
Abstract
Background:
Identifying circulating biomarkers that reflect cerebrovascular health may help clarify underlying mechanisms associated with brain damage. Serum albumin, a multifunctional protein with antioxidant, anti-inflammatory, and endothelial-stabilizing properties, could serve as a marker of cerebral integrity. We examined the association between albumin levels and neuroimaging markers of cerebral small vessel disease (cSVD) in a rural population of older adults.
Methods:
We conducted a cross-sectional study among community-dwelling individuals aged ≥ 60 years in rural Ecuador. Participants were invited to undergo brain MRI and laboratory testing as part of the study protocol. Inclusion was based on completion of these procedures and serum albumin levels within the physiological range of 3.0–5.0 g/dL. Logistic regression models were fitted to assess the association between serum albumin and cSVD markers, adjusting for demographics and cardiovascular health metrics .
Results:
Among 409 participants (mean age: 66.2 ± 6.1 years; 60% women), moderate-to-severe white matter hyperintensities (WMH) were present in 34% of participants. Serum albumin showed a non-linear inverse association with WMH. Only participants in the highest albumin quartile (4.42-5.0 g/dL) showed significantly lower odds of moderate-to-severe WMH (adjusted OR: 0.48; 95% CI: 0.25-0.93). No significant associations emerged with other cSVD markers.
Conclusion:
Higher physiological albumin levels were associated with a lower burden of WMH, consistent with a threshold-dependent protective effect on the cerebral microvasculature. These findings support serum albumin as a candidate biomarker of brain health in aging populations. Albumin may capture systemic processes – such as endothelial integrity and vascular inflammation – that contribute to cSVD. Its accessibility and affordability underscore its potential utility in community-based aging research and population-level screening.
Keywords
Introduction
Cerebral small vessel disease (cSVD) is a leading cause of stroke, cognitive impairment, and functional decline worldwide. 1 Its burden is particularly high in older adults, and recognition is often delayed in rural communities where access to MRI is restricted.2-4 Identifying accessible biomarkers that reflect brain health and microvascular integrity could improve early risk stratification and inform preventive strategies.
Pathogenesis of cSVD is closely related to endothelial dysfunction, blood–brain barrier disruption, and chronic low-grade inflammation. 5 Circulating proteins that influence these pathways may therefore provide insights into disease expression. Serum albumin, traditionally viewed as a nutritional marker, also has potent antioxidative, anti-inflammatory, and endothelial-stabilizing properties. By binding free radicals, maintaining plasma oncotic pressure, and preserving the endothelial glycocalyx, albumin helps regulate vascular permeability and microcirculatory function.6-8 It has been suggested that low albumin levels may be associated with impaired endothelial function, higher vascular risk, and greater burden of neuroimaging abnormalities. 9
A previous study reported an inverse association between serum albumin levels and the severity of white matter hyperintensities (WMH) of presumed vascular origin, a hallmark feature of cSVD, suggesting that lower serum albumin levels may reflect greater disease expression. 10 However, evidence remains limited and warrants further confirmation through independent investigations. Moreover, it is unknown whether the relationship is linear across the physiological range of albumin concentrations or whether a threshold effect is present.
Recent population-based studies have reported associations between serum albumin and neurovascular outcomes, including stroke severity, functional impairment, and long-term mortality.11-13 For example, hypoalbuminemia has been linked to increased risk of poor outcomes after ischemic stroke, while optimal albumin levels appear to confer vascular protection. However, most existing studies have focused on acute stroke populations or mortality outcomes, with limited data on albumin’s relationship to neuroimaging markers of cerebral small vessel disease in community-dwelling older adults.
To address these gaps, we investigated the association between serum albumin levels and neuroimaging markers of cSVD in a homogeneous cohort of community-dwelling older adults in rural Ecuador. This population, characterized by Amerindian ancestry, traditional dietary habits, and limited exposure to urban cardiovascular risk factors, offers a unique opportunity to explore the role of systemic biomarkers in brain aging and microvascular integrity while minimizing heterogeneity. We hypothesized that higher albumin levels would be associated with reduced WMH burden, reflecting preserved cerebral microvascular health and broader brain resilience.
Methods
Study Population
This study was conducted in community-dwellers aged ≥ 60 years residing in 3 neighboring rural villages located in coastal Ecuador. Residents of these villages share ethnicity (Amerindian ancestry), low levels of education, have similar living conditions, and exhibit comparable cardiovascular health status. 14 These consistencies minimize the possibility of disparities in assessing the investigated variables during the conduction of population studies.
Study Design
Of the 590 community-dwelling adults aged ≥ 60 years identified through door-to-door surveys and enrolled in a well-established population-based cohort, 409 (69%) participated in this cross-sectional study, in which brain MRI and laboratory assessments were conducted within a maximum interval of 3 months. Based on the results of a panel of biochemical tests and radiological exams, along with the results of interviews and procedures previously conducted on these individuals, we excluded those who had chronic obstructive pulmonary disease, advanced liver disease, chronic renal failure, cancer, immunodeficiency, autoimmune diseases, hematological disorders, or acute infections. Likewise, we excluded individuals with serum albumin levels outside a predefined range (between 3.0 and 5.0 g/dL). This range was selected to ensure a representative sample while minimizing the exclusions of individuals with borderline serum albumin levels (3.0-3.4 g/dL) that do not necessarily indicate pathology. Unadjusted and multivariate logistic regression models were fitted to assess the association between serum albumin levels and the most relevant neuroimaging markers of cSVD. This research was conducted following the ethical principles of the Declaration of Helsinki. Written informed consent was obtained from all participants, and the study was approved by an internationally accredited Ethics Committee.
Independent Variable
Serum albumin was treated as the exposure. Blood samples were drawn and centrifuged on the field and then transported on ice to the laboratory of our Institution for further processing. Serum albumin measurements were conducted with a COBAS® c 501 Automatic Analyzer (Roche Diagnostics, Mannheim, Germany) and reported in g/dL.
Dependent Variables
Neuroimaging markers of cSVD were assessed using unenhanced brain MRIs, with a 1.5 T MRI system (Phillips Medical Systems, Eindhoven, The Netherlands) that included multi-slice turbo spin echo T1-weighted, fluid attenuated inversion recovery (FLAIR), T2-weighted, and gradient-echo sequences in the axial plane. White matter hyperintensities (WMH) of presumed vascular origin were defined as hyperintense lesions on T2-weighted images that remained bright on FLAIR (without cavitation) and were graded according to the modified Fazekas scale. 15 In accordance with this widely used visual rating scale, WMH were considered moderate-to-severe when periventricular WMH extended into the deep white matter or when deep WMH became confluent or semi-confluent. Cerebral microbleeds were identified as small (≤10 mm) round areas of signal void with blooming, as seen on gradient-echo sequences and rated according to the microbleed anatomical rating scale. 16 Lacunes of presumed vascular origin were defined as fluid-filled cavities measuring 3 to 15 mm in diameter located in the territory of perforating arterioles. 17 Enlarged basal ganglia-perivascular spaces were defined as small, sharply-delineated spaces of CSF intensity on T2-weighted images that followed the course of perforating arterioles; these lesions were graded on a scale from 0 to 4, and considered moderate-to-severe if >10 lesions were seen on one side of the brain. 18 MRIs were reviewed by 2 independent investigators blinded to clinical and laboratory data. Kappa coefficients for inter-rater agreement ranged from very good to excellent, with discrepancies resolved with the aid of an external neuroradiologist.
Covariates Investigated
Age, sex, and traditional cardiovascular risk factors were considered relevant confounders. Demographics were assessed by self-report, while cardiovascular risk factors were evaluated using the Life’s Simple 7 construct of the American Heart Association (AHA), which includes 7 health metrics categorized as poor as follows: (1) smoking status: current or quit < 1 year; (2) body mass index: ≥30 kg/m2; (3) no moderate or intense physical activity; (4) unhealthy diet: regular consumption of none or only 1 component of the suggested AHA healthy diet; (5) blood pressure: ≥140/ ≥ 90 mmHg; (6) fasting glucose: ≥126 mg/dL; and (7) total cholesterol blood levels: ≥240 mg/dL. 19
Statistical Analysis
Data analysis was carried out using STATA version 19 (College Station, TX, USA). In unadjusted analyses, continuous variables were compared using linear models and categorical variables by using the chi-square or Fisher exact test, as appropriate. Unadjusted and multivariate logistic regression models were fitted to assess the association between serum albumin levels (exposure) and the aforementioned neuroimaging markers of cSVD, which were treated as distinct dependent variables. Multivariate models were adjusted for demographics and traditional cardiovascular risk factors.
Results
The mean (±SD) age of 409 study participants was 66.2 ± 6.1 years (median age: 65 years) and 247 (60%) were women. CVH metrics in the poor range included: smoking status: 16 (4%); body mass index: 107 (26%); physical activity: 31 (8%); diet: 39 (10%); blood pressure: 160 (39%); fasting glucose: 106 (26%); and total cholesterol blood levels: 60 (15%). There were several differences in these characteristics across these 409 participants and the 181 excluded individuals (Table 1).
Differences in Clinical Characteristics Across Excluded Individuals and Included Participants (Univariate Analysis).
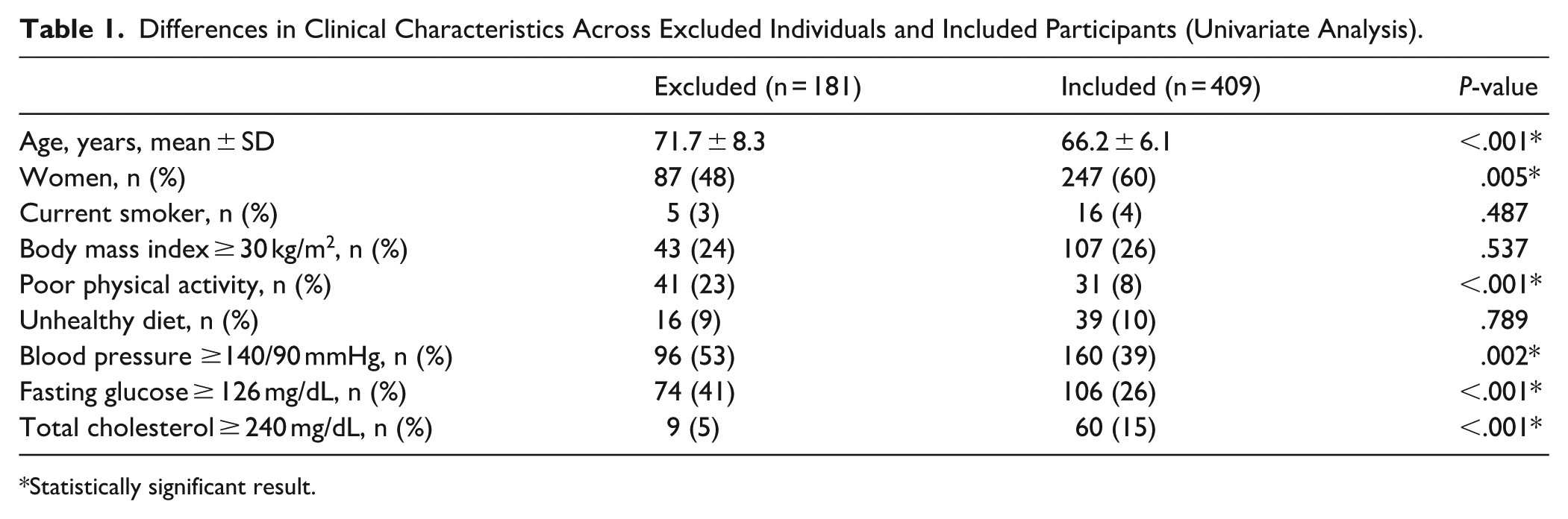
Statistically significant result.
Serum albumin levels had a mean value of 4.2 ± 0.3 g/dL (median 4.2 g/dL), with 105 participants allocated to the first (3.0-4.02 g/dL), 110 to the second (4.03-4.21 g/dL), 92 to the third (4.22-4.41 g/dL), and 102 to the fourth quartile (4.42-5.0 g/dL). Moderate-to-severe WMH were recognized in 141 (34%) participants, cerebral microbleeds in 53 (13%), lacunes in 42 (10%), and enlarged basal ganglia-perivascular spaces in 142 (35%).
Unadjusted logistic regression models showed a significant inverse association between serum albumin levels and the presence of moderate-to-severe WMH (OR: 0.53; 95% C.I.: 0.29-0.98); however, no significant associations were observed between albumin and other neuroimaging markers of cSVD (Table 2). Given the non-linearity observed in the albumin-WMH relationship (Supplemental File), we fitted a multivariate model categorizing serum albumin into quartiles, adjusting for demographics and cardiovascular health metrics. In this adjusted model, only individuals in the highest albumin quartile showed significantly reduced odds of moderate-to-severe WMH when compared with individuals of the first quartile (Table 3). Among all covariates, only increased age remained independently associated with WMH severity, as visualized in the forest plot depicted in the Supplemental File.
Unadjusted Logistic Regression Models Showing the Association Between Serum Albumin Levels (Independent Variable) and Each of the Neuroimaging Markers of Cerebral Small Vessel Disease and Moderate-to-Severe White Matter Hyperintensities of Presumed Vascular Origin.

Statistically significant result.
Multivariate Logistic Regression Model Showing the Association Between Serum Albumin Levels (Stratified in Quartiles) and the Presence of Moderate-to-Severe White Matter Hyperintensities of Presumed Vascular Origin, After Adjusting for Demographics and Cardiovascular Risk Factors.

Statistically significant result.
Discussion
In this population-based study of older adults in rural coastal Ecuador, we found that serum albumin levels in the upper physiological range were independently associated with lower odds of moderate-to-severe WMH. This association was non-linear, with a protective effect evident only among participants in the highest albumin quartile (4.42-5.0 g/dL). No significant associations were found with other neuroimaging markers of cSVD, such as cerebral microbleeds, lacunes, or enlarged basal ganglia perivascular spaces.
Findings of this study support the hypothesis that serum albumin levels, beyond serving as a marker of nutritional status, may be involved in processes that preserve brain health by maintaining endothelial integrity, modulating inflammation, and preserving blood-brain barrier function, mechanisms closely implicated in WMH development. 20
Our findings align with prior population-based studies that have identified non-linear associations between serum albumin and neurovascular outcomes.11-13 For instance, registry data from stroke cohorts have shown that both low and very high albumin levels may be associated with increased mortality, suggesting a U-shaped relationship. Similarly, studies in general populations have reported that albumin’s protective effects may emerge only above certain thresholds, consistent with our observation that only participants in the highest quartile experienced reduced WMH burden. These parallels strengthen the biological plausibility of albumin as a marker of cerebral resilience and underscore the need for longitudinal studies to clarify its predictive value.
Our results also expand upon prior evidence, which identified a similar inverse relationship between albumin and WMH volume in individuals with alcohol use disorders and HIV infection. 10 Results of that study, however, may not be generalizable to the population at large. By demonstrating this association in a low-income population with restricted access to advanced diagnostics, our study also strengthens the case for albumin as a potential low-cost marker for subclinical cerebral microvascular damage. This reinforces its relevance for community-based aging research, particularly in settings where neuroimaging is limited or unavailable.
The observed threshold effect, whereby only individuals in the highest albumin quartile experienced a less severe WMH burden, suggests a possible non-linear biological relationship. This is consistent with findings for other systemic biomarkers, such as C-reactive protein and homocysteine, where vascular risk is modulated only beyond certain thresholds.6,21 Albumin’s protective properties may become physiologically meaningful only at concentrations high enough to buffer oxidative and inflammatory insults. 9
The lack of significant associations between albumin and other cSVD markers might be due to several factors. First, WMH are considered the most directly linked to chronic endothelial dysfunction, whereas other lesions like lacunes or cerebral microbleeds may reflect more discrete or heterogeneous pathological mechanisms. Second, the relatively low prevalence of these other markers in our cohort may have reduced statistical power to detect subtle associations.
This study has several strengths, including a standardized neuroimaging protocol with high inter-rater reliability, careful exclusion of confounding systemic illnesses, and use of a culturally and environmentally homogeneous sample that enhances internal validity. We also employed a well-established cardiovascular health framework, facilitating robust adjustment for relevant vascular risk factors. However, serum albumin concentrations are influenced by age, nutrition, hydration status, and hepatic or renal function. We minimized confounding by excluding individuals with chronic systemic diseases or albumin levels outside the physiological range, yet residual variability cannot be excluded.
Other limitations should be acknowledged. The cross-sectional design limits causal inference, and unmeasured confounders, such as albumin-binding capacity, hepatic synthetic function, or underlying inflammatory load, could influence both albumin levels and cSVD expression. Although we restricted our sample to physiologically plausible albumin concentrations to avoid extremes of malnutrition or chronic illness, our results may not generalize beyond this range. Albumin’s anti-inflammatory properties are central to our hypothesized mechanism. However, we did not measure inflammatory biomarkers such as C-reactive protein or interleukin-6. This limits our ability to assess whether low-grade inflammation mediates the observed association between albumin and WMH burden. Additionally, our cohort may differ from urban or ethnically diverse populations in ways that influence the generalizability of the findings. For example, traditional dietary patterns, low migration, and reduced exposure to urban vascular risk factors may influence both albumin metabolism and cSVD expression. While these homogeneities enhanced internal validity in our study, replication of these findings in more diverse populations will be important to establish broader applicability.
In conclusion, our results indicate that serum albumin levels in the upper physiological range are associated with reduced WMH severity in older adults. This non-linear relationship suggests that serum albumin may serve as a biomarker of brain health, reflecting microvascular integrity through its antioxidative, anti-inflammatory, and endothelial-stabilizing properties. Serum albumin may serve as a clinically accessible indicator of cerebral resilience and vascular aging, particularly in settings where neuroimaging is limited. Its affordability and routine availability make it a promising candidate for population-level screening and hypothesis generation in aging research. Future longitudinal studies are warranted to determine whether serum albumin levels predict WMH progression or mediate cognitive decline, which would further clarify its role as a biomarker of cerebral resilience.
Supplemental Material
sj-pdf-1-jpc-10.1177_21501319251406848 – Supplemental material for Serum Albumin as a Biomarker of Brain and Microvascular Health in Older Adults: Implications for Community-Based Aging Research
Supplemental material, sj-pdf-1-jpc-10.1177_21501319251406848 for Serum Albumin as a Biomarker of Brain and Microvascular Health in Older Adults: Implications for Community-Based Aging Research by Oscar H. Del Brutto, Robertino M. Mera, Denisse A. Rumbea, Emilio E. Arias, Kleber Arriaga and Víctor J. Del Brutto in Journal of Primary Care & Community Health
Footnotes
Author Contributions
OHD: study design, manuscript drafting; RMM: statistical analysis, significant intellectual contribution to manuscript content; DAR: study coordinator, data collection and analysis; EEA: data collection; KA: interpretation of laboratory exams; VJD: study design, significant intellectual contribution to manuscript content.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Universidad Espíritu Santo – Ecuador. The sponsor had no role in the design of the study or in the decision to submit the manuscript for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are not publicly available due to their containing information that could compromise the privacy of research participants, but are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.