
Abstract
Background
Digital Health Literacy (DHL) is crucial in navigating digital health environments, yet few studies focus on older adults.
Objective
Explore the associations of digital health information and resource utilization, IT-related social support, and barriers/enhancers to digital health service usage with DHL among older adults.
Methods
A cross-sectional study was conducted from January 2022 to April 2023, involving 417 individuals over the age of 60 who were interviewed using an instrument for collecting data on DHL, social support, barriers/enhancers influencing use of digital health resources and personal/demographic data. Multi-regression models were used to examine the associations.
Results
Higher DHL scores were associated with daily use of digital interaction with healthcare (B = 0.28; 95% confidence interval [CI] = 0.07, 0.49; p = .01), daily use of other digital health resources (B = 0.22; 95% CI = 0.05, 0.40; p = .01), ease in finding assistance for online navigation (B = 0.27; 95% CI = 0.08, 0.45; p = .01), self-perceived digital proficiency (“usually very good at surfing the internet,” B = 0.35; 95% CI = 0.18, 0.52; p = .01), assistance from relatives/others in internet browsing (B = 0.20; 95% CI = 0.02, 0.37; p = .02), and having access to a computer, tablet, or smartphone (B = 0.29; 95% CI = 0.11, 0.47, p = .01). Conversely, barriers like “no access to a computer, tablet, or phone at all times” (B = −0.19; 95% CI = −0.34, −0.04; p = .01), “difficulty understanding online content” (B = −0.22; 95% CI = −0.36, −0.07; p = .01), and “believing to be too old for online services” (B = −0.18; 95% CI = −0.32, −0.03; p = .02) were associated with lower DHL scores.
Conclusions
Engagement with digital health platforms, including making online appointments and accessing personal health records, is associated with higher DHL levels. Support from relatives or others, a modifiable attribute, is also associated with elevated DHL among older adults.
Keywords
Introduction
In modern technology-driven healthcare, digital health services have emerged as transformative tools with the potential to improve health outcomes, accessibility, and overall well-being. 1 The utilization of these digital resources, however, is contingent upon individuals’ ability to navigate and comprehend the complex digital health services. The ability, known as digital health literacy (DHL), is particularly significant among elderly individuals when encountering challenges in adopting and effectively utilizing digital health services. 2 DHL is defined as the ability to search for, access, understand, appraise, validate, and apply online health information, and the ability to formulate and express questions, opinions, thoughts, or feelings when using digital devices. This concept relates strongly to the frequency with which people use different health resources from digital sources and resources such as online video consultations, digital personal health records, social media, and health-related apps.3,4 DHL differs depending on the individual’s situation and the environmental and social context. 5
While older people worldwide are increasingly using digital resources, 6 many digital health tools are still not designed to accommodate the needs of older people. 7 The availability of digital health information provides increasing opportunities to engage and empower individuals to participate in their healthcare, 8 yet this potential is realized only partially. 9 Noted social determinants of health are strongly associated with digital health skills and particularly of DHL among the older population, for example, race/ethnicity, 10 socioeconomic status, 11 and social salience. 12 While older adults are interested in integrating new technologies into their healthcare, 13 many of them experience social exclusion due to the perceived barriers to using digital resources. 14
The demographics in Taiwan have experienced a drastic shift into an aging population. In 2022, 17.56% of Taiwan’s population was aged 65 or older and to be nearly 28% by 2035. 15 Additionally, 94.2% of individuals aged 65 or over expected possible long-term care in Taiwan. 16 Digital healthcare can become a more important service and, therefore, DHL of the elderly is of utmost importance in Taiwan.
Elderly individuals are often confronted with barriers such as limited digital literacy, cognitive challenges, and concerns regarding privacy and security, which can impede access to and utilization of digital health services.17,18 Conversely, sources of support and enhancement, including IT-related social support and strategies to mitigate barriers, can serve as catalysts for the effective use of digital health resources among the elderly population.19,20
Taiwan has a robust information technology infrastructure and well-established comprehensive healthcare services that afford to test whether having the resources at the macro and meso level is associated with their use by elderly end users. 21 Based on the Internet Usage Survey in Taiwan, the percentage of individuals aged 55 and above utilizing smartphones increased significantly from 16.8% in 2011 to 67.9% in 2014. Additionally, a 2014 survey conducted by IEK revealed that around 45% of individuals aged 50 to 75 were familiar with internet usage, with 90% of them engaging in social media platforms like Line or Facebook. 22 Therefore, we conducted this study to examine the associations between digital health information utilization, IT-related social support, barriers and facilitators of digital health services with DHL among the elderly in Taiwan.
Materials and methods
Study design and sample
A cross-sectional study was conducted from January 2022 to April 2023, involving 505 eligible participants capable of responding to the questionnaire. Participants were recruited from five hospitals, including three affiliated with Taipei Medical University (Medical University Hospital, Wan Fang Hospital, Shuang Ho Hospital), and two affiliated with the Show Chwan Memorial Hospital, situated in the northern and central regions of the country, respectively. Elders who had cognitive impairment (e.g., dementia), illiterate, aphasia or visual impairment, or in emergency conditions, were not recruited. A simple random sampling was used to include the study participants from the list of seniors provided by each hospital. Trained research assistants contacted and invited the elders to participate in the survey during their visit to the hospital/center for regular check-ups, consultations, or health education programs. Face-to-face interview was administered after participants signed an informed consent form. Excluding data with missing values, responses of 417 individuals were included in the final analysis.
Measurements
Digital health literacy
DHL was assessed using the adjusted measure based on the European Digital Health Literacy Instrument (DHLI) within the context of the Health Literacy Survey (HLS)-19 study conducted by the Measuring Population and Organizational Health Literacy Network (M-POHL). 23 The survey questionnaire comprised 10 items, designed to assess four distinct subscales: Information Searching, Evaluating Reliability, Adding Self-Generated Content, and Determining Relevance. 24 Respondents were asked to rate their answers on a 4-point scale. The available response options ranged from “very easy” (4 points) to “rather easy” (3 points), “rather difficult” (2 points), and “very difficult” (1 point). Subsequently, mean scores for both the DHL index and its individual subscales were calculated. The mean scores were ranked from 1 to 4, with higher scores indicating better DHL and its subscales.
Barriers and enhancers of the use of digital healthcare services
A set of 13 items was used to assess both the barriers and enhancers associated with the utilization of digital healthcare services. Each item within these questionnaires employed a 5-point scale, wherein responses ranged from “very untrue for me” (1 point) to “very true for me” (5 points). Intermediate response options included “untrue for me” (2 points), “neutral” (3 points), and “true of me” (4 points). In the context of barriers, higher scores indicated a greater degree of difficulty in utilizing digital health services. Conversely, within the enhancers, higher scores reflected a higher level of proficiency in effectively utilizing digital health services.
IT-related social support
Two items were employed to assess IT-related social support. 25 The initial question queried, “When you need advice or help surfing the Internet, for example help in finding a particular site or service, how easy is it for you to find someone who will help you?.” This was evaluated on 5-point Likert scale, ranging from 1 (very difficult) to 5 (very easy), encompassing responses of difficult (2 points), neutral (3 points), and easy (4 points).26,27
The second question was “During the past 12 months, how often have you used the internet for finding others with health issues or concerns similar to the ones you are facing?” This was also gauged on a five-point Likert scale, spanning from “very rarely” (1 point), “rarely” (2 points), “sometimes” (3 points), “often” (4 points), to “very often” (5 points). A heightened score denoted greater IT-related support.
Use of digital health information and resources
Participants were asked about their utilization of various digital resources for obtaining health-related information, including “In a typical week, how many days do you use the following digital resources for getting health-related information?” The specified resources included: Website for getting health-related information; Social media including online forums for getting health-related information; A digital device related to health or health care; Health apps on your mobile phone, Digital interactions with your health system; Other digital resources for getting health-related information.
Responses were rated on a five-point scale, as follows: “Less than once per week” (1 point); “1–3 days per week” (2 points); “4–6 days per week” (3 points); “Once a day” (4 points); “More than once per day” (5 points). A higher score indicated a greater frequency of engaging with digital health information and resources. 2
Socio-demographics
The respondents’ demographic information was collected, including age (years), sex (male and female), marital status (single, married, or separate/divorce/widow), education attainment (lower secondary school or below, upper secondary school or post-secondary non-tertiary education, bachelors or higher), ability to pay for medication (very difficult or fairly difficult, and fairly easy or very easy), residence area (urban, suburban, or rural), time for travel to the nearest/preferred hospital (≤20 min, >20 min), number of people living in the same household (≤3 people, >3 people), and self-reported social-economic status (low, middle, high).
Statistical analysis
We evaluated the Internal consistency reliability by using Cronbach's alpha statistic, with acceptable values of alpha above 0.70. 28 Categorical variables were analyzed using frequency and percentage distributions, while continuous variables were examined using mean and standard deviation. To appropriately compare means, T-tests and one-way analysis of variance were applied as needed. Both unadjusted and adjusted models were employed in a linear regression analysis to determine variables associated with DHL and its subscales. In multivariate regression models, each item on these questionnaires was adjusted for socio-demographic variables, including age, gender, education, social status, marital status, medication payment, residence, number of people living in the same household, and duration of time needed to travel to the nearest/preferred hospital, due to the high correlation among the items (Supplementary). All statistical analyses were conducted using SPSS version 26.0 from IBM Corp, Armonk, NY, USA. The threshold for statistical significance was set at p < .05.
Results
Socio-demographic description of the sample
Of the 417 individuals, 82 (19.7%) were male, 334 (80.3%) were female, 347 (83.2%) were within 60–74 years, and 70 (16.8%) were 75–85 years old (Table 1). The mean score of DHL was 2.8 ± 0.6. Significant differences were observed in DHL across several variables, including: social status; use of digital health information and resources including: website, social media, digital devices, digital interaction with health system, other digital resources; IT-related social support, including: finding someone who will help in accessing a particular site or service, frequency of the internet use for finding others with health issues or concerns similar to the ones you are facing; and barriers and enhancers of use of digital health services, including: “I don’t have a computer, tablet or mobile phone available at all times, I find it difficult to understand what I read on the internet, I am too old to use online services, I have no time, I don’t have someone to help me navigate the digital system, I am usually very good at surfing the internet, my relatives/others help me surf the internet, and I have at my disposal a computer or a tablet or a smart phone” (p < .05).
Distribution of digital health literacy by patients’ characteristics (n = 417).

Note. DHL, digital health literacy; IT, Information Technology; SD, standard deviation.
Use of digital health information and resources, IT related-social support with digital health literacy using multivariate linear regression models
For the use of digital health information and resources, we have six items, as shown in Table 2. The Cronbach’s alpha value for these items is 0.87. The multiple linear regression test was performed in Table 2. The results show that the factors associated with higher DHL scores were “use of digital interaction with your healthcare once a day or more than once per day” l (unstandardized regression coefficient, B = 0.28; 95% CI = 0.07, 0.49; p =.01), “use of other digital resources for getting health-related information once a day or more than once per day” (B = 0.22; 95% CI = 0.05, 0.40; p = .01), and easy or very easy to find someone who will help you in finding a particular site or service (B = 0.27; 95% CI = 0.08, 0.45; p =.01).
Association of use of types of digital health information and resources, IT related-social support with digital health literacy and its subscales (n = 417).
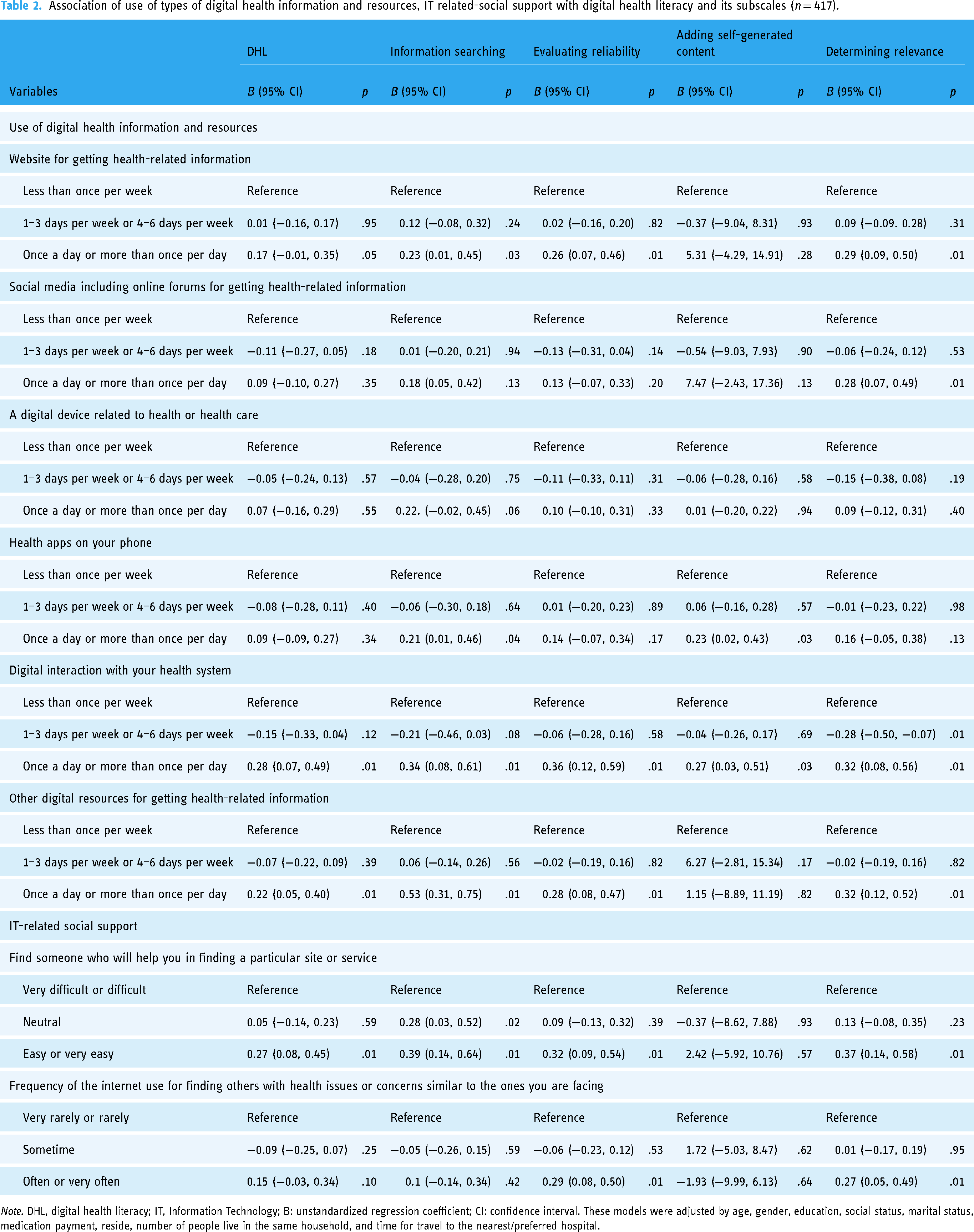
Note. DHL, digital health literacy; IT, Information Technology; B: unstandardized regression coefficient; CI: confidence interval. These models were adjusted by age, gender, education, social status, marital status, medication payment, reside, number of people live in the same household, and time for travel to the nearest/preferred hospital.
For information searching, the results show that factors associated with higher “information searching” scores were once a day or more than once per day using websites for getting health-related information (B = 0.23; 95% CI = 0.01, 0.45; p =.03), once a day or more than once per day used health apps on your phone (B = 0.21; 95% CI = 0.003, 0.46; p = .04), once a day or more than once per day digital interaction with your health system (B = 0.34; 95% CI = 0.08, 0.61; p = .01) and easy or very easy to find someone who will help you in finding a particular site or service (B = 0.39; 95% CI = 0.14, 0.64; p =.01).
For evaluating the reliability of the information, the results show that factors associated with higher scores were using websites once a day or more than once per day for getting health-related information (B = 0.26; 95% CI = 0.07, 0.46; p = .01), digital interaction with your health system once a day or more than once per day (B = 0.36; 95% CI = 0.12, 0.59; p = .01), easy or very easy to find someone who will help you in finding a particular site or service (B = 0.32; 95% CI = 0.09, 0.54; p = .01), especially, often or very often regarding “Frequency of the internet use for finding others with health issues or concerns similar to the ones you are facing” (B = 0.29; 95% CI = 0.08, 0.50; p = .01).
The results show that factors associated with higher adding self-generated content scores were using health apps on your phone once a day or more than once per day (B = 0.23; 95% CI = 0.02, 0.43; p = .03), and digital interaction with the health system once a day or more than once per day (B = 0.27; 95% CI = 0.03, 0.51; p = .03).
For determining relevance, the results show that factors associated with higher scores were using websites for getting health-related information once a day or more than once per day (B = 0.29; 95% CI = 0.09, 0.50; p = .01), and Social media including online forums for getting health-related information once a day or more than once per day (B = 0.28; 95% CI = 0.07, 0.49; p = .01), once a day or more than once per day Digital interaction with your health system (B = 0.32; 95% CI = 0.08, 0.56; p = .01), and easy or very easy to find someone who will help you in finding a particular site or service (B = 0.37; 95% CI = 0.14, 0.58; p = .01).
Barriers and enhancers of use of digital health services with digital health literacy and its subscales using multivariate linear regression models
For Barriers and Enhancers of Use of Digital Health Services, we have 13 items, as shown in Table 3. The Cronbach’s alpha value for these items is 0.819. In Table 3, the results show that the factors associated with higher DHL scores were true for me or very true for me I am usually very good at surfing the internet (B = 0.35; 95% CI = 0.18, 0.52; p = .01), true for me or very true for me for my relatives/others help me surf the internet (B = 0.20; 95% CI = 0.02, 0.37; p = .02), and true for me or very true for me for I have at my disposal a computer or a tablet or a smartphone (B = 0.29; 95% CI = 0.11, 0.47; p = .01). Conversely, neutral for I don’t have a computer, tablet or phone available at all times (B = −0.19; 95% CI = −0.34, −0.04; p = .01), neutral for I find it difficult to understand what I read on the internet (B = −0.22; 95% CI = −0.36, −0.07; p =0.01), neutral for I am too old to use online services (B = −0.18; 95% CI = −0.32, −0.03; p = .02), and neutral for I have no time (B = −0.20; 95% CI = −0.35, −0.06; p = .01) were associated with lower DHL scores.
Association of barriers and enhancers of use of digital health services with digital health literacy and its subscale (n = 417).

Note. DHL, digital health literacy; IT, Information Technology; B: unstandardized regression coefficient; CI: confidence interval. The models were adjusted by age, gender, education, social status, marital status, medication payment, reside, number of people live in the same household, and time for travel to the nearest/prefered hospital.
For information searching, the results show that the factors associated with higher “Information Searching” scores were true for me or very true for me for I have at my disposal a computer or a tablet or a smartphone (B = 0.29; 95% CI = 0.11, 0.47; p = .01). Conversely, neutral for I don’t have a computer, tablet or smartphone available at all times (B = −0.22; 95% CI = −0.41, −0.02; p = .03), “True for me or very true for me” for I find it difficult to understand what I read on the internet (B = −0.25; 95% CI = −0.49, −0.01; p = .04), neutral for “I am not good at manipulating the cellular devices or computer” (B = −0.22; 95% CI = −0.39, −0.03; p = 0.02), and neutral for “I don’t have someone to help me navigate the digital system” (B = −0.20; 95% CI = −0.40, −0.01; p = 0.04) were associated with lower information searching scores.
For evaluating reliability, the results show that the factors associated with higher “evaluating reliability” scores were true for me or very true for me I am usually very good at surfing the internet (B = 0.29; 95% CI = 0.07, 0.51; p = .01), true for me or very true for me I am usually very good at surfing the internet (B = 0.29; 95% CI = 0.09, 0.50; p = .01). Conversely, neutral for I don’t have a computer, tablet or phone available at all times (B = −0.23; 95% CI = −0.41,−0.05; p = 0.01), “True of me or very true of me” for I find it difficult to understand what I read on the internet (B = −0.29; 95% CI = −0.45, −0.12; p = .01), neutral for I am too old to use online services (B = −0.19; 95% CI = −0.37, −0.02; p = .03), neutral for I have no time (B = −0.19; 95% CI = −0.36, −0.01; p = .03) and neutral for “I don’t have someone to help me navigate the digital system” (B = −0.22; 95% CI = −0.39, −0.04; p = .02) were associated with lower evaluating reliability scores.
For Adding self-generated content, the results show that the factors associated with lower “adding self-generated content” scores were true for me or very true for me for my relatives/others help me surf the internet (B = −8.41; 95% CI = 0.02, 0.37; p = .02) Conversely, neutral for I don’t have someone to help me navigate the digital system (B = 7.16; 95% CI = 0.45, 13.87; p = .04), “True of me or very true of me” for I have bad or unstable internet connection (B = 8.51; 95% CI = 0.53, 16.49; p = .04), were associated with higher adding self-generated content scores.
For determine relevance, the results show that the factors associated with lower “determine relevance” scores were true for me or very true for me i am usually very good at surfing the internet (B = 0.45; 95% CI = 0.24, 0.65; p = 0.01), true for me or very true for me for my relatives/others help me surf the internet (B = 0.30; 95% CI = 0.09, 0.51; p = 0.01), and true for me or very true for me for I have at my disposal a computer or a tablet or a smartphone (B = 0.39; 95% CI = 0.17, 0.61; p = .01). Conversely, neutral for I don’t have a computer, tablet or phone available at all times (B = −0.23; 95% CI = −0.40,−0.05; p = .02), neutral for I find it difficult to understand what I read on the internet (B = −0.27; 95% CI = −0.43, −0.11; p = 0.01), neutral for I am too old to use online services (B = −0.19; 95% CI = −0.37, −0.02; p = .03), and neutral for I have no time (B = −0.27; 95% CI = −0.44, −0.09; p = .01) were associated with lower DHL scores.
Discussion
In this study, we found a clear correlation between individual engagement with digital health platforms, namely making online appointments, accessing personal health records, and utilizing online consultation services with their higher levels of DHL. Additionally, those individuals who reported having easy access to assistance when navigating online platforms, and specifically mentioned receiving help from relatives or others to browse the internet, exhibited elevated levels of DHL. Conversely, participants who reported a lack of support in navigating digital systems were shown to have comparatively lower DHL scores. Notably, individuals who lacked consistent access to digital devices such as computers, tablets, or phones, and those who expressed challenges in comprehending online content, tended to exhibit lower DHL. Furthermore, individuals who demonstrated proficiency in internet usage and possessed personal access to devices like computers, tablets, or smartphones consistently demonstrated higher DHL scores. These findings collectively underscore the importance of digital interactions, accessibility, external support, and individual comfort with technology in influencing individuals’ DHL.
Among socio-demographic factors, DHL was dependent on reported social status. However, DHL was not dependent on education and, payment ability a measure of financial deprivation. According to Estrela, et al., higher education, income, and social support are associated to higher DHL, specifically a significant association of age on the eHealth literacy scale (eHEALS) scores among older adults was observed.2,29,30 In Taiwan, widespread internet access appears to mitigate challenges related to the education level, financial capacity, and residential regions of elderly individuals. 22 In our study, a significant majority (83.2%) of individuals aged 60 to 74 were categorized as “younger old.” 31 This skewed age distribution among the participants could potentially explain why age does not appear to have a significant effect on DHL. Additionally, older people with better social conditions and higher education are more likely to accept digital technology to manage their health. 32 Hence, payment ability does not exert a significant influence on DHL, whereas social status emerges as a pivotal factor affecting DHL among the elderly in Taiwan.
Regarding use of digital health information and resources, individuals often interact with digital health systems such as: making online appointments, online consultations access to personal health records, electronic delivery/transmission of medical tests, digital communication with a provider and digital resources, and other digital resources for getting health-related information without website, digital devices, social media, health apps had higher DHL, compared with individuals who interact less than once per week. However, when analyzing the results from the subscales of DHL, we observed that individuals who engaged with websites exhibited higher skills in information searching, evaluating reliability, and determining relevance. Similarly, individuals who engaged with social media showed an increase in determining relevance skills. Moreover, individuals who used health apps tended to demonstrate higher information-searching skills and a greater ability to add self-generated content. In the current era, these areas of the media environment are expanding to include podcasts, emails, online consultations, etc. In addition to these offerings, the field of virtualized media communication has newly emerged with health-tracking apps, computer games, and gamification apps. 33 As the field of artificial intelligence (AI) also continues to grow, including digital chatbots and apps that act without human assistance, 31 individuals will have more opportunities to be exposed to these resources. Based on our findings, older individuals tend to place more trust in health information found on websites when compared to social media platforms, regarding information searching and evaluating reliability field. This observation aligns with AlMuammar's research, 34 which similarly found that medical websites were the primary source of health information, followed closely by consultations with physicians. Websites often belong to reputable organizations, institutions, or healthcare providers, which can lend credibility to the information they present. Social media, on the other hand, can be more decentralized, making it difficult to determine the source’s reliability. Besides, websites are usually curated by professionals and experts, ensuring the accuracy and reliability of the content. In contrast, social media content can be generated by individuals with varying levels of expertise and may not undergo the same level of scrutiny. Social media platforms can host a wide range of content, including advertisements, personal opinions, and misinformation. The older public may be cautious about trusting health-related information on social media due to concerns about biased or misleading content. Therefore, the government needs to promote validated and evidence-based health information on the website and other sources, to accommodate diverse DHL skills. 35
Besides, the individuals for whom it is easy to find someone to help find information had higher DHL. This is because having access to knowledgeable and helpful individuals makes it easier for someone to ask questions, seek guidance, and learn about digital health tools and information. When people can turn to others for assistance, they feel more empowered to explore and engage with digital health resources, leading to a higher level of DHL. Essentially, the presence of a supportive network helps bridge the knowledge and skill gap, making it easier for individuals to understand and effectively utilize digital health technologies. The support from social ties was also mentioned in previous studies,36,37,38 through social ties not only increase knowledge but also change the actions of individuals in some diseases, such as: social ties may encourage some to stop smoking, they may encourage others to take up the practice 38 or grow obese together. 39 This is the basis for a future study among people in Taiwan throughout the life-course.
When considering the barriers to using digital health services it is important to note that the absence of electronic devices like computers, smartphones, and tablets has a detrimental impact on DHL. Without access to these devices, individuals face limitations in engaging with digital health resources, platforms, and information. These devices play a crucial role in developing DHL skills and facilitating access and interaction with a variety of digital health tools, applications, and websites. 40 Besides, when analyzing subscales of DHL, we also found that individuals who lack manipulating cellular devices or computer skills had lower searching information skills. Regular usage of digital devices offers a hands-on experience with technology, fostering a sense of familiarity and comfort. Not having access to these devices can hinder the development of fundamental digital skills necessary for effectively navigating health-related information online. Moreover, electronic devices serve as a gateway to staying well-informed about health-related news, updates, and guidelines available through diverse online sources. The absence of these devices may result in individuals missing out on valuable information that could contribute to enhancing their health knowledge and thus their health behavior, health outcomes and well-being. Furthermore, digital devices enable direct communication with healthcare professionals and peers, affording individuals the opportunity to pose questions, share personal experiences, and receive supportive guidance. The lack of access to such devices restricts the potential for online interactions related to health matters. Regular utilization of digital devices also contributes to overall digital literacy, encompassing skills such as web browsing, information retrieval, and critical evaluation of online content. Without exposure to these devices, individuals may encounter challenges in honing these essential skills. In essence, the absence of digital devices constitutes a significant barrier to accessing and effectively utilizing digital health resources. Access to these devices is pivotal for individuals to fully participate in the digital health landscape, empowering them to engage with health-related tools, information, and platforms to their utmost advantage. In contrast, the availability of an internet connection and the cost of internet usage were not found to be associated factors with HDL. Interestingly, while Taiwanese individuals tend to trust the information available on the internet, challenges arise in comprehending the content, posing barriers to achieving DHL. Simplifying online content for the elderly can play a crucial role in enhancing their understanding. Consequently, such efforts hold the potential to significantly improve DHL.
When it comes to internet content, individuals who find it challenging to understand the information tend to exhibit lower DHL, particularly in the areas of information searching, determining relevance, and evaluating reliability. Similarly, individuals who believe they are too old to use the internet also tend to have lower DHL. Therefore, it is crucial to ensure that online content is made easily understandable for older individuals.
Results of previous research may help shed a light on the findings of this study, with regard to the enhancing elements or barriers that we studied, such as easy-to-find people helping to search for information and lack of electronic devices. In the enhancer part, individual skills, electronic devices available, and the supporting from relatives play crucial roles in enhancing DHL. According to Norman and Skinner (2006), DHL is understood as a meta-competency consisting of six different sub-competencies including both analytical skills (literacy and numeracy, media literacy, information literacy) and context-specific skills (HL, computer literacy, scientific literacy). 41 In contrast to our definition of DHL, it has been noted that the concept of DHL encompasses the curative content of HL and extends it to include content that is prevention-oriented. 42 As a result, it becomes essential to organize intervention aimed at enhancing the understanding of how to effectively use digital devices, while also increasing access to these devices to enable the elderly to access the internet. In addition, the results of the study show that, individuals who receive assistance from relatives while navigating the internet tend to exhibit a negative impact on their ability to augment their self-generated content knowledge related to DHL. Therefore, providing training or resources for both individuals and their relatives on how to effectively search and evaluate online health information. This can empower them with the necessary skills, foster communication between healthcare professionals, individuals, and their relatives to ensure that everyone is on the same page when seeking health-related information online. By implementing these strategies, we can mitigate the negative impact of receiving assistance from relatives and, instead, turn it into a positive collaborative learning experience for all involved
The study has several limitations that should be acknowledged. First, a convenience sampling was employed, which may not fully represent the entire population of individuals aged 60 and above. Consequently, the findings may not be generalizable to all the individuals. Future research should concentrate no less on males than females and on older elderly 75 years old and above, who were underrepresented in this study. Second, while our sample size was moderate, it is important to note that our patient cohort was recruited from six hospitals, providing insights that are representative of a broader Taiwanese context. In the future, it is expected to enhance the scope of this study by enrolling a more extensive and diverse pool of individuals from a wider range of hospitals. Lastly, we found a high correlation among the items on these questionnaires, making it difficult to avoid intercorrelation between them. In the future, we will incorporate insights from each factor identified in the current study into new models.
Conclusions
This study revealed that individuals who frequently engaged with online sources and other information channels exhibited higher levels of digital health literacy (DHL). Conversely, a lack of digital devices had a negative association on DHL. Furthermore, individual proficiency and easy access to assistance from relatives were positively associated DHL. Considering these findings, it is advisable for the healthcare institutions to provide interventions aimed at educating elderly individuals about accessing DHL skills and to ensure the provision of digital devices for patients, and to make sure that diverse avenues of communication are available for older adults.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076241278926 - Supplemental material for Digital health literacy and its determinants among community dwelling elderly people in Taiwan
Supplemental material, sj-docx-1-dhj-10.1177_20552076241278926 for Digital health literacy and its determinants among community dwelling elderly people in Taiwan by Tu T. Tran, Peter WS Chang, Jenn-Ming Yang, Tso-Hsiao Chen, Chien-Tien Su, Diane Levin-Zamir and Orna Baron-Epel, Efrat Neter, Shih Feng Tsai, Bryan Lo, Tuyen V Duong, Shwu-Huey Yang in DIGITAL HEALTH
Footnotes
Acknowledgments
We would like to thank all of the healthcare providers and individuals who participated in this study from three affiliated with Taipei Medical University (Medical University Hospital, Wan Fang Hospital, Shuang Ho Hospital), and Chang Bing Show Chwan Memorial Hospital.
Contributorship
TTT and TVD conducted statistical analysis and draft the manuscript, PWSC, SFT, TVD, SHY involved in gaining ethical approval and collecting data. PWSC and SHY provided the supervisions. TTT, PWSC, DLZ, OBE, EN, SFT, BL, SHY involved in conceptualization, validation, revise the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. This work was supported by the National Science and Technology Council, Taiwan (MOST 111-2923-H-038-001-MY2).
Ethical approval
The study was approved by the Research Ethics Committee of Taipei Medical University (TMU-JIRB No. 202104123).
Guarantor
TVD and SHY.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.