
Abstract
The purpose of this study was to gain consensus on Social Determinants of Health indicators among researchers actively publishing on SDH. We used a modified Delphi Method, an approach to gather expert opinions and gain consensus. We recruited participants in February 2024 via email from a PubMed search of researchers who had published on SDH in the last year. Participants (n = 22) completed 3 rounds of surveys. In each survey participants ranked the importance of each indicator. Fourteen participants completed all 3 surveys. Participants agreed to add indicators of Income (n = 14), Transportation (n = 14), Access to Quality Education (n = 13), Experiences of Racism and Discrimination (n = 12), Type of Healthcare Coverage (n = 11), Adverse Childhood Events (n = 9), Access to Higher Education (n = 8), Costs of Care (n = 8), and Provider Cultural and Linguistic Competency (n = 8). Participants agreed on significant modifications to an existing SDH framework, including adding more nuanced indicators on education, insurance coverage, transportation, and social context. However, the low response rate and over-representation of early career researchers indicate that further study is needed. Future research may also include a qualitative interview component to more fully understand participant rationale for responses. Our future goal is to develop a SDH instrument for use in population level public health surveillance based on the consensus of SDH indicators. To achieve this goal, additional research is needed to include a broader range of SDH researchers.
Introduction
With national priorities for achieving health equity in the United States, there is a need to address the social determinants of health (SDH) that underlie and contribute to inequities. Healthy People defines SDH as “the conditions in the environments where people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks.” 1 However, there is currently a lack of expert consensus on what constitutes the term SDH and wide variation in specific indicators. 2
The Healthy People SDH Framework is one way to visualize SDH, using indicators across 5 domains: Economic Stability, Education Access and Quality, Healthcare Access and Quality, Neighborhood and Built Environment, and Social and Community Context. 1 Originally developed as a part of Healthy People 2020, which launched in 2010, the framework represented a goal of addressing social environments that impact health. 3 The framework is currently a priority area of Healthy People 2030. 4 While Healthy People is considered one of the leading national frameworks for understanding SDH, the constructs are not operationalized as indicators for measurement.
In practice, there are patient-reported screeners for SDH, such as the PRAPARE Tool (PRAPARE, 2024), that are being implemented in clinical settings; however, measurement is at the individual level for clinical intervention. From a research perspective, the PhenX Toolkit provides protocols and instruments for measuring SDH at the individual and structural levels. 5 However, the measures provided are based on specific domains, exist in separate databases, and lack a comprehensive, framework-based resource. Furthermore, prior research has shown that the measurement of SDH in population-based databases is inconsistent across datasets and lacks comprehensive measurement. 6
As such, there is a need to revisit the Healthy People SDH Framework’s indicators and the relevance to the current research community for SDH. This study aimed to gain expert consensus on SDH indicators for use in public health surveillance. It is important to gain expert consensus before moving forward on the goal of creating measures for a SDH instrument for use in community surveys.
Methods
Overview
To reach a consensus on the SDH measures, we conducted a modified Delphi study.7,8 We intentionally included academic researchers as participants due to our goal of reaching consensus for future use in broad-scale population based surveys. We acknowledge that there are clinical uses for SDH including use of brief SDH clinical screeners, yet this was not the focus of our current work. We conducted 3 rounds of surveys with experts in the SDH field who were identified by recent publications related to SDH. The study was conducted online in 2024 using Qualtrics software (Qualtrics, 2025). This study was approved by the UMCIRB at East Carolina University.
Sample
We searched PubMed using the search term “social determinants of health” between October 2022 and October 2023 to identify current publications related to SDH. We chose this sampling method to identify participants actively publishing on SDH and selected PubMed as the largest database for health sciences literature. The corresponding authors and contact information for these articles were abstracted from the article (n = 184). In addition, we identified additional SDH experts through an informal web search of university and professional health organization websites (n = 31). After removing duplicates (n = 13), 203 people were identified to contact. A screening question was included to ask the participant if they indicated that SDH was a focus of their research. Individuals were contacted by email to invite them to participate in this study with 3 rounds of surveys. Each survey was open for a period of 2 weeks. Participants were notified of each survey round by email and were sent a reminder 1 week before the deadline. Participants received a gift card for their participation. Fourteen participants completed all 3 surveys.
Measures
Using the modified Delphi method, the surveys were iteratively adjusted to reflect information from the prior round of surveys to inform the subsequent rounds. The initial survey was developed based on the SDH indicators from the Healthy People Social Determinants of Health Framework. 1 This framework includes 5 domains, each of which contains 3 to 4 indicators. The key areas and their corresponding indicators are as follows: (1) Economic Stability (employment, food insecurity, housing instability, poverty), (2) Education Access and Quality (early childhood development and education, enrollment in higher education, high school graduation, language and literacy), (3) Healthcare Access and Quality (access to health services, access to primary care, health literacy), (4) Neighborhood and Built Environment (access to foods that support healthy dietary patterns, crime and violence, environmental conditions, quality of housing), (5) Social and Community Context (civic participation, discrimination, incarceration, social cohesion).
In Survey Round 1, participants were asked about each SDH indicator with the following question: “How important is it to include [indicator name] as an indicator for [SDH category]?” with response options of Very Important, Important, Neutral, Not Very Important, and Not At All Important. Participants were then asked if they had additional indicators to add for each SDH Category. Participants were not limited in the number of indicators they could agree to add. Additionally, there was no indication that survey respondents needed to reduce the number of indicators within a single domain.
Prior to Survey Round 2, the lead author edited the survey based on consensus of importance from Survey Round 1. Consensus was measured as 75% or higher participant agreement. The study team then added suggested indicators from Survey Round 1 to Survey Round 2. The same question structure was used for Survey Round 2.
Finally, for Survey Round 3, participants were asked a separate set of questions on final confirmation of whether to add or remove indicators. Participants were asked if they agreed with the removal of items from the final framework that did not reach at least 75% of participants rating an indicator as Important or Very Important. Similarly, participants were asked if they agreed with the addition of newly suggested indicators from previous surveys, that had at least 75% of participants rating the indicator as Important or Very Important, in the final framework. They were also asked to rank the importance of including these newly suggested indicators in the final framework.
Data Analysis
Descriptive frequencies and percentages were estimated for categorical variables in each survey round to inform the future iteration of the survey.
Results
Of the 203 potential participants contacted, 16.7% (n = 34) participated in Survey 1, 7.3% (n = 15) responded to Survey 2, and 6.9% (n = 14) responded to all 3 surveys. Among the participants in Survey Round 1, most had a PhD as their terminal degree and were employed at a university (Table 1). The top fields of study were medicine and public health. Participants were mostly at the assistant or associate professor level and most participants had at least 5 years of employment since completing their training.
Demographics of Participants in Survey Round 1 (n = 34).

In Survey Round 1 (n = 34), most Healthy People 2030 SDH Framework indicators were above the 75% threshold for inclusion except for food insecurity and civic participation indicators (Table 2). Thirty-three new indicators were proposed for the subsequent round.
Proportion Important/Very Important from Modified Delphi Surveys Rounds 1 and 2.
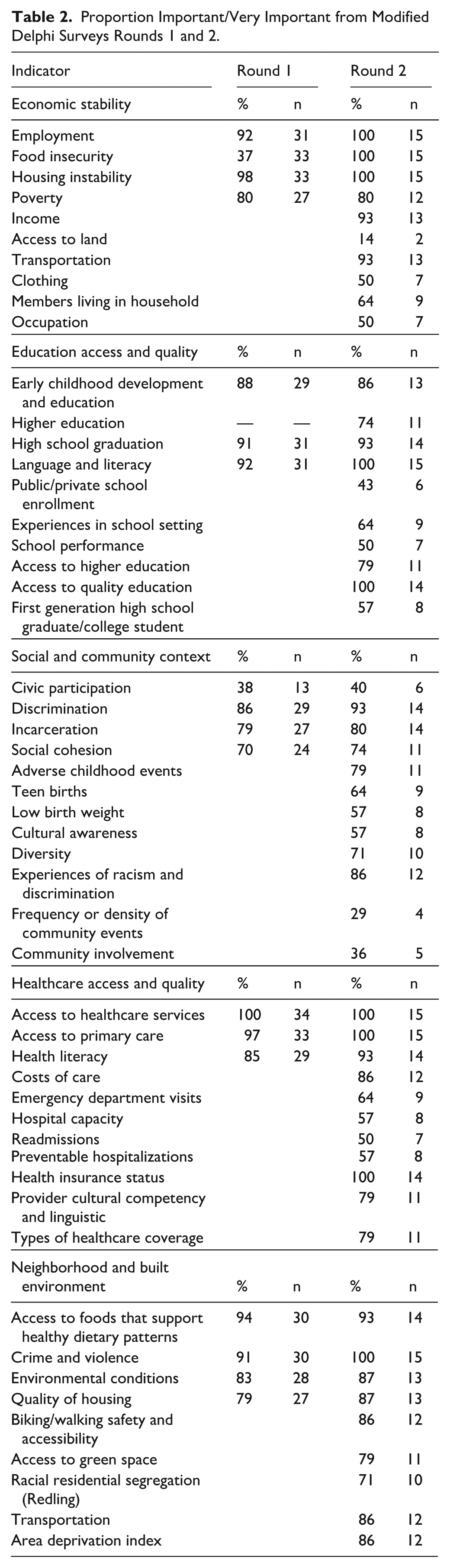
In Survey Round 2 (n = 15), participants were asked to re-rate the importance of indicators from the original Healthy People 2030 SDH Framework after viewing the responses of others from survey 1. In the second round, more indicators fell below the 75% threshold for inclusion. Participants were also asked to rate the importance of the new suggested indicators, of which 19 fell below the 75% threshold (Table 2).
In Survey Round 3 (n = 14), instead of re-rating indicators, participants were asked for a final confirmation of whether to remove indicators with less than 75% consensus on survey 2. Most participants recommended removal of Civic Participation (n = 9) and Social Cohesion (n = 8), but not Higher Education (n = 7). Participants had suggested new indicators on Survey 1 and rated those suggested new indicators on Survey 2. New indicators with greater than 75% consensus as very important or important in Survey 2 were considered for addition to the framework. In Survey 3, participants made a final decision of “agree to add,” “disagree with adding,” or “indifferent.” A majority of participants agreed to add indicators of Income (n = 14), Transportation (n = 14), Access to Quality Education (n = 13), Experiences of Racism and Discrimination (n = 12), Type of Healthcare Coverage (n = 11), Adverse Childhood Events (n = 9), Access to Higher Education (n = 8), Costs of Care (n = 8), and Provider Cultural and Linguistic Competency (n = 8) (Table 3). Participants responding to Survey Round 3 were supportive of having a framework with a combination of individual-level and system-level SDH indicators.
Revised SDH Framework.

Crossed out text indicates indicators removed from the original framework by consensus.
Italized text indicates consensus on additional indicators to framework.
Discussion
Results of our study indicate that participating SDH researchers agreed several modifications existing SDH framework. However, interpretation of results must take into consideration the low response and follow up rates and lack of representativeness of our sample. These constraints limit our ability to state that true consensus was reached. A large proportion of our participants indicated that they were early career, and high percentages of agreement among this sample may not reflect consensus in the larger field. However, this study contributes to the literature by presenting the views of a sample of researchers who study SDH and will be a part of the larger conversation about how it should be defined and measured in years to come. Overall, participants suggested more items to add to the framework, rather than to remove. Removed items include enrollment in higher education, civic participation, and social cohesion. Most items added were related to healthcare access and quality.
While the Healthy People Social Determinants of Health Framework was originally created to cover only population-level indicators, participants in our study often suggested adding individual level indicators. Other SDH frameworks such as the World Health Organization (WHO) Conceptual Framework for Action on the Social Determinants of Health does include individual level factors such as gender. 9 Further efforts are needed to decide whether a unified approach to measuring SDH should include both individual and population-level indicators.
It is interesting that there was consensus for income to be added as an indicator to the domain of economic stability, when poverty was not removed. As poverty status is measured by income, this inadvertently duplicates indicators. 10 This trend is also reflected in education access and quality. There was consensus to add Access to Quality Education as a new indicator, yet it is also the title of the domain itself. Participants opted to remove enrollment in higher education and add access to higher education. The emphasis on access rather than enrollment may bring attention to the financial barriers students often face when trying to access post-secondary education in the United States. 11 There is also an emphasis on quality in access across all levels of education as high school graduation rates can vary based on quality of education. 12
The authors found it surprising that Adverse Childhood Experiences (ACE) were selected to be added to the domain of Social and Community Context. ACEs are closely interrelated with a wide range of SDH, and ACE frameworks have historically existed separately from SDH frameworks.13-15 Including ACEs in a SDH framework may result in confounding when moving forward to operationalize measures. A recent study presented an Intersectional Nature of ACEs Framework that differentiates between ACEs that are consequences of social inequities and ACEs that are inflicted directly by a person. 15 Future research is needed to consider the implications of combining SDH and ACE frameworks in a way that can further contextualize environments that link to health outcomes.
The other indicator added to the domain of Social and Community Context, experiences of racism and discrimination, also implies individual experiences and potentially interpersonal aspects of racism. Discrimination was already an indicator in the domain and this addition may have been intended as a way to differentiate between interpersonal racism and structural racism. Structural racism is embedded within systems, for example, residential segregation and environmental injustice. 16 It is a common point of discussion among SDH researchers whether elements should be solely at the societal level or include elements at other levels of the social-ecological framework like individual or interpersonal. 17
The indicator added to the domain of Neighborhood and Built Environment, transportation, can impact all other domains including how people access healthcare, get to employment, school, or interact within the community.18,19 Transportation is acknowledged by the American Public Health Association as a community driver of health. 20
The domain of Healthcare Access and Quality included the most additions based on expert consensus. It is worth mentioning that researchers who study health and were identified via PubMed may inherently be more likely to value healthcare access over other social determinants. Cost of healthcare is a driving indicator of access that is separate from insurance status in that prices for healthcare are high in comparison with comparable countries. 21 Additional indicators, insurance status and type of insurance coverage were also added. It is unclear if insurance status and type of insurance status are both necessary as indicators, or if type of insurance status could be a future measurement of insurance status. Lastly, participants opted to add the indicator of provider cultural and linguistic competency. Barriers created by differences in spoken language and cultural norms can lead to poorer health outcomes.22,23 Culture as a concept is not commonly considered an SDH, but it has been proposed previously in a 2012 Roundtable on the Promotion of Health Equity and the Elimination of Health Disparities. 24 Previous work has also noted that cultural competence is not sufficient to reduce health inequities and that only addressing cultural differences can mask underlying differences in SDH rooted in racial discrimination 25
It is worth considering why expert consensus agreed to remove 3 of the indicators included in the original Healthy People 2030 Framework. The consensus to remove enrollment in higher education could reflect a shift to considering technical jobs rather than a college degree. 26 It may also indicate a need for more nuanced indicators of education, reflected by the decision to add indicators of access to higher education and access to quality education. The other 2 indicators removed from the framework, social cohesion and civic participation, are nebulous terms. Social cohesion can be difficult to define as a concept and it also overlaps with civic participation in some ways. 27
As previously stated, comprehensive SDH scales exist but are typically brief medical screeners for a clinical visit rather than comprehensive surveys. The difference between a population-based survey and a patient screener tool is that the survey is designed to be more in-depth and designed for broadscale public health research rather than part of a patient’s clinical plan of care. 28 For example, the Protocol for Responding to and Assessing Patient Assets, Risks, and Experiences (PRAPARE) tool is a 21-item questionnaire intended for use with patients in health centers. It can be incorporated into Electronic Health Records and is intended to be brief, due to the short nature of clinical encounters. PRAPARE was developed because there was no national standardized patient screening tool for SDH. Our work addresses a similar gap in that there is not a standardized set of indicators nor measures for use in large population-based surveys.
Another existing resource for SDH measures is the PhenX Toolkit, a web-based catalog of recommended measurement protocols. 5 Although measurement is the next step after identifying indicators, it is important to compare and differentiate our work and this existing resource. It was created by 2 workgroups funded by the US Department of Minority Health and Health Disparities to establish common data elements for health disparity research. The workgroups developed 10 Scope elements to guide identification of measures. 29 Many of these elements overlap with the indicators used in Healthy People SDH framework and our study. Because PhenX provides measurement tools rather than groups into indicators, it is possible that this tool can be used in conjunction with our findings for a future framework-based measurement tool. However, each protocol is found in a different publicly available database and each protocol is found in a different publicly available database and there are 42 individual protocols, making it difficult to group them into 1 comprehensive, population-based survey.
Our study is not without limitations. A disproportionate number of early career researchers responded, which may not represent the full field of SDH researchers nor senior experts with more depth of experience. We had a low response and follow up rate, initially of 16.7%, which dropped to 6.9% by the third survey. Previous research has indicated attrition as a large issue in Delphi studies. Participants who drop out may have dissenting views, creating a form of response bias. 30 Since we collected demographic information only in Survey 1, we were unable to determine if there were differences between participants who dropped out or continued to complete all 3 surveys. As such, we were also unable to determine the relationship between rater characteristics and selected indicators. Our recruitment strategy only contacted lead authors of manuscripts, which may have excluded other experts who participated in recently published SDH-focused articles. It became clear in our results, that we did not ask participants to focus only on population-level indicators, which was the purpose of the initial creation of the Healthy People SDH Framework. As such, many suggested individual level indicators that may be more appropriate for a separate framework. In addition, we have a small sample size. However, sample size requirements for modified Delphi studies such as ours, are not consistent in the literature. A review of Delphi studies in the health sciences found most studies having a sample size of between 8 and 20. 30 Manyara et al, 31 recommends 60 to 80 participants in multi-stakeholder Delphi surveys, yet a sample size of 20 to 30 rating all items per group may be sufficient for individual stakeholder groups such as clinicians.
It is important to acknowledge that we began with an existing framework, the publicly available Healthy People SDH Framework. 1 This framework was selected as it is a comprehensive, widely known framework, yet, it is not without limitations and was not originally created for use as a research-based measurement tool.
This study is unique in that previous Delphi studies examining SDH have not been framework-based and have had a clinical or medical education curriculum focus.32-34 Our study serves as a first step toward our future goal is to develop an SDH instrument for use in public health surveillance based on the consensus of SDH indicators. However, our results were not conclusive enough to create a measurement tool without further study. This study contributes to the literature as it highlights that there are a variety of opinions on what indicators make up SDH to have more consistency across SDH studies. Future research should include a broader range of experience in SDH researchers and tease out the differences when including individual and/or social-level factors in SDH frameworks. Future work should also include a qualitative interview component to understand participants’ rationale for responses more fully.
Footnotes
Ethical Considerations
This study was certified as exempt by the Institutional Review Board at East Carolina University (UMCIRB-23-002235).
Consent to Participate
All participants completed an online informed consent prior to beginning the study.
Author Contributions
Conceptualization: SBM, ET, and SG; Data Collection: SBM; Performed Analysis: SBM; Manuscript Writing: ET and SBM; Manuscript Review: ET, SBM, and SG.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the College of Health and Human Performance at East Carolina University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Participants did not consent to their responses being made available outside of the research team.