
Abstract
Introduction/Objectives:
Despite the efficacy of vaccines in preventing disease and disability and their cost-effectiveness, a proportion of the population remains reluctant to vaccination. Vaccination literacy is one of the main determinants of vaccine decision-making. The aims of this study were to assess the measurement properties of the Hungarian version of a vaccination literacy instrument and describe the level and determinants of vaccination literacy among the Hungarian adult population.
Methods:
A cross-sectional study was conducted on a sample of 1205 Hungarian adult respondents within the European Health Literacy Population Survey 2019–2021. The data were collected by computer-assisted telephone survey in December 2020. The questionnaire covered the following topics: sociodemographic data, self-perceived health, social support, and general and vaccination literacy. The instrument’s internal consistency was measured using Cronbach’s alpha, its reliability was assessed based on the Spearman–Brown correlation coefficient. The construct validity of the questionnaire was examined using principal component analysis based on a polychoric correlation matrix. Multivariate ordered logistic regression analyses investigated the relationship between vaccination literacy and other relevant variables.
Results:
The Cronbach’s alpha was 0.78, while the Spearman-Brown correlation coefficient was 0.725. The principal component analysis extracted 1 significant factor that explained 69% of the total variance. The Hungarian adult population had a good level of vaccination literacy (mean score: 82.4, 95% CI 74.9-89.8). We found that social support (OR for the moderate support: 1.93, OR for the strong support: 2.19; P < .001 for both), lack of financial deprivation (OR: 2.05, P < .001), and secondary education level (OR: 1.50, P: .024) are positively correlated with vaccination literacy.
Conclusion:
We recommend using the vaccination literacy instrument to identify individuals with inadequate vaccination literacy. Interventions focusing on social support and education to promote vaccine-related information would contribute to enhancing vaccination literacy.
Keywords
Introduction
Vaccines are highly effective and cost-efficient in protecting individuals from diseases, disabilities, and death caused by vaccine-preventable diseases, and although there is overwhelming evidence of their benefits, a significant part of the population doubts the need for and usefulness of immunization.1,2
Numerous factors affect vaccine decision-making; general health literacy (GHL) and vaccination literacy (VHL) are among the main determinants. i Being health and vaccine literate leads to vaccine empowerment, trust in vaccines and their effectiveness, as well as trust in the healthcare system, and results in vaccine acceptance and uptake.3,4
The idea of VHL has flourished within the concept of GHL.5-7 It was first defined by Ratzan in 2011 as “not simply knowledge about vaccines but also developing a system with decreased complexity to communicate and offer vaccines as sine qua non ii of a functioning health system.” 8 (p. 229) The most recent definition of VHL emphasizes that the concept encompasses both skills (at the personal, community, and population levels) and context. According to it, VHL “is linked to health literacy. It entails people’s and communities’ knowledge, motivation, and competencies to access, understand, and critically appraise and apply information about immunization, vaccines, vaccination programs, and organizational processes to access vaccination and to navigate the health system, in order to make informed decisions about vaccines for themselves, the members of their family, and the community, and to appreciate the larger global impact of vaccines with respect to population health.” 9 (p. 4-5)
Previously, there had not been any research in Hungary specifically measuring VHL in general. 10 Hungary joined the Action Network on Measuring Population and Organizational Health Literacy (M-POHL), which was established under the aegis of the World Health Organization’s European Health Initiative and aims to improve health literacy (HL) in the World Health Organization’s European Region. Hungary participated in the Health Literacy Survey 2019-2021 (HLS19), which is M-POHL’s first project. HLS19 was a multicenter cross-sectional study in which data were collected between November 2019 and June 2021. 11
Investigating the measurement properties of the VHL instrument is essential to ensure it measures reliably and validly individuals’ ability to access, understand, appraise, and apply information related to vaccination. Demonstrating its psychometric soundness enables proper assessment of VHL levels within the population and facilitates comparison across studies and contexts. However, validation alone does not fully capture the complexity of VHL as a public health construct. It is equally important to examine the determinants of VHL in order to identify the social, economic, and educational factors that shape individuals’ capacity to make informed vaccination decisions. Understanding these associations can inform the design of targeted interventions and communication strategies aimed at improving VHL and ultimately enhancing vaccine confidence and uptake within the population. Therefore, the aims of our study were to (1) assess the measurement properties of the Hungarian version of the HLS19-VAC instrument, the VHL instrument of the HLS19, (2) describe the level of VHL in the Hungarian adult population, and (3) investigate its determinants.
Methods
Study Design and Sampling
A nationwide cross-sectional survey was conducted on a sample of 1205 people (response rate calculated based on the number of completed interviews divided by the sum of interviews and refusals: 27%) aged 18 and over among Hungarian residents as part of the HLS19. 12 The study sample was representative of the Hungarian population by age, sex, educational level, and place of residence.
A professional polling company collected the data in December 2020, using computer-assisted telephone interviews (CATI) in Hungarian in response to the COVID-19 pandemic. A probability sampling strategy was used which included stratification based on regions/type of settlements to define the case numbers to achieve per each, while ensuring random selection by using a pool of phone numbers drawn from public registries. The probability sample had been selected in multiple stages with proportional stratification during the data collection. The regions formed the first strata, type of settlements the second. The localities were chosen from these strata with the help of probability-proportional-to-size (PPS) sampling. Afterwards, it was determined how many persons should get into the sample from each type of settlement within each region in accordance with the proportion of the basic population in the whole adult population broken down to regions, and the proportion of the population of the type of settlement within the region. After the localities and the number of target interviews for each have been set, the phone numbers were selected from the online public phonebook. This process complemented by a quota for sex/age/region/type of settlement control during fieldwork ensured a representative sample of the Hungarian population aged 18 years and older who are living in private households. Details of weighting and data collection have been described elsewhere. 13 The Medical Research Council Scientific and Research Committee, Hungary (IV/10181-3/2020/EKU) approved the study and informed consent was obtained from all participants in accordance with the Declaration of Helsinki.
Data Collection Domains and Tools
Sociodemographic Data
We collected the following sociodemographic data: sex, age, educational level, child-rearing, being trained in a health profession, self-perceived social status, and financial deprivation. Sex was dichotomized as male and female. Three age groups were set up as 18 to 35, 36 to 65, and 66 years of age and over. Four categories were created for the highest level of education (primary education; secondary education without baccalaureate; secondary education with baccalaureate; college, university degree, or higher). Information about child-rearing and being trained in a health profession was dichotomized as yes or no. The self-perceived social status was measured on a 10-point Likert scale, with step 1 standing for the lowest level in society and step 10 representing the highest level in society. Low level in society was defined as 1 to 4. 12 The difficulty of paying utility bills and paying for necessary medical examinations, treatments, and medications was used as a gauge of financial deprivation. Each question was answered using a 4-point Likert scale ranging from “very difficult” to “very easy”. The available score was calculated on a scale from 0 to 100, based on the combined percentage of “difficult” and “very difficult” responses. Higher scores indicate more severe financial deprivation, a score above 50 was considered deprived. 12
Self-Perceived Health and Social Support
A 5-point Likert-scale (1 – “very bad”, 5 – “very good”) based on the question of the European Health Interview Survey 2019 was used to assess self-perceived health.14,15 The perceived social support was measured using the 3-item Oslo Social Support Scale. Social support is classified as poor below 8 points, moderate between 9 and 11 points, and strong above 12 points.14,15
General and Vaccination Literacy
GHL was measured using the 12-item HLS19-Q12 questionnaire. 16 For each question, the respondent had to select the most relevant answer on a 4-point Likert scale from “very easy” to “very difficult.” The total score was calculated if at least 80% of the questions were answered. 12 The scale has shown high internal reliability in previous Hungarian study. 13
The HLS19-VAC instrument assessed the 4 aspects of vaccination-related information management with 1 item for each aspect. The questionnaire consisted of 4 questions: How easy or difficult would you say it is to find information on recommended vaccinations for you or your family?; understand why you or your family may need vaccinations?; judge which vaccinations you or your family may need?; and decide if you should have a flu vaccination? 12 Respondents were asked to select the most appropriate answer on a 4-point Likert scale (from “very easy” to “very difficult”). The score was calculated based on the valid responses, on the percentage of “easy” or “very easy” answers (0 and 100), where a higher score indicated a higher level of VHL.
Statistical Analyses
The terminology from the COnsensus-based Standards for the selection of health status Measurement INstruments (COSMIN) taxonomy was used when the measurement properties of the questionnaire were described. 17 The internal consistency of the HLS19-VAC instrument was measured using Cronbach’s alpha with the corresponding bootstrapped 95% confidence intervals and “alpha if item deleted” (change in coefficient alpha after removal of a single component), where a value between 0.70 and 0.95 was considered as acceptable reliability. 18 The Spearman rank correlation was used to measure the association between the total scores of GHL and VHL. The Spearman correlation coefficient (rho) was calculated for both the total sample and the socioeconomic subsamples. Correlations are considered moderate if rho >0.4 and strong if rho >0.6. 19
Because of the COVID-19 pandemic, it was not possible for us to perform a “test-retest” analysis with repeated data collection, so an alternative reliability indicator was quantified using the Spearman-Brown split-half reliability method. For this method, the items were randomly allocated into 2 groups, and the total score for each half of the instrument was calculated. The 2 sets of scores were correlated, and the corrected Spearman-Brown correlation coefficients were calculated. Consistency was considered moderate if the correlation was 0.50 to 0.69, strong if the correlation was 0.70 to 0.89 and very strong if the Spearman-Brown coefficient was >0.90. Item-total correlations were also analyzed, with a value greater than 0.3 being considered as acceptable. As a sensitivity analysis, we also tested the internal consistency of the HLS19-VAC instrument in different subsamples. The construct validity of the questionnaire was examined using principal component analysis (PCA) based on a polychoric correlation matrix, which is appropriate for items measured on a 4-point Likert scale. Factorability was assessed using the Measure of Sampling Adequacy (MSA) derived from the anti-image matrix of the polychoric correlations, and the number of components to retain was guided by inspection of the scree plot and parallel analysis with polychoric correlations.
Descriptive analyses were based on data weighted by age, sex, education, and place of residence with 95% confidence intervals (95% CI). Multivariate ordered logistic regression analyses were conducted to examine the relationship between VHL and sociodemographic, social support, and self-perceived health variables. Due to the limited number of items (n = 4) and the resulting discrete score distribution (0, 25, 50, 75, 100), the VHL score was treated as an ordinal variable in these analyses rather than applying arbitrary cut-off points. This analysis was adjusted for self-perceived social status, child-rearing, and being trained in a health profession, and was based on complete case data. The validity of the proportional odds assumption was checked using a full likelihood ratio test comparing the fitted location model to a model with varying location parameters. Associations were quantified using odds ratios (OR) and corresponding 95% confidence intervals (95% CI). A P-value less than 0.05 was considered statistically significant.
Data analysis was performed using the statistical software Stata/IC 16 survey data analysis module (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC), with the SPSS 26.0 software (IBM Corporation, Armonk, New York, USA) and R version 4.4.3 (R Core Team, 2025).
Results
Characteristics of the Sample
Our sample consisted of 1205 people. The mean age of respondents was 48.0 years (min. 18, max. 91 years; SD: 17.5 years), with an almost equal proportion of males and females (47% vs 53%). The largest part of the sample had a secondary education. More than 70% of the respondents rated their level in society to normal. Nearly one-third of respondents were financially deprived and nearly half of them has rated their health as good or very good and received moderate social support (Table 1).
Main Characteristics of the Study Sample (Weighted by Age, Sex, Education, and Place of Residence), and Cronbach’s Alpha Values and Spearman-Brown Correlation Coefficients for the Subsamples.
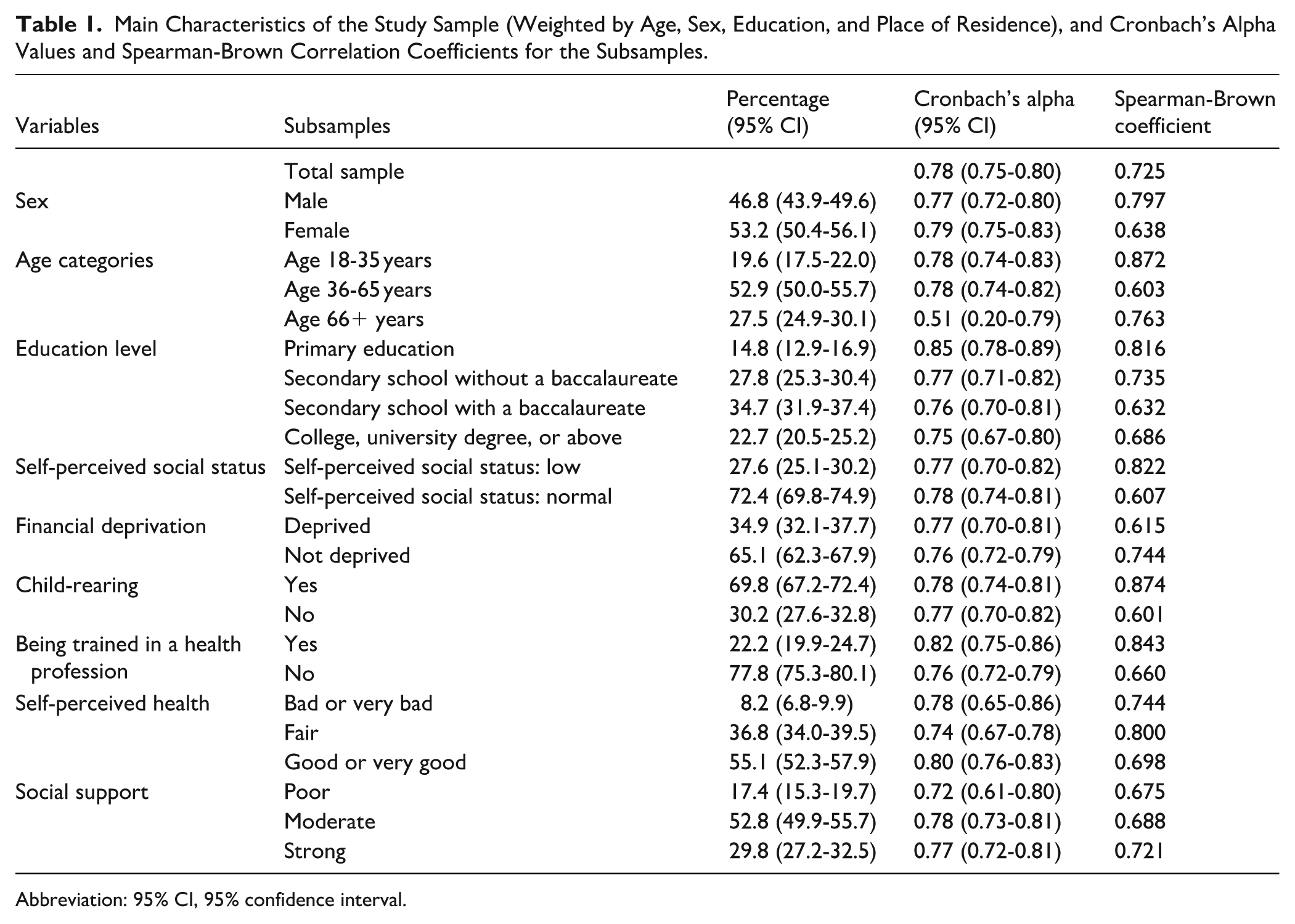
Abbreviation: 95% CI, 95% confidence interval.
Measurement Properties of the Questionnaire
The internal consistency measured by Cronbach’s alpha was 0.78, while the split-half reliability calculated with the Spearman-Brown correlation coefficient was 0.725 for the total sample. Table 1 displays the calculated values for the various subsamples. The Cronbach’s alpha for the subsample showed a quite wide range from 0.51 (age above 65) to 0.85 (primary education). The values of the Spearman-Brown correlation coefficient varied between 0.601 (having no children) and 0.874 (having children).
We tested the Cronbach’s alpha coefficient by removing individual items and found that, except for the last item, removing any item results in a decrease in the coefficient. The item-total correlation coefficients were higher than the minimum acceptable level (0.3) in all cases. The lowest was for the last item (0.74), and the highest was for the third item (0.82).
The Measure of Sampling Adequacy (MSA = 0.794) indicated that the data were suitable for conducting PCA based on the polychoric correlation matrix. Examining the scree plot confirmed the suitability of a 1-factor solution. The PCA extracted 1 significant factor that explained 69% of the total variance. The factor loadings were between 0.73 (“decide if you should have a flu vaccination”) and 0.89 (“understand why you or your family may need vaccinations” and “judge which vaccinations you or your family may need”). Values for uniqueness ranged from 0.21 to 0.47, which means that the common factor explained most of the differences between items (Table 2).
Result of the Principal Components Analysis Based on Polychoric Correlation Matrix, Estimated by the R package “psych”.

We found a statistically significant correlation between GHL and VHL scores for the total sample (rho: 0.41, P < .001) and for all subsamples. It means that respondents with a higher level of GHL are more likely to have a better level of VHL. The strongest correlation, indicating a moderate positive correlation (r: 0.49, P < .001) between GHL and VHL, is found in the primary education group. The lowest correlation is found in the tertiary education group (r: 0.32, P < .001), indicating a weak positive correlation between GHL and VHL scores (Table 3).
Correlation Coefficients Between Health Literacy Scores and Vaccination Literacy Scores for the Subsamples.

Abbreviation: 95% CI, 95% confidence interval. Significant results are in bold.
The Vaccination Literacy of the Hungarian Adults and its Determinants
The weighted mean VHL score in Hungary was 82.4 (95% CI 74.9-89.8), it was the lowest among people with primary education and the highest among non-deprived people (Figure 1). More than one-fifth of respondents found it difficult to “judge which vaccination you or your family may need?” (Figure 2).

The weighted mean vaccination literacy stratified by the respondent socio-demographic characteristics in Hungary.

Distribution of responses to questions in the vaccination literacy instrument (weighted by sex, age, educational level, and place of residence).
Moderate (OR: 1.93, P < .001) and strong (OR: 2.19, P < .001) social support and the lack of financial deprivation (OR: 2.05, P < .001) had a positive effect on VHL. In terms of educational level, we observe that VHL is significantly higher among individuals without a baccalaureate (OR: 1.50, P = .024) compared to primary school graduates (Table 4).
Determinants of Vaccination Literacy According to the Multivariate Ordinal Logistic Regression Analyses.

Abbreviations: OR (95% CI), odds ratio (95% confidence interval); ref., reference category.
Adjusted for self-perceived social status, child-rearing, and being trained in health profession.
Significant results are in bold.
Discussion
The aims of our study were to investigate the measurement properties of the Hungarian version of the HLS19-VAC instrument, to describe the level of VHL of the Hungarian adult population and to investigate its determinants.
The Cronbach’s alpha coefficient (0.78), measuring internal consistency of the instrument, is higher than the acceptable level and the Cronbach’s alpha in the international study (0.72).12,20 The high split-half reliability coefficient suggests a strong correlation between the 2 halves of the test, indicating good internal consistency of the questionnaire. Our analyses confirm that no modifications to the item set are needed to enhance the scale’s reliability and consistency in the Hungarian version. The HLS19-VAC instrument has a 1-factor structure based on the PCA, which is also supported by Rasch analysis carried out on the HLS19 data.12,20 We observed a moderate positive correlation between GHL and VHL. Since the idea of VHL has flourished within the concept of GHL, the 2 constructs reveal partial overlap. Our findings suggest that GHL is an important foundation for VHL, particularly in vulnerable groups such as older adults and those with lower educational attainment.
The Hungarian VHL level was 82.4 on a scale from 0 to 100. Our result is not directly comparable with previous Hungarian results from 2015 and 2017, because the content and scoring of the VHL tool, as well as the data collection method, have evolved over time.10,21 In our survey “to judge which vaccine you or your family may need” was the most difficult task. This question was also among the most difficult tasks in the previous Hungarian surveys10,21 and in other HLS19 countries. 12 This may indicate that respondents have difficulty assessing which recommendations apply to them.
The determinants of VHL included lack of financial deprivation, social support, and education, highlighting the impact of socioeconomic status on individuals’ capacity to access, understand, and use vaccine-related information. These findings underscore the importance of targeted interventions for disadvantaged populations to improve vaccine literacy and public health outcomes.
Individuals with low VHL may struggle to find, interpret, and apply health information. A vaccine-literate environment, particularly within healthcare organizations, can help compensate for these limitations. 9 As healthcare professionals are trusted sources, their training should include vaccinology, communication, and strategies to identify and support people with low VHL. 22 Patient educators or health mediators can help healthcare professionals and clients communicate better. 23 To help people make vaccine-related decisions, multiple channels must provide trustworthy, commercially unbiased information. Also important is building and maintaining trust in public institution information channels. It is also essential to combat health and vaccine misinformation, monitor antivaxxer groups, and dismantle their arguments.
Community projects, which can be organized by health mediators and health promotion offices using the comprehensive health literacy intervention model, can boost social support. 24 Local events and projects can reach more people, identify leaders, and train them as non-professional community health workers. Health flyers could also be tailored to local vaccination culture and VHL levels.
Education from primary school onward can be a priority area for promoting health- and vaccine-related information. Developing GHL and VHL can be an equal part of the curriculum, while adults could participate in GHL and VHL activities as part of lifelong learning.
VHL was surveyed in 10 other countries besides Hungary in the HLS19. Hungary has the second highest VHL score after Portugal (M: 87.1, SD: 22.5).12,25 When comparing international results, it should be considered that both the method and timing of data collection may differ between countries participating in the HLS19. The COVID-19 pandemic, as well as the availability of vaccines and information about them may have influenced the survey results. 12
Vaccination policies vary widely in countries measuring VHL within the HLS19. Austria, Ireland, Germany, Norway, and Portugal have only recommended childhood vaccinations; Belgium has 1, the Czech Republic has 8, Italy and Slovenia have 10, Bulgaria has 11, and Hungary has 12 mandatory childhood vaccinations. 26 If a country has a high number of compulsory vaccinations, this may have an impact on individuals’ attitudes toward vaccination. The lack of choice may lead to individuals seeking less information about vaccination, which may also affect their VHL. In the HLS19, Bulgaria and Hungary have the highest number of mandatory vaccinations, but while Hungary has one of the highest levels of VHL, Bulgaria has the lowest. This indicates that factors beyond vaccination policy, such as public trust, education, and communication strategies, play important roles in shaping VHL.
Our findings highlight the necessity of comparing not only scores but also important contextual factors, such as policy, socioeconomic conditions, and public trust, on an international scale. Further studies may investigate the correlation between mandatory vaccination policies and VHL, just as VHL for mandatory and recommended vaccines, as well as evaluate the long-term impact of targeted interventions.
Strengths and Limitations
One of the strengths of our study is its large, representative sample. Our study was part of an international survey, so the results are internationally comparable and give a good picture of Hungarian VHL. Because our data was collected before Hungary’s COVID-19 vaccine rollout, this sensitive period may have influenced the study’s results. The first and second waves of the COVID-19 pandemic raised debate about vaccines. People may know more about vaccines, their risks and benefit, and how to navigate the health system. It may have a positive impact on VHL. Due to the cross-sectional nature of the study, causal relationships cannot be drawn. Even though we used a stratified sampling method and a weighting procedure to represent the Hungarian adult population in our study, selection bias attributable to non-responses cannot be excluded.
Conclusions
Our study shows that adult Hungarians have good level of VHL. Our study found that the HLS19-VAC instrument could be used to identify low VHL risk. The HLS19-VAC instrument should be combined with other vaccination attitude tools because high VHL does not guarantee vaccine uptake.
VHL determinants included lack of financial deprivation, social support, and education. Interventions targeting these determinants should improve both VHL and GHL, as education and social support are also determinants of GHL. 27
Footnotes
Acknowledgements
Authors’ NoteThe professional polling company responsible for data collection had no role in the analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. They were involved in sample drawing, data collection, and creation of the weighted database.The HLS19 instrument used in this research was developed within “HLS19 – the International Health Literacy Population Survey 2019–2021” of M-POHL. Further information about using the HLS19 instruments can be found here: ![]() .
.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki, and approved by the MEDICAL RESEARCH COUNCIL AND RESEARCH COMMITTEE, Hungary (IV/10181-3/2020/EKU – 2020).
Consent to Participate
Verbal informed consent was obtained from all subjects involved in the study.
Consent for Publication
Not applicable.
Author Contributions
Conceptualization, G.M. and É.B.; methodology, F.V.; formal analysis, F.V. and É.B.; data curation, F.V.; writing—original draft preparation, G.M.; writing—review and editing, F.V, R.Á. and É.B.; visualization, F.V.; supervision, R.Á.; funding acquisition, R.Á. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the Ministry of Human Capacities, Hungary (IV/956-4/2020/EKF) and by the Interior Ministry, Hungary (BM/10449-2/2023). This paper was supported by the János Bolyai Research Scholarship of the Hungarian Academy of Sciences (BO/00933/22/5). This project was also financed by the HUN-REN Research Network (TKCS-2021/32). RÁ also works as team member of the National Laboratory for Health Security Hungary (RRF-2.3.1-21-2022-00006) supported by the National Research, Development and Innovation Office (NKFIH).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors upon reasonable request. The data are not publicly available due to the participants of this study did not give written consent for their data to be shared publicly.