
Abstract
Cervical cancer mortality among Hispanic immigrant women remains disproportionately high in Tarrant County, Texas, despite national improvements. In this region, restrictive healthcare eligibility criteria and fragmented safety net systems limit access to preventive and life-saving care. A reactionary political environment further compounds these barriers. Drawing on the findings of a multi-year mixed-methods study and a subsequent academic-community partnership in Tarrant County, this article examines how governance decisions, fiscal priorities, and institutional policies shape immigrant health access. Using a political economy of health framework, we show how these structural conditions produce and sustain cervical cancer disparities. Qualitative research is essential for documenting how political and structural forces shape health outcomes. However, scholars working in restrictive policy environments within reactionary governance contexts face distinct methodological and ethical pressures. These include scrutiny of research framing, limitations on community collaboration, and risks associated with publicly naming policy-level drivers of inequity. Based on insights from conducting research in a politically contested setting, we identify strategies for maintaining rigor while minimizing harm to both research participants and community partners. These strategies include ethical community-engaged research practices, capacity-building efforts that strengthen local health infrastructures, and strategic framing techniques that communicate findings accurately without increasing political resistance. By pairing empirical analysis with pragmatic guidance for research in reactionary governance contexts, this article demonstrates how qualitative scholarship can contribute to public understanding, institutional reflection, and incremental system change even when direct policy reform is constrained. We ground these insights in cervical cancer survivorship among Hispanic immigrant women in Tarrant County to keep methodological guidance anchored in disease-specific realities.
Keywords
Background
Qualitative research methods are increasingly hailed as essential tools for exposing the macro-level forces that shape population health in racialized populations. 1 A growing number of studies draw on qualitative work to contextualize quantitative health disparity data, assess contributing factors, and advance recommendations for structural interventions to reduce health disparities among Black, Latine, and Indigenous communities through public policies or community mobilization.2-6 While these studies provide critical insights into structural inequities, they often overlook the methodological and ethical complexities researchers face when working in politically contested spaces and the strategies needed to navigate them. 7
This article presents a county-level analysis of Tarrant County, Texas, an urban county in the Dallas–Fort Worth (DFW) region with one of the highest cervical cancer mortality rates among Hispanic women in the United States. Drawing from a multi-year mixed-methods study and subsequent academic-community collaboration with local stakeholders, we use Tarrant County as a focal example for understanding how restrictive policy contexts, reactionary political environments, and institutional barriers intersect to shape immigrant health outcomes.
In reactionary political environments, researchers must consider how their work may be interpreted, framed, or challenged, particularly when studying policies that directly shape resource allocation, service eligibility, or institutional accountability for health equity. Scholars engaging in this work often confront both explicit and implicit constraints that affect data collection, dissemination, and the potential for policy influence. This necessitates a research approach that remains ethically grounded while strategically responding to these constraints. This analysis is also grounded in the concept of structural violence, which highlights how policy decisions, institutional practices, and social hierarchies collectively constrain access to preventive and specialty care and produce persistent inequities in health outcomes.8,9
Reactionary politics are characterized by beliefs and attitudes such as opposition to diversity, equity, and inclusion (DEI) initiatives, 10 resistance to expansion of the federal government, anti-immigrant sentiment, and racial resentment. 11 In politically conservative states such as Texas—where limited government ideology and decentralized healthcare governance shape local decision-making—state and institutional leaders often enact policies that constrain the adoption of evidence-based interventions aimed at reducing health disparities. For researchers conducting qualitative studies in such contexts, navigating these constraints requires a careful balance between scientific integrity, ethical responsibility, and political awareness.
Health disparities researchers working within reactionary political environments may experience increased scrutiny, politically motivated pushback, or even institutional barriers to funding and dissemination.12-14 This is particularly true for community-based scholars whose work amplifies marginalized voices and challenges dominant narratives. Because their work centers lived experiences and structural analyses of inequality, it may be perceived as politically threatening.
In response to these pressures, many scholars choose to engage in strategic methodological adaptation, shifting the scope and framing of their research activities to avoid controversy and maximize policy impact.15,16 These dynamics reflect a reactionary governance context in which restrictive policies and reactionary political environments reinforce each other. While such choices can reduce the risks for researchers and partners, they may also inadvertently minimize structural inequities or reframe systemic barriers as individual shortcomings. 17
This article seeks to bridge the research-to-action gap by examining how scholars can navigate restrictive policy environments within a reactionary governance context to produce methodologically rigorous and ethically sound data-driven insights that inform discussions on health inequities. The first section briefly describes a novel mixed-methods study conducted by an external research team (fRAP 2.0) aimed at promoting cervical cancer survivorship among Hispanic women. We synthesize qualitative insights from an academic-community partnership that point to policy barriers and anti-immigrant sentiment as key influences on elevated cervical cancer disparities. The second section draws on multiple sources through a political economy of health framework, which examines how economic and governance structures shape population health outcomes. 18 We draw on this lens to contextualize the federal, state, and county dynamics that shape access to healthcare for Hispanic immigrants in a “high-disparity” county. The final section advances methodological and ethical considerations for researchers conducting qualitative work in these environments, emphasizing approaches that ensure rigor, transparency, and ethical accountability while mitigating risk.
Cervical Cancer as an Indicator of Structural Inequities
Disparities in cervical cancer, a highly curable disease, reflect systemic inequities that disproportionately affect women from low-income and racially minoritized communities.19,20 The incidence of cervical cancer has declined over the last several decades, particularly in high-income countries with widespread access to the human papillomavirus (HPV) vaccine, Papanicolaou tests (Pap smears), and advanced treatment technologies (eg, chemotherapy, radiation, and targeted therapies). 21 Timely intervention is critical for mitigating the risk of adverse health outcomes, including mortality, following a diagnosis. Cervical screenings are only recommended every 3—5 years, and cervical cancer has a 91% survival rate when diagnosed and treated at an early stage. 22
Despite an overall downward trend, incidence rates of cervical cancer among Hispanic women in the United States (US) have long exceeded those of other groups.23,24 Elevated mortality rates are concentrated in southern and border regions—including Texas and other non-Medicaid-expansion states—where uninsured rates remain high and access to preventive and specialty care is limited.25,26 Although national screening and HPV vaccination rates improved following the Affordable Care Act (ACA), coverage gaps persist in states that did not expand Medicaid, sustaining inequities in early detection and treatment. 27
Most public health interventions addressing this disparity rely on culturally tailored materials and outreach strategies. These efforts frequently target socio-cultural barriers among Hispanic women, such as a lack of knowledge about cervical cancer screening, uncertainty about HPV vaccination, and cultural beliefs regarding gynecological exams. 23 However, many interventions fail to address the structural factors that constrain an individual’s ability to adopt recommended behaviors, such as a lack of health insurance, immigration-related fear, limited specialty care access, and fragmented public coverage systems.6,15,28-31 These structural challenges require research approaches that examine the policies and systems shaping healthcare access rather than focusing solely on individual-level interventions.
Summary of the ACS-Funded fRAP 2.0 Study
In 2018, with funding from the American Cancer Society (ACS), a team of scholars launched the Cervical Cancer Mortality Disparities in U.S. Hispanic Women Study, 32 which aimed to identify local policy levers for reducing cervical cancer disparities among US Hispanic women. The present authors were not involved in the design, data collection, or analysis of the fRAP 2.0 study. This multi-year study employed extensive data collection and stakeholder engagement using a focused Rapid Assessment Process (fRAP), an innovative mixed-methods approach designed to efficiently capture community and policy insights. This 3-step methodology identifies high-need geographic areas, applies qualitative inquiry to examine barriers and facilitators to cervical cancer survivorship, and cultivates community partnerships to drive evidence-informed discussions on multilevel policy targets. 33 We did not participate in the ACS-funded fRAP study; we synthesized its publicly available findings to contextualize cervical cancer disparities in Texas and contribute a new political-economy analysis of Tarrant County’s governance, policy environment, and implications for immigrant healthcare access. The policy analysis and methodological recommendations that follow are original contributions that have not appeared in prior peer-reviewed literature.
Following geospatial mapping of zip-code level incidence and mortality rates of all Texas counties, researchers conducted Community Assessment Profiles and selected Bexar County, Dallas County, and Tarrant County for further analysis. Despite similar population sizes, these counties exhibited different patterns of cervical cancer disparities (see Table 1). Consistent with state and national trends, Hispanic women in all 3 counties have higher disease incidence and mortality rates than non-Hispanic women. Although no remarkable differences in the relative incidence of cervical cancer existed, the relative mortality ratio of Hispanic women in Tarrant County (1.6x the state rate) is much higher than that of their Dallas County (1.1x) and Bexar County (1.0x) counterparts.
Cervical Cancer Disparities Among Hispanic and White Non-Hispanic Women in 3 Texas Counties With Different Disparity Profiles.
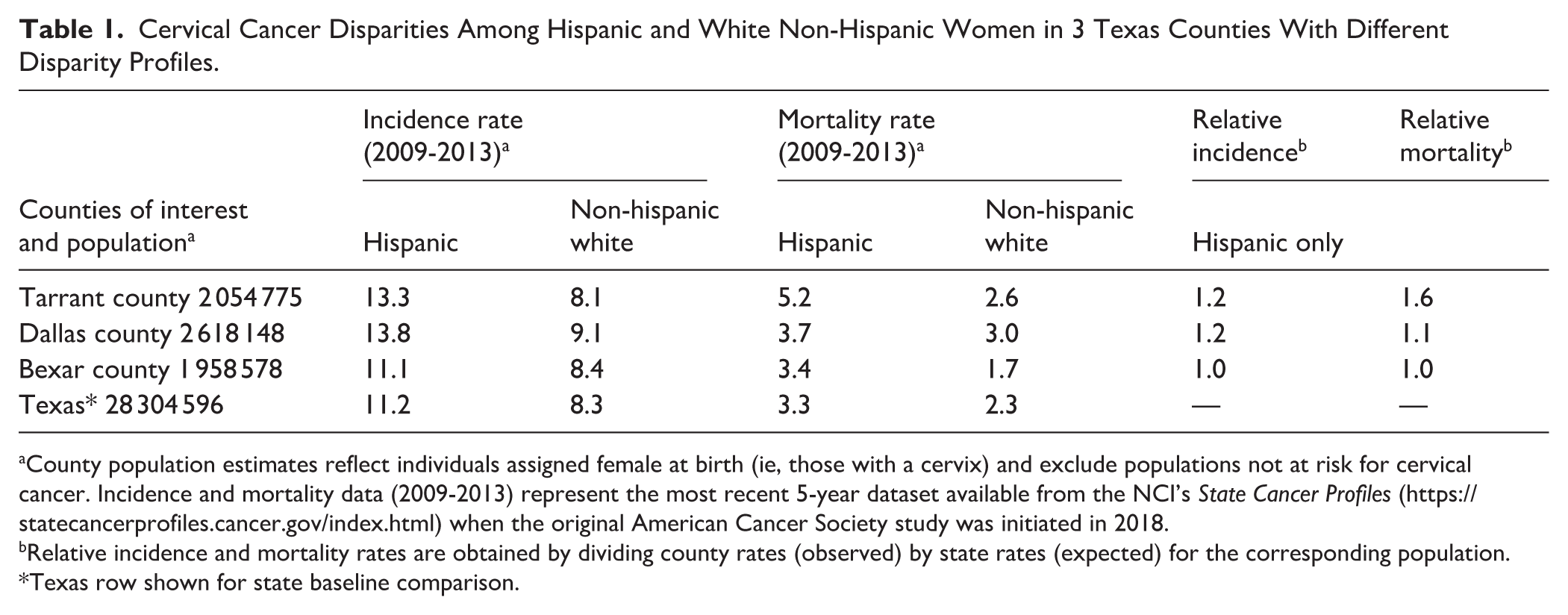
County population estimates reflect individuals assigned female at birth (ie, those with a cervix) and exclude populations not at risk for cervical cancer. Incidence and mortality data (2009-2013) represent the most recent 5-year dataset available from the NCI’s State Cancer Profiles (https://statecancerprofiles.cancer.gov/index.html) when the original American Cancer Society study was initiated in 2018.
Relative incidence and mortality rates are obtained by dividing county rates (observed) by state rates (expected) for the corresponding population.
Texas row shown for state baseline comparison.
Through qualitative interviews with key informants from the community, medical, and policy sectors, the fRAP process revealed multilevel factors influencing cervical cancer survivorship. 32 These findings, detailed in the published fRAP 2.0 study, document system-level drivers of disparity, including fragmented safety-net care, inconsistent screening outreach, and limited follow-up capacity among uninsured patients. Hispanic women in the “low-disparity” county (Bexar) experience greater community engagement in survivorship care and a healthcare system structured to be inclusive of undocumented immigrants. By contrast, Hispanic women in Tarrant County, the “high-disparity” county, navigate an environment with greater institutional constraints, where policies limiting access to safety-net healthcare programs create additional barriers to equitable cancer treatment. This case study illustrates the role of qualitative research in identifying policy gaps and informing targeted interventions. Together, these findings establish the contextual conditions that inform the original policy analysis presented in the sections that follow.
Advancing Local Policy Change Through Community Engagement
Our engagement with this work began only after the completion of the fRAP 2.0 study, when community stakeholders invited us to participate in dissemination discussions and subsequent task group activities. During the final phase of the Cervical Cancer Mortality Disparities in US Hispanic Women Study, the fRAP research team partnered with local stakeholders to implement actionable steps for local policy change. Rather than approaching policy change through direct advocacy, the team facilitated roundtable discussions to examine study findings, during which participants (including co-authors MN and JE, who were involved as local stakeholders rather than members of the fRAP research team) identified structural gaps, systemic delays, and ethical concerns as key factors exacerbating poor cervical cancer survivorship in Tarrant County (see Figure 1). Among the primary concerns raised were gaps in public awareness, prolonged administrative barriers in accessing treatment, ethical dilemmas, and pervasive avoidance of healthcare systems due to fear of immigration enforcement and financial constraints. These discussions led MN and JE to partner with HP in forming a multi-sector task group to enhance research dissemination and develop knowledge-shaping strategies that engage both policymakers and affected communities. Over 3 years, this initiative developed into an academic-community partnership that later incorporated MC, LR, KW, and JF. These academic-community partnership activities and their policy implications constitute part of the original contribution of the present article.

Priority issues uncovered through qualitative analysis and roundtable discussions with Tarrant County stakeholders.
Beginning in early 2021, this task group engaged in targeted dissemination efforts over 2 years. These initiatives sought to translate research findings into actionable insights, foster collaborative dialog among stakeholders, and establish partnerships to create a more informed and inclusive environment for immigrant healthcare access. Through multi-modal engagement strategies, the group:
Secured local media coverage to amplify research findings 34 ;
Convened a stakeholder-driven roundtable discussion with subject matter experts;
Hosted an online Teach-Out on immigrant health, 35 designed as a publicly accessible learning platform; and
Delivered presentations at multiple public forums, engaging elected officials, hospital leaders, health and social service providers, and other key stakeholders.
The Teach-Out featured an interview with the lead author of the ACS study, serving as an innovative model of community-academic dialog. This platform not only disseminated research findings but also provided an opportunity for reciprocal learning, advancing a deeper understanding of the institutional and systemic factors affecting immigrant women’s health outcomes. The statement below encapsulates the urgency of structural intervention and highlights the need for a research approach that moves beyond documentation to fostering inclusive, participatory engagement.
For 5—10 years, the medical system [and] the environment around a woman is failing her that she could have that virus progress to that point—over almost a decade—to the place where she’s going to end up with a cervical cancer diagnosis. I think that’s really key to imagine, and for people to sit with that and think about what those failings mean. . .across time and space.
35
Methods
This article presents an original policy analysis conducted by the authors. We synthesized county governance documents, hospital district eligibility policies, Texas statutes affecting immigrant access to care, fiscal records, political actions, local media reporting, and internal materials from a multi-sector task group that the authors helped convene in Tarrant County. These sources form the empirical basis for the analysis presented in the Results section. This article does not present a quantitative or mixed-methods evaluation of cervical cancer outcomes; rather, it offers a county-level political economy of health analysis designed to illuminate how structural and policy contexts shape survivorship patterns. We reviewed all materials using a political economy of health framework to examine how structural, fiscal, and ideological forces shape access to cervical cancer care for Hispanic immigrant women in Tarrant County. Analytical memoing and iterative coding guided theme development. Findings from the ACS-funded fRAP 2.0 study summarized in the Background section were used solely for contextual grounding and were not collected or analyzed by the present authors.
Results
Rather than modeling population-level outcomes, our analysis focused on identifying structural pathways through which local policy decisions and governance practices influence access to preventive and specialty care for Hispanic immigrant women. Building on the contextual insights summarized in the Background section, our policy analysis examined how structural and political conditions in Tarrant County shape immigrant access to cervical cancer care. Our analysis identified 3 interrelated structural pathways shaping immigrant cervical cancer survivorship in Tarrant County: fragmented access to preventive and specialty care, exclusionary local eligibility policies, and political dynamics that restrict investment in safety-net systems and academic partnerships. The political economy of health framework views health outcomes as the product of political and economic structures—such as labor markets, governance systems, and policy decisions—that determine how power and resources are distributed across a population.36-38 In contrast to behavioral or biomedical models, this approach interrogates how state policy, market priorities, and ideological currents shape both the distribution of disease and institutional responses to it. Within this framework, we use the term restrictive policy context to describe formal rules, eligibility criteria, and administrative structures that limit access to healthcare services for uninsured and immigrant populations. We distinguish this from the reactionary political environment, which refers to the broader ideological and partisan dynamics that generate resistance to equity-oriented reforms and shape how research findings and public health initiatives are received. Together, these conditions create a reactionary governance context, wherein political ideology and policy constraints reinforce one another to sustain structural barriers to care. This framing aligns with the political determinants of health, which emphasize how governance, power, and policy decisions collectively structure the conditions under which health inequities persist.
In this analysis, we operationalize the framework by examining how Tarrant County’s fiscal policies, governance structure, and institutional decision-making operate within a reactionary governance context to reproduce exclusionary access to care for uninsured immigrant women.
Fragmented Access to Care
The federal government plays a foundational role in funding cervical cancer care efforts for uninsured and underinsured women through partnerships between national and state agencies, including the Centers for Disease Control and Prevention (CDC) and the Texas Breast and Cervical Cancer Services (BCCS) program. The BCCS program allocates public funding to provide free or low-cost cancer screening and healthcare services for women with limited access to routine care; program eligibility and downstream treatment pathways vary by policy and funding source. However, significant gaps persist, as women without lawful authorization remain ineligible for Medicaid for Breast and Cervical Cancer (MBCC) coverage in Texas, creating a critical gap in treatment accessibility. 39
Enacted in 1996, the Personal Responsibility and Work Opportunity Reconciliation Act (PRWORA) established federal guidelines for incorporating immigration status into Medicaid and public benefit eligibility screenings. Under PRWORA, most public health benefits remain restricted to US citizens, with exceptions for refugees, asylees, and lawful permanent residents (LPRs) who meet specific criteria. 40 While PRWORA permitted states to allocate local funding to expand eligibility for other non-citizens, most states, including Texas, have maintained restrictive coverage policies, excluding undocumented individuals from Medicaid-funded cancer treatment.
Due to these coverage restrictions, many uninsured women delay care until they experience severe symptoms, such as uncontrolled vaginal bleeding. Under the Emergency Medical Treatment and Labor Act (EMTALA) of 1986, hospitals must screen and stabilize all patients presenting with emergency medical conditions, regardless of their ability to pay or immigration status. While EMTALA is a federal mandate limited to emergency stabilization (not definitive oncology care), downstream access and financing for non-emergent treatment are governed by state and local policies, 41 producing wide variation in continuity of cancer care. As a result, uninsured Texas women ineligible for Medicaid often remain unable to access publicly funded treatment, even if diagnosed in a hospital setting.
Federally Qualified Health Centers (FQHCs) serve as the primary—and often only—accessible source of preventive and primary healthcare for uninsured patients, regardless of immigration status. However, their capacity is limited to outpatient care, and they are not equipped to deliver specialized oncology treatments such as chemotherapy, radiation, or surgical interventions. As a result, even when FQHCs successfully identify cervical cancer through screening, uninsured women frequently encounter insurmountable barriers in accessing definitive care, creating critical gaps in the cancer care continuum. Some safety-net systems have even experimented with electronic consultation (eConsult) models to expand specialist input for uninsured patients, but these approaches still cannot replace comprehensive coverage of definitive oncologic care. 42
Coverage Disparities in Tarrant County
In Texas, county governments function as the payer of last resort for uninsured individuals through indigent healthcare programs and hospital districts. These entities vary widely in structure, funding, and eligibility criteria, creating a patchwork of access across the state.43-45 For example, while some jurisdictions levy dedicated taxes and administer broad coverage via a hospital district, others rely on minimal programs and disparate clinics. This leads to persistent fragmentation in access to preventive and specialty care for uninsured patients, particularly those with precarious or undocumented immigration status.6,15,30
Tarrant County provides a notable example of these disparities. In 2004, its public hospital district, John Peter Smith Health Network (JPS Health Network), implemented a policy that bars individuals without US citizenship or lawful permanent residency from receiving nonemergency financial assistance. 46 This policy, which remains in effect, creates a significant barrier to preventive care and lifesaving treatment for uninsured immigrant women. By contrast, neighboring Dallas County has implemented more inclusive policies, offering locally funded financial assistance to low-income residents regardless of immigration status. This inter-county discrepancy illustrates how, within a reactionary governance context, local governance decisions determine whether uninsured immigrants can receive critical medical care.
For example, in Tarrant County, an uninsured woman diagnosed with precancerous lesions through a community clinic would likely be referred to JPS Health Network but denied nonemergency financial assistance due to her immigration status. In contrast, a similarly situated patient in neighboring Dallas County could qualify for locally funded care through Parkland Health’s financial assistance program, enabling access to timely treatment. These divergent trajectories underscore how local governance decisions directly shape the continuum of care and long-term survivorship for immigrant women.
Reactionary Politics and Public Healthcare Access
Tarrant County, the third most populous county in Texas, is located within the DFW metroplex, a region that has experienced significant demographic shifts over the past 2 decades and rising demand for healthcare services. Fort Worth, its county seat, ranks as the 12th largest US city and remains one of the nation’s fastest-growing metropolitan areas. 47 As local population growth increases healthcare demands, public hospital systems must strategically respond to constraints characteristic of a reactionary political environment—shaping budget allocations, patient eligibility, and long-term investment in healthcare services. These demographic shifts, especially the rapid growth of racially and economically diverse communities, have heightened political tensions and helped create a reactionary policy environment influencing healthcare access.
Public health and healthcare leaders in Tarrant County and similar regions must navigate substantial political, social, and economic risks when addressing policy gaps in healthcare access. 48 Public hospitals, in particular, must balance fiscal constraints with the challenges of fragmented healthcare coverage, rapid demographic growth, and an increasingly competitive market. 49 Unlike privately owned healthcare systems, public hospitals are directly subject to public accountability, with funding decisions and policy direction often influenced by shifting political landscapes. This greater susceptibility to the reactionary political environment, in turn, affects service provision and resource allocation.
Tarrant County’s political landscape continues to shape its healthcare policies in distinct ways. While its political leadership has historically leaned Republican, recent elections have reflected a shift toward fiscal conservatism, which has reduced investment in public health. 50 This evolving political composition influences budgetary decisions regarding healthcare funding and hospital district policies. Compared to other urban hospital districts in Texas—such as those in Dallas, Travis, and Harris Counties—JPS Health Network operates with a moderate tax rate near the state median for hospital districts, according to comparative data compiled by Central Health. 51 However, in 2024, newly elected county officials voted along partisan lines to reduce the hospital district tax rate—the third decrease in 6 years, despite increasing demand for safety-net services. 52 This reduction not only limits hospital district funding but also curtails broader healthcare and social service initiatives.
Recent evidence indicates that political partisanship in local government policies exerts a greater influence than previously recognized, particularly in states with a commission form of government.53,54 Since Texas is heavily reliant on property taxes for state revenue, its local governments wield greater administrative authority than states with more diverse tax structures. 55 County governments, therefore, play a pivotal role in determining local healthcare funding and policy priorities. Texas counties are governed by 4 precinct-level commissioners and a County Judge who serves as the presiding officer (Tex. Const. Art. 5, § 18). These 5 elected officials exercise both legislative and executive powers while overseeing local boards and agencies. This includes control over public hospital district policies and financial assistance programs that impact low-income and uninsured populations (4 Tex. Health & Safety Code § 281.021).
Although Tarrant County lies more than 400 miles from the international border between the US and Mexico, its top law enforcement official has actively endorsed federal- and state-level policies intended to deter unauthorized migrants.56,57 Texas leaders have enacted a series of immigration policies with significant public health implications, heightening concerns about access to public services, including healthcare. Despite ongoing constitutional challenges, these policies have intensified contentious debates over local governance and immigrant access to essential services. 58
This fiscal conservatism extends beyond healthcare, affecting other social determinants of health. Tarrant County is home to Arlington, the largest US city without a public transit system. 59 Although local officials have widely debated this issue, voter-led initiatives to improve accessibility have largely failed, reinforcing barriers to healthcare access for uninsured and low-income residents.
Weakened Academic Agency
These same political dynamics also shape the academic conditions under which community health research is conducted. In regions like Tarrant County, community-based scholars contend with a restrictive policy environment that actively limits public health efforts framed around equity. In 2023, the Texas legislature advanced 2 new laws aimed at limiting institutional investment in diversity-related initiatives. SB 17 banned offices of diversity, equity, and inclusion (DEI) in public universities. 60 While SB 17 does not target scholarly activities or curricular content, a second law (SB 18) expanded the conditions under which tenured faculty can be dismissed, raising concerns about the erosion of research autonomy and state interference in academic governance.
University officials expressed concern about the impact of SB 17 and SB 18 on faculty retention, particularly for scholars from historically underrepresented communities and those whose research focuses on racial and ethnic minorities, immigrants, and LGBTQ+ populations. These policy shifts have contributed to an emerging trend in which faculty specializing in social justice-oriented research seek positions in institutions with stronger academic protections, leading to knowledge attrition in critical research areas. Highly trained and innovative scholars are relocating to institutions with stronger research protections and funding support, weakening the academic networks that sustain community-based public health research.
In 2025, additional legislation further intensified these constraints. Several new laws—such as SB 37 and companion measures taking effect September 1, 2025—expanded state oversight of faculty governance, imposed new restrictions on curriculum content, and increased compliance requirements for research collaborations. 61 These reforms have heightened institutional risk within a reactionary governance context and further discouraged university partnerships with community-based organizations and external research institutions.
These academic restrictions directly constrain frontline community work. When universities withdraw from partnerships or faculty are limited in conducting applied research, community-based organizations lose technical support for grant reporting, evaluation, and data analysis. Health departments and nonprofits that depend on academic collaborators for research design and outcome evaluation face longer project timelines and reduced access to credible evidence that can sustain or scale interventions. Public health service delivery is weakened when evidence generation slows or when trust networks between universities and communities are disrupted.
For researchers outside Texas, collaboration barriers have also grown. Institutional review boards and data-sharing offices at Texas universities now operate under state-level compliance policies that restrict external partnerships involving sensitive topics such as immigration, reproductive health, or racial equity. This limits the ability of out-of-state investigators to conduct or fund multi-site studies that include Texas populations—further isolating local health systems and reducing national understanding of region-specific disparities.
It is important to note that, even in states with more inclusive policies, translational research—defined here as scholarship that bridges scientific discovery and real-world application through policy, practice, or community partnerships—scholars still encounter institutional barriers to engaging in high-impact, policy-relevant research. Community-based health interventions are typically driven by shifting priorities of funding agencies. Similarly, researchers are evaluated and retained based on the quality and volume of their scholarship, rather than direct impact on policy, practice, or health outcomes. These structural constraints limit long-term engagement between academic institutions and the communities they serve, reducing opportunities for sustained health equity interventions.
Discussion: Implications for Qualitative Research in Restrictive Contexts
Building on publicly available fRAP findings and county-level dialogs, we show—through a political-economy-of-health lens—how reactionary contexts restrict institutional support, funding, and innovation, and we convert those insights into actionable strategies for researchers in similar settings. The insights presented here synthesize findings from the fRAP study’s documentation of local system barriers within our team’s original policy analysis, extending that work to highlight implications for qualitative research practice. While Tarrant County provides a concrete illustration of these dynamics, the conditions it represents—politicized governance, exclusionary eligibility criteria, and fragmented safety-net systems—are not unique to Texas. Similar patterns emerge in other regions where ideological opposition to government intervention limits investment in public health infrastructure. This section, therefore, shifts from analysis to action, offering strategies for scholars working in such environments to navigate institutional barriers, maintain ethical accountability, and advance health equity through community-engaged research methodologies.
Addressing Structural Barriers Through Research and Engagement
Scholars working in restrictive policy environments must develop approaches that balance scientific integrity with strategic engagement.3,62 This section applies the concept of structural violence to examine how restrictive policy contexts and reactionary political environments together limit access to healthcare and constrain the ability of academic institutions, health professionals, and community organizations to address disparities effectively.63,64 Structural violence refers to the systematic ways in which social structures harm or disadvantage individuals by restricting access to basic needs, such as healthcare. 8 In qualitative research, addressing structural violence requires a reflexive approach that recognizes how policy constraints shape both the research process and the lived experiences of affected populations. Scholars face unique challenges, particularly when institutional policies restrict public health research, limit external funding, or frame health equity work as politically sensitive. However, even within restrictive policy landscapes, rigorous, community-driven qualitative research can generate knowledge that informs public discourse, policy adaptation, and localized interventions.
Community Capacity Building
To reduce disparities in cancer care and other health outcomes, and reflecting insights identified in the ACS-funded fRAP study’s community assessments of Tarrant County, scholars can prioritize community capacity-building initiatives that reinforce local networks of care rather than focusing exclusively on policy change. In restrictive policy contexts, qualitative methods can serve as a mechanism for strengthening community networks, amplifying affected voices, and co-producing knowledge with community partners and local institutional collaborators. Community capacity refers to the relationships, resources, and structures within affected communities that can be mobilized to address their own health challenges. 65 While broad systemic reforms may be politically unattainable in some settings, capacity-building offers an alternative route to improving healthcare access through localized, adaptable solutions.
Some municipalities have implemented locally funded safety-net healthcare programs despite broader state or national restrictions. Adapting similar locally funded programs in Tarrant County—such as expanding eligibility criteria for county-supported treatment pathways—would directly address the care gaps identified in our analysis while remaining feasible within existing state constraints. Practical application of these recommendations is already evident in neighboring counties. For example, Dallas County’s inclusive financial assistance program enables uninsured residents—including immigrants—to access oncology services through the county hospital system. Adopting a similar locally funded treatment pathway in Tarrant County would directly address the gaps identified in our analysis, particularly for women diagnosed with cervical abnormalities at FQHCs who are currently unable to access specialty care. Such locally actionable changes illustrate the feasibility of implementing structural and methodological recommendations even in politically restrictive contexts.
Scholars can support such efforts by identifying evidence-informed, context-responsive approaches, conducting needs assessments, and facilitating knowledge exchange between community partners and local institutional collaborators. However, direct advocacy for policy shifts may not always be feasible. Instead, researchers can focus on strengthening local healthcare systems and fostering collaborative partnerships that address care gaps. Community capacity-building strategies should focus on:
Strengthening partnerships with nonprofit healthcare systems, grassroots coalitions, and social service agencies to mobilize local resources;
Supporting alternative funding models that reduce reliance on contested public programs, such as private philanthropy or hybrid public-private partnerships.
Facilitating cross-sector collaboration by engaging healthcare providers, legal advocates, and local leaders in identifying pragmatic solutions to care barriers; and
Developing research-practice partnerships that provide long-term engagement rather than focusing solely on short-term policy advocacy.
By framing these initiatives as capacity-building rather than direct policy reform, scholars can help foster sustainable solutions that are ethically sound and politically viable.
Strategic Framing
In politically restrictive settings, the framing of qualitative research findings is crucial to their reception and potential influence. Direct appeals for equity may face resistance, but reframing issues in terms of economic impact, workforce sustainability, or administrative efficiency can make them more palatable in ideologically divided environments.
Research on framing processes shows that strategic messaging can help mobilize support for social change by aligning with dominant narratives. 66 Recent public health communication research demonstrates that framing can significantly influence how audiences interpret and respond to messages about health equity, including generating resistance when messages conflict with political identity or worldview.67,68 Rather than positioning health equity solely as a moral imperative, scholars can frame discussions in terms of economic impact, workforce sustainability, and public safety. For example, emphasizing the burden placed on emergency rooms when preventive care is inaccessible shifts the conversation toward cost-effective healthcare planning rather than rights-based advocacy. This reframing underscores that health equity is not only a moral concern but a matter of fiscal responsibility and system sustainability, which can resonate more strongly in reactionary political environments. Similarly, highlighting provider burnout and workforce shortages frames the issue as one that affects health professionals and taxpayers, not just marginalized communities. 69 In qualitative research, the way findings are structured and communicated can determine their resonance with diverse audiences, including policymakers, healthcare administrators, and the public. Strategic framing techniques may include:
Presenting health disparities as an economic issue by demonstrating the long-term costs of preventable conditions;
Emphasizing how healthcare restrictions place undue burdens on frontline providers, leading to burnout and reduced workforce retention70,71; and
Framing solutions in terms of shared values, such as fiscal responsibility, healthcare efficiency, and public safety.
By adapting messaging to align with local priorities rather than directly confronting ideological resistance, scholars can create more opportunities for engagement while maintaining ethical and methodological integrity.
Minimizing Harm in Politicized Spaces
Even well-intended public health interventions can create unintended harm if they fail to account for the political and policy realities. In reactionary policy environments, programs that expand cancer screening without ensuring treatment access can lead to distress and distrust among communities who recognize the limits of available care. 29 Similarly, overly visible advocacy efforts can trigger backlash, endangering not only the scholars involved but also the local organizations they support. 72
A harm reduction approach can help mitigate these risks by prioritizing community-centered research practices that balance knowledge production with ethical responsibility. In this context, harm reduction applies both to researchers and community partners, emphasizing strategies that minimize institutional, political, and personal risks associated with conducting or participating in equity-oriented research in restrictive settings. Traditionally used in substance-use interventions, harm-reduction principles can also guide ethically responsive research practices aimed at reducing the negative consequences of policy constraints rather than requiring full systemic change. 73 For instance, instead of framing efforts solely as a response to systemic injustice, scholars might highlight their role in strengthening local health infrastructure, improving patient navigation, and supporting medical providers. Key harm reduction strategies for qualitative researchers working in restrictive political climates include:
Focusing on collaborative, participant-driven research approaches that enhance knowledge-sharing and minimize risk;
Ensuring that research dissemination prioritizes participant safety by reducing risks of surveillance, legal repercussions, or medical neglect; and
Collaborating with trusted local organizations to co-develop initiatives that align with existing community priorities.
These dilemmas often extend beyond research design into decisions about direct support for participants and community partners. In restrictive environments, scholars must balance institutional rules with moral obligations—such as whether to contribute financially to local initiatives, support mutual aid networks, or facilitate fundraising for community-based organizations. Global health scholarship offers valuable parallels, highlighting the ethical complexities of navigating reciprocity, power, and care in contexts where structural inequities limit formal advocacy channels.74,75 By acknowledging the constraints of the reactionary governance context, qualitative scholars can design methodologically rigorous studies that contribute to informed public discussions while maintaining ethical accountability.
Conclusion
This paper builds on findings from a community-engaged research study to examine the intersection of healthcare policy, political ideology, and health disparities within a reactionary governance context. Using cervical cancer survivorship among Hispanic immigrant women in Tarrant County, Texas, as a case study, we identify restrictive and exclusionary policies that systematically limit access to preventive care and treatment. Our analysis highlights how reactionary governance shapes public health policy, restricting access to safety-net healthcare services, limiting funding for safety-net programs, and reinforcing disparities through bureaucratic exclusions.
To bridge the research-to-action gap in reactionary political environments, we propose a multi-pronged approach that includes ethically grounded community capacity building, strategic framing, and harm reduction strategies. These methods provide alternative pathways for scholars and advocates working in restrictive political climates, where direct policy interventions may provoke resistance rather than drive change. By centering ethical research practices, scholars can contribute to evidence-based public discourse while maintaining methodological rigor and community accountability.
This paper complements a recently published companion study that empirically examined the political determinants of immigrant health—specifically, how reactionary governance structures shape immigrant health and cervical cancer disparities in Tarrant County, Texas. 76 Whereas that article identified the political and structural conditions shaping cervical cancer outcomes, the present manuscript extends that work by articulating methodological and ethical strategies for conducting rigorous, community-engaged research in politically restrictive settings. Together, these studies contribute to a broader framework for understanding how structural violence operates across the continuum from research design to policy implementation. By centering ethical accountability, reflexive methodology, and harm-reduction principles, this article provides an enduring roadmap for scholars seeking to advance health equity amid reactionary governance and institutional constraint.
Although cervical cancer incidence has declined globally, it remains a disproportionately burdensome disease for US Hispanic women, particularly in regions where restrictive policy environments create barriers to early detection and treatment. The disparities observed in Tarrant County underscore the broader consequences of exclusionary health policies that prioritize ideological governance over public health evidence. Despite 3 decades of inaction, Congress has failed to enact meaningful immigration or healthcare reform, leaving local jurisdictions to adopt policies that, in many cases, exacerbate inequities rather than mitigate them.
For scholars working in these environments, the expectation to directly influence policy may not always be feasible, and in some cases, may compromise professional standing. Academic researchers are not policymakers, nor are they advocates in the traditional sense—but they play a critical role in producing methodologically sound research that informs public debate, policy decisions, and institutional practices. In politically restrictive spaces, maintaining neutrality is often a necessary survival strategy—but neutrality does not require disengagement. By carefully navigating political constraints, scholars can ensure that their research serves as a tool for public knowledge and institutional learning.
Qualitative research provides avenues for documenting structural inequities, generating awareness, and facilitating dialog, even when direct policy change is not immediately attainable. While scholars in reactionary spaces may face limits on direct advocacy, their contributions can still shape discourse, influence institutional practices, and provide a foundation for incremental policy shifts and long-term structural change. The path forward is not without challenges, but neither is it devoid of possibilities. Through strategic engagement, interdisciplinary collaboration, and a commitment to ethically sound, evidence-based inquiry, scholars can help bridge the divide between research and action, ensuring that the voices and lived experiences of affected communities are neither ignored nor accepted as inevitable. Ultimately, this framework underscores that restrictive policy environments and reactionary political ideologies are not peripheral challenges but central determinants of health constituting the reactionary governance contexts through which inequities are maintained.
Footnotes
Acknowledgements
Many ideas expressed in this paper draw on decades of insights gained from interactions with community leaders and advocates committed to improving basic health care access in Tarrant County and beyond. We thank the following individuals for their role in establishing partnerships and lending expertise critical to the ideas in this paper: Jose Aguilar, Ann Sutherland, Richard Scotch, Amanda English, Amanda Arizola, Alexis Allison, and Willie Lubka. We are particularly grateful to Autumn Kieber-Emmons and her research team for providing the methodological foundations for the ideas developed in this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.