
Abstract
Background:
Digital health literacy (DHL) may be important in promoting health. However, there is little understanding of how social support and utilizing electronic resources are associated with DHL.
Objectives:
To assess whether perceived social support of internet use, use of digital resources, and medical services serve as mediators and moderators in the pathway between DHL and self-reported health (SRH).
Methods:
A cross-sectional telephone survey of 587 respondents aged 60+ was conducted in Israel in 2024. Respondents reported their DHL, SRH, perceived support of internet use, use of digital resources, and sociodemographic measures. Information regarding their actual use of digital health services for 2024 was retrieved from the healthcare service database. Statistical analyses were performed using moderation mediation models with SRH as the dependent variable.
Results:
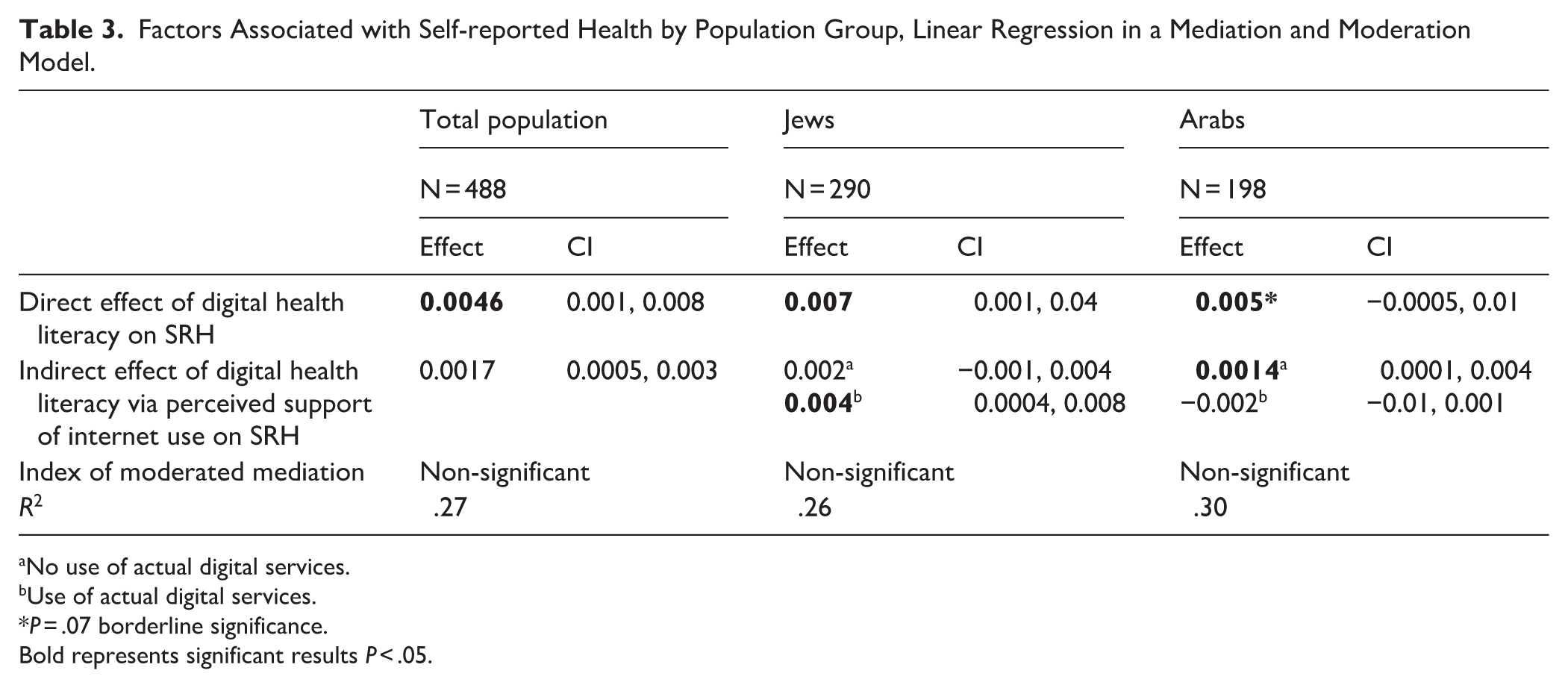
Perceived social support in internet use was a significant mediator between DHL and SRH. The direct effect was 0.0046 (CI 0.001, 0.008) and the indirect effect was 0.0017 (CI 0.0005, 0.003). Use of digital resources and services were not associated with SRH and do not serve as significant moderators of the association between DHL and SRH.
Conclusions:
As more medical services have and are becoming digitalized the importance of the digital divide is increasing. Perceived support in using digital resources may enable individuals to overcome the digital divide and benefit from the digital resources available. It is important to note that findings are correlational due to the cross-sectional nature of the study.
Keywords
Introduction
Digital Health Literacy (DHL) has emerged as a crucial competency for navigating the use of technology generally and in health services specifically.1-5
DHL is generally defined as an individual’s “ability to seek, find, understand, and appraise health information from electronic sources and apply the knowledge gained to addressing or solving a health problem.” This concept, initially termed “eHealth literacy” 4 has continued to evolve alongside technological advancements. DHL is defined as “the ability to search for, access, understand, appraise, validate, and apply online health information, and the ability to formulate and express questions, opinions, thoughts, or feelings when using digital devices.” 3 In this study we adopt this definition.
On average nearly 40% of populations across Europe reported difficulties in processing digital health information. Family, friends, and others could help navigate access for those having difficulties in utilizing the digital health service. 6
The increasing reliance on digital health resources, however, highlights a significant challenge: the digital divide.7-9 This divide refers to the inequitable access, use, and outcomes of technology among various societal subgroups. Populations with lower income or education, culturally diverse minorities, older age, and rural residents are often less likely to possess the necessary access or skills to effectively use technology, including digital health tools. This disparity raises concerns that well-intentioned efforts to digitalize healthcare, if not carefully implemented, could inadvertently worsen existing health inequities. Understanding the predictors of digital health service uptake is therefore a crucial first step to prevent such pitfalls.
Research has shown a link between DHL and various health outcomes, such as self-rated health (SRH) and health behaviors,3,10-17 often showing inconsistent results. DHL is considered a key skill for disease management and healthcare in the digital age. Despite its recognized importance, the average levels of DHL vary between population groups 13 suggesting a significant gap in skills within various vulnerable groups.
Socioeconomic and social factors, internet use, and experience are consistently strong positive correlates of better DHL: higher social status, higher frequency of internet use, prior internet experience, and specifically using the internet for health-related information, are all associated with higher DHL levels.1,2,12,15
Beyond these individual and demographic factors, social support emerges as a critical factor. Most of the research regarding social support was performed regarding HL and found to be a mediator between HL and SRH.18-20 Social support may explain to some extent the association between HL and SRH, suggesting social support helps people with low levels of HL to perform tasks that improve their health. 18 Yet, this is under-explored as a determinant of DHL and research regarding HL cannot be generalized to DHL as they measure different abilities of individuals, and the association between them is only moderate. 21 Existing research highlights the significance of social support as a correlate of older adults’ utilization of electronic information resources for health-related purposes. Support from family and friends has been shown to effectively improve DHL.22,23 Strategies such as “technology feedback, intergenerational support, and peer education” are proposed as effective means to bridge the digital divide, particularly for older adults. These findings underscore the importance of social context in facilitating digital health engagement. The role of Health Information Surrogates (HISs), individuals who seek health information on behalf of others, such as family or friends further illustrates the profound impact of social interactions on eHealth use. 24 The findings of 2 recent studies exploring the pathways in which health literacy and social support are associated among older adults, showed that media exposure 25 and having a smartphone 26 play a crucial role in this pathway. However, the focus of these studies was general health literacy, as differentiated from DHL.
In the present era, it is important to understand how DHL relates to the use of web-based health services, as we expect those with high DHL to be more adapt in using the digital services and portals.27,28 Most studies have looked at self-reported use of services, 28 however, this study utilizes the actual use of portal health services.
Despite the growing recognition of the social factors in the way DHL could be associated with health, there remains a need for more in-depth research to fully understand this intricate relationship and the pathways leading from DHL to health. While individual factors and broad health outcomes have been studied, the specific mechanisms and pathways through which social support influences the development of DHL skills and its subsequent impact on health outcomes require more study.
Israel consists of 2 main population groups differing in language, religion, and culture, Previous studies have found differences in use of health services 29 and HL; therefore, exploring both population is important. 30 It is important to mention that both groups receive healthcare as part of the national health insurance law.
This study explored the relationship between DHL, perceived support from social networks in internet use, use of digital health services or portals and SRH. The novelty of the present analysis lies in including actual data on use of digital health services in the study.
Methods
A cross-sectional survey design was utilized to examine the associations between DHL, social support in internet use, self-reported health (SRH), reported and actual use of digital resources, and healthcare services (Figure 1). In addition to the self-reported data, the study analyzed secondary data based on actual use of digital health services. The survey was performed during the months June to September, 2024.

Model describing factors associated with self-reported health.
Both the University of Haifa Institutional Review Board (IRB) and the Clalit Health Services (CHS) IRB approved the study protocol, Numbers: 298/25 and 0101-23-COM2. All participants provided verbal informed consent before commencing the telephone interview.
The target population consisted of Israeli citizens, both Jewish and Arab, including men and women aged 60 years and older, receiving health services from CHS.
We received a random list of 5688 potential participants, aged 60 years and over (first name and contact phone details) from CHS; each potential participant was assigned a unique id number before the file was sent to the survey company. Study size was calculated based on the assumption that the response rate will be around 20% and a sample of 600 will provide a sufficiently large enough sample to identify significant mediator and moderators and a separate analysis of Arabs and Jews. Telephone interviews were conducted either in Hebrew, Arabic, or Russian, according to the preference of the interviewee. The overall response rate was 20.4% and specifically 17.24% for Jews and 32.05% for Arabs, after deleting phone numbers with no response after at least 3 attempts. Six hundred participants agreed to be interviewed, sampling error of 2.04%.
The interviews (n = 13) with the ultraorthodox Jewish respondents were not included in the analysis, as they significantly differed from the other groups in their general exposure and use of the internet due to religious and social restrictions. The analysis included responses from 587 individuals. Thirty-eight respondents did not identify themselves as neither Arab nor Jewish, selecting “other,” and were therefore excluded from the analysis.
Following the survey administration, use of the digital healthcare services accessed through the CHS portal was provided for each participant retrospectively for the year 2024. This was extracted by the CHS Information Technology (IT) staff and matched to the survey participant and anonymized for analysis.
The questionnaire included socioeconomic variables, DHL, use of internet resources, social support of internet use, and SRH. The questionnaire was translated into Russian and Arabic by professional translators and translated back to Hebrew to double check accuracy of translation. A pretest of the questionnaire was performed with 30 participants to identify problems in understanding the questions after which small changes were made.
The Dependent Variable
Self-reported health: (SRH) “How would you describe your general health, physical, and mental,” with a 5-point scale, from bad to excellent. This question has been validated and used in multiple studies in Israel31,32 and has been shown to be a very strong proxy for mortality. 33 The continuous form of self-reported health was used for analysis.
Independent Variables
Digital health literacy (DHL): Digital Health literacy was measured using the HLS19-DIGI Instrument 3 comprised of 8 items on Digital Health Literacy. The DHL scale (HLS19-DIGI) was validated in 13 countries including Israel. Respondents were asked how difficult or easy is it for them to access, understand, appraise, and apply online health information and resources. (Cronbach’s alpha = .89 in the current study.) A mean score for the 8 items was calculated for those that answered at least 4 of the items. For 66 participants this measure was missing.
Reported use of digital resources was measured by the mean of 6 items. Participants reported the frequency of using the following resources for health concerns during the last 6 months: websites, social media, digital devices, mobile health apps, digital communication with health services, and other digital resources for receiving health/medical information. The answers included a 5-level scale, ranging from “less than once a week” (1) to “more than once a day” (5). In addition, respondents could answer “not relevant for me” or “do not know.”
Perceived social support in internet use: Respondents were asked: “How difficult or easy is it for you to ask for help or receive advice regarding surfing the web, and for example finding a specific site or service.” The answers included a 5-level scale from 1 “very difficult” to 5 “very easy.” Hayat et al 23 used this question in their study and found that respondents with low eHealth literacy who were able to ask for help for online activities, reported better perceived health compared to respondents who did not get help. This suggests criterion validity.
Socioeconomic and demographic status: Participants reported their gender, age, ethnicity (Arab or Jewish), education (did not complete high school, completed high school, and hold an academic degree), and perceived social status (PSS; the MacArthur ladder).34,35
Actual use of digital health services: CHS collects information on the following digital activities of the members regarding health services: online consultation with a physician; requests for tests/procedures and referrals; requests for prescriptions (eg, refill of routinely-taken medication); office/administrative request; payment refunds; consultation with clinic administrators/service staff; funding for procedures implemented outside the CHS system. These activities were grouped into 2 categories: activities involving a physician (actual use of digital medical services) and activities involving administration (actual use of administrative health services). In addition, an overall score was computed. The data was extracted for 2024.
There were no missing data for the socioeconomic, social support, and health related variables. For the other variables it was acceptable to reply “not relevant” or “do not know.”
Statistical Analysis
Categorical variables were analyzed using frequency and percentage distributions, while continuous variables were examined using mean and standard deviation. Differences between Jews and Arabs were calculated. Linear regression models were computed for Jews and Arabs separately and combined to assess the association between SRH and the other factors in the model (Figure 1). The model in Figure 1 was tested with a mediation moderation regression model using R. Perceived social support in internet use was tested as a mediator and use of resources and services was tested as a moderator. We tested the assumptions of normality of the residuals for the main variables and the assumptions hold. The socioeconomic variables added as covariates were: age, perceived social status, and education. These were found to be significantly associated with either outcome or predictor variables. There was no significant association between use of digital resources and SRH, suggesting use of digital resources could not have a mediating effect. However, the possibility of a moderation effect, was tested. Direct effects and indirect effects are reported. Participants with missing data for the variables in the model were not included in the moderation mediation analysis (99).
This manuscript was prepared in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) cross-sectional reporting guidelines for the reporting of observational studies. 36 The checklist is available as Supplemental Material.
Results
Table 1 presents the characteristics of the sample population by ethnicity. The Jewish sample was significantly older than the Arab sample (age: 71.4 compared to 69.0, respectively). Jews had significantly higher levels of DHL compared to Arabs, and reported better SRH. Likewise, education and actual use of digital health services were significantly higher among Jews.
Characteristics of Participants by Population Group, Mean, SD, Number, and %.

P < .05 difference between Jews and Arabs.
Table 2 presents the linear regression models identifying factors associated with SRH. Perceived social support in internet use and perceived social status (PSS) were both associated with SRH in both the general model and separately for Arabs and Jews. Respondents with higher levels of support in internet use and PSS reported better health. However, DHL, age, and education were significantly associated with SRH only among Jews. The model for the total population indicates that the 5 variables are significantly associated with SRH. Reported use of digital resources and actual use of digital medical services were not associated with SRH of the total population and among Jews. However, among Arabs, actually using digital services was significantly associated with worse SRH – the lower the use of digital health services, the worse the SRH.
Factors Associated With Self-reported Health by Population Group, Linear Regression Model. Standardized Beta, P, and Confidence interval.

The hypothesis that perceived social support in internet use may serve as a mediator in the association between DHL and SRH was tested in a mediator-moderator model where the reported use of digital resources and actual use of medical digital services were tested as moderators of the association between DHL and SRH. Figure 1 depicts the model and Table 3 presents the statistical results of the model. Other models were tested; for example, we tested models with 1 moderator and not 2, or with no moderators and a model with mediation alone. However, they were not found to reach acceptable model fit indices. Reported and actual use of digital resources and services were not associated with SRH, therefore we did not test them as mediators between DHL and SRH.
Factors Associated with Self-reported Health by Population Group, Linear Regression in a Mediation and Moderation Model.
No use of actual digital services.
Use of actual digital services.
P = .07 borderline significance.
Bold represents significant results P < .05.
In the total population, perceived social support in internet use was a significant mediator between DHL and SRH, where the direct effect was .0046 and the indirect effect was .0017 (P = .01). Use of digital resources and actual use of digital medical services were not significant moderators in this full model of association between DHL and SRH (Table 3). The index of the moderated mediation was non-significant (P = −.0000).
When dividing the population into 2 ethnic groups (Arabs and Jews), the significance of the mediation diminishes, this may be due to the samples being smaller. Among Jews, perceived support in internet use was a significant mediator only when there was use of actual digital medical services, but not when no digital medical services were used. The moderation of the association between DHL and SRH was not significant among Jews.
Among Arabs, perceived support in internet use was only borderline significant as a mediator between DHL and SRH (P = .07). Perceived support in internet use was a significant mediator only with no use of actual digital medical services, but not significant when actual digital medical services were used. The moderation effect of use of digital services was not significant among Arabs either.
Discussion
Healthcare services in the developed world are increasingly implementing new digital technologies for the population to avail information and various healthcare services. However, it is not exactly known what affects the ability to utilize these services in various populations. This study attempted to unravel the complexity of determinants of health that may be important in the context of modern healthcare systems. The individual’s level of digital health literacy (DHL) could be important for determining the capacity for using digital resources and healthcare services and adopting the new technologies to ultimately manage their healthcare.
Therefore, this study examined the association between DHL, social support in internet use, self-reported health (SRH), and actual use of digital health services among older adults in Israel. Our findings contribute to the growing literature on DHL by highlighting the role of social support as a mediator in the pathway between DHL and health and by exploring ethnic group differences within the Israeli context.
DHL and SRH
Consistent with previous research,3,11,12,37 we found that higher DHL was associated with better SRH, and that this relationship was partially explained by social support in internet use. This aligns with recent studies suggesting that DHL contributes not only to improved access and use of health information but also to enhanced self-management, health behaviors, and communication with providers.10,17 However, in our sample, DHL was significantly associated with SRH mainly among Jews, whereas among Arabs, this association was weaker and nonsignificant. This divergence underscores the importance of considering cultural, social, and structural factors when evaluating the benefits of DHL. However, it could also be attributed to the smaller sample size of Arabs in our study. We do not assume causality as this is a cross-sectional survey.
The Mediating Role of Social Support in Internet Use
A key contribution of this study is the finding that perceived social support in internet use mediated the relationship between DHL and SRH. This builds on and supports previous work that identified social support as a mediator between general health literacy and health outcomes.18-20 In the digital context, family members, peers, and intergenerational networks can provide crucial assistance in navigating online services, particularly for older adults who may lack confidence in digital skills.22,23 Our findings resonated with the concept of “Health Information Surrogates,” whereby individuals relied on others to search, interpret, and use digital health resources on their behalf. 27 Interestingly, subgroup analysis revealed that the mediating role of social support differed by ethnicity and by actual use of digital health services. Among Jews, mediation was significant only for those who used digital services, suggesting that support enhance d the ability of digitally active individuals to benefit from their DHL. Among Arabs, however, social support mediated the DHL–SRH association only among those not using digital services, possibly reflecting reliance on family networks to compensate for low DHL or limited engagement with formal digital health platforms. These findings highlighted the cultural context of digital engagement, where family-based support systems may substitute for direct interaction with digital health tools.
The mediating role of perceived social support in internet use can be interpreted through social capital theory and ecological models of health literacy. From a social capital perspective, social ties function as resources that enable individuals to access, interpret, and act upon health information.38,39 In the digital health context, support from family and peers constitute both bonding and bridging social capital that helps translate digital health literacy into actual health-related action. Our findings may suggest that digital skills can be enhanced for improving SRH when embedded within supportive social networks that facilitate meaningful use of digital information.
In addition, ecological models of health literacy further conceptualize literacy as an interaction between individual abilities and social, institutional, and cultural environments rather than a purely personal attributes. 40 Within this framework, perceived social support represents a key interpersonal-level mechanism that modulated whether digital resources are effectively transformed into health benefits.
Limited Role of Digital Service Use
Contrary to expectations and some prior research,27,28 neither reported nor actual use of digital health services moderated the association between DHL and SRH in the overall sample. This may be explained by the relatively low uptake of digital services in the study population, particularly among Arabs (92.4% reported no use), and the fact that simple measures of frequency may not capture qualitative differences in the way services are used. In fact, among Arabs, actual use of digital services was associated with poorer SRH, possibly reflecting reverse causality where individuals with poorer health may be more likely to seek digital services, or dissatisfaction with services that were not adapted to cultural or linguistic needs. Actual use of digital services in this study strengthens the results, as they were not based on self-report.
Ethnic Disparities in DHL and Digital Health Engagement
The large disparities between Jews and Arabs in DHL, education, and use of digital services echo ed earlier findings regarding health service use and health literacy disparities in Israel.29,30 Arabs in our study reported much lower DHL and substantially less engagement with digital health services, compared to Jews, which likely contributed to the weaker association between DHL and SRH. Previous research has linked these disparities to differences in socioeconomic status, language barriers, and cultural norms regarding health communication. 31 These findings reinforced concerns that digitalization of health services, if not accompanied by tailored support strategies, may widen the digital divide and exacerbate health inequalities.7,9
An additional ecological insight regarding the ethnic differences observed in the mediation patterns can be suggested. Among Arab participants, social support appears to compensate for lower engagement with digital services, reflecting dependence on family-based social capital in navigating health information. Among Jewish participants, mediation was primarily evident among those already engaged in digital medical services, suggesting a synergistic interaction between institutional access and social facilitation. Overall, these findings support a socially embedded model of digital health literacy, in which social capital and ecological context are central mechanisms shaping the health impact of digital skills.
Implications for Policy and Practice
Our findings have several implications. First, interventions to improve DHL among older adults should be complemented by strategies to strengthen social support systems, including peer education, intergenerational mentoring, and community-based digital literacy programs.22,23 The development of digital navigators could help older adults cope with the new technologies. 41 Second, health systems should acknowledge cultural and linguistic diversity when designing digital platforms to ensure equitable access and usability for minority populations. Finally, measuring DHL alone may be insufficient; incorporating assessments of social support and perceived confidence in digital use may provide a more comprehensive understanding of individuals’ capacity to benefit from digital health innovations.
Strengths and Limitations
This study has several strengths, including the use of a validated DHL instrument, 3 the inclusion of both self-reported and objectively measured digital service use, and the focus on an older population that is often underrepresented in digital health research. In addition, the study takes a deeper dive into models explaining the determinants of DHL. 42 The random sample of older participants from the largest healthcare service in Israel (52% of Israeli citizens) enables us to generalize to some degree to the wider older population in Israel, and could be tested in other countries.
We acknowledge several limitations of this study. The cross-sectional design prevents causal inference and differences observed between Arabs and Jews may partly reflect unmeasured contextual factors such as digital infrastructure, health service availability, or intra-family caregiving norms. In addition, the relatively low response rate may introduce selection bias, although the inclusion of both survey and database analysis strengthens the validity of the findings. Future research should adopt longitudinal designs and interventions to clarify the causal pathways linking DHL, social support, and health. Qualitative studies could provide deeper insight into how cultural values and family roles shape digital health engagement. Furthermore, evaluating interventions that combine individual skill-building with supportive social environments could shed light on effective ways to bridge the digital divide and promote equity in digital health use.
Conclusions
This study demonstrates that social support in internet use plays a mediating role in the relationship between DHL and SRH among older adults, with distinct patterns across ethnic groups in Israel. While DHL is an important determinant of health in the digital era, its importance is dependent upon the social and cultural context in which digital services are consumed. Tailored interventions that enhance both digital skills and supportive networks are essential to ensure that digital health innovations reduce rather than widen existing health disparities.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319261418534 – Supplemental material for Digital Health Literacy and Self-Reported Health in Older Adults: The Role of Social Support in Internet Use
Supplemental material, sj-docx-1-jpc-10.1177_21501319261418534 for Digital Health Literacy and Self-Reported Health in Older Adults: The Role of Social Support in Internet Use by Orna Baron-Epel, Efrat Neter, Ester Eliyahu, Peter W. S. Chang, Tuyen V. Duong and Diane Levin-Zamir in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
We wish to thank Talish Razi, Clalit Health Services for her assistance in data extraction.
Ethical Considerations
This study was approved by the institutional review board of both the University of Haifa (#298/25) and CHS (#0101-23-COM2).
Consent to Participate
All respondents expressed consent before their participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Science & Technology, Israel and The National Science and Technology Council Taiwan.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be provided on request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.