider qualitative methods like interviews to explore cultural and linguistic nuances affecting the English SDS. Given Malaysia’s multicultural society, translating the SDS into other major languages such as Mandarin and Tamil is recommended to ensure broader accessibility and cultural relevance across different ethnic groups.
Conclusion
The findings confirm that the translated English version of the SDS is a reliable and valid tool for identifying screen media dependency in Malaysian preschoolers aged 4 to 6 years. The thorough translation and psychometric testing support its cultural relevance, strong internal consistency, and solid construct validity. Its simple format makes it practical for use by educators and healthcare providers. Early identification of at-risk children enables timely interventions to mitigate the negative effects of excessive screen time. Overall, the validated SDS supports healthier screen habits and promotes well-being among young children in today’s digital age.
Footnotes
Ethical Considerations
Ethical approval was obtained from the IIUM Research Ethics Committee (IREC), ID No.: IREC 2022-223.
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Consent for Publication
All participants consented to the publication of the findings.
Author Contributions
Azwanis Abdul Hadi: Research proposal, Literature review, Data analysis, Editing, and supervision. Nadirah Zainoren: Research proposal, Literature review, Data collection, Data analysis, Writing, and editing. Abdul Hadi Said: Research proposal, Reviewing, Editing, and supervision. Muhammad ‘Adil Zainal Abidin: Data analysis and Review and Editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available on reasonable request.