
Abstract
Introduction/Objectives:
Initiatives to identify and address health-related social needs (HRSN) are increasingly being implemented in clinical settings and have the potential to improve health outcomes. However, best practices for HRSN assessment and implementation are still needed. We gathered input to guide implementation of an HRSN initiative within adult primary care clinics at an academic health center.
Methods:
We conducted 6 focus groups to explore multiple perspectives (ie, clinicians, staff, patients, and community organization representatives) on optimal approaches to collecting HRSN data, processes for providing support to patients, and strategies for incorporating HRSN data into clinical workflows. Data were qualitatively analyzed to address the study’s research questions, resulting in themes stratified by each interest-holder group.
Results:
Themes centered on how the successful development and integration of HRSN initiatives require a multifaceted approach that includes dedicated staffing, standardized data collection, adequate resources for actionable support, streamlined EHR functionalities, and structured training for key personnel. HRSN initiatives must also consider local context, including the role of community organizations and their capacity to provide services that address social needs.
Conclusions:
Findings highlight perspectives from key interest-holders for shaping HRSN initiatives within primary care settings. We provide recommendations for developing organizational capabilities to effectively address HRSN.
Introduction
Health-related social needs (HRSN) are non-medical factors, such as food insecurity, housing instability, and lack of transportation, that create barriers to maintaining health and well-being. 1 There is growing recognition that HRSN put individuals at risk for worse health outcomes and increase health care utilization.1-8 For example, among adults with 2 diabetes, HRSN are associated with lower care quality, more complications, lower adherence to self-care, and worse clinical outcomes.7,9-12 Given the impact of HRSN on health outcomes, the National Academies of Science, Engineering, and Medicine, professional societies, and regulatory agencies recommend the routine collection of HRSN information in clinical practice and incorporation into electronic health records (EHRs).13-17 Greater awareness of patients’ HRSN facilitates whole-person care and an opportunity to potentially address unmet HRSN, which can help improve health outcomes, reduce health care utilization, overcome disparities, and affect policy.13,18-20
HRSN initiatives are increasingly being implemented in clinical settings; however, not all health systems have formal screening and referral processes,6,20-23 rates of uptake vary,6,19-21,24 and evidence on the effectiveness of HRSN initiatives is still emerging.19,20,22,25-27 Evidence to guide HRSN assessment and implementation is particularly needed in academic health centers,28-31 which account for nearly 25% of clinical services in the U.S. and serve large numbers of socially disadvantaged people. 32
Many groups have a vested interest in the development and implementation of HRSN initiatives in clinical settings, including patients, healthcare professionals, and community organizations.17,21,22,33 However, limited research has examined and synthesized perspectives across these groups, especially those in academic health center settings.28,31,34,35 When new initiatives are developed, exploring the perspectives of such groups is considered a best practice for successful implementation. Namely, it is critical to understand the needs and preferences of patients as they have the potential to reap the most benefit or suffer the most from unintended consequences, clinical teams’ readiness to adopt and ability to accommodate new workflows within already constrained environments, and the impact on community organizations that may be involved in care coordination and referral assessments, yet whose input is often limited or absent.21,26,33,36 Understanding concerns and recommendations across these groups can help identify principles and approaches for optimal integration of HRSN data into healthcare workflows. This study contributes to the existing literature by integrating perspectives from multiple interest-holder groups that are often studied separately but who are each essential for effective HRSN processes, allowing for a breadth of insights to inform implementation of HRSN initiatives in academic health centers.
Objectives
The purpose of this study was to solicit input via focus groups from key interest-holders on implementing HRSN screening and support in adult primary care clinics at an academic health center that did not previously have formal HRSN screening in place. We use the term “interest-holders” to represent people from groups who are “responsible for or affected by health-related decisions that can be informed by research evidence.” 37 The study sought to inform implementation of an HRSN initiative that would target patients with type 2 diabetes, a group known to be adversely impacted by HRSN. 7 We specifically focused on how to optimize the collection, integration, and use of HRSN data. Three research questions guided our study:
Methods
Study Setting
The study was conducted at 6 primary care clinics that are part of a large academic health center in the southeastern United States. The academic health center serves a diverse patient population with respect to race and ethnicity, socioeconomic status, and rural/urban geography, reflective of the region. More than 25% of patients come from under-resourced communities. The study received exempt status from the academic health center’s Institutional Review Board (IRB #232040).
Participants
We used a descriptive qualitative design to understand perspectives from 4 key groups of interest: primary care clinicians, clinic staff, and adult patients, and representatives of local community organizations. Clinicians (ie, physicians or nurse practitioners) and staff (ie, registered nurses, medical assistants, and patient service specialists) worked at 1 of the 6 partnering primary care clinics, were identified using a list provided by clinic directors, and invited to participate via email. Patient participants were 18 years of age or older; received care at 1 of the 6 primary care clinics; had an active patient portal account; were marked as “OK to contact” for research in the EHR; and were diagnosed with type 2 diabetes plus hypertension and/or hyperlipidemia. We first identified potential patient participants using the EHR and then sent these patients information about the study via the patient portal with an option to indicate their interest. If patients indicated interest, we emailed them a 4-question HRSN screener via a secure REDCap link to assess the presence of commonly reported social needs (ie, lack of reliable transportation, housing instability, lack of affordable healthcare access, and/or food insecurity).38,39 Patients were then formally invited to participate via email or phone call. We enriched our patient sample by ensuring patients with social needs were included; however, having a social need was not a requirement for participation. Community organization participants represented local community organizations that provide HRSN-related services (ie, food assistance, housing, and other health and human services). Participants were recruited with help from the project’s Advisory Committee, which is composed of 5 representatives from health care, community-based and non-profit organizations, and a grantmaking public charity. All focus group participants were English-speaking.
Data Collection
In keeping with our goal of informing implementation of an HRSN initiative, we used purposive sampling to help ensure representation within each group while adhering to the timeline of our initiative. Specifically, we invited patients to participate who represented different demographics (ie, gender, race, ethnicity, and types of social needs) and received care across the 6 primary care clinics. Staff and clinicians represented various roles and worked at different clinic sites. Community organizations represented different social needs sectors, including food assistance, housing services, and health and human services.
Focus group guides were developed by the experienced research team, informed in part by the Health Equity Implementation Framework (HEIF) given its usefulness in identifying determinants prior to implementation,40,41 and adapted for each interest-holder group. For example, for the clinician focus group we asked the question “What are some common challenges you have, or anticipate having, when addressing patients’ social risk factors?”, which targeted the clinical encounter domain. Focus groups were conducted separately with each of the 4 groups to promote peer-based dialogue. All focus groups were held virtually. Two trained study personnel (JH and EB) facilitated focus groups, 1 serving as moderator and the other as notetaker.
Prior to initiating each session, participants received information about the study (eg, voluntary nature, discussion guidelines, etc.). We also provided participants with a definition of social needs to help orient the focus group discussions (ie, things outside the doctor’s office that affect someone’s health and well-being; examples include difficulty with accessing health care, food, housing, and/or transportation). Because HRSN screening was not formally integrated in the clinics at the time of this study, we asked participants about their perspectives on integrating HRSN processes into clinic workflows. However, some participants had prior experiences with HRSN in other settings, which they reflected on when providing input. Focus groups lasted between 40-55 min, were audio-recorded, de-identified, and transcribed. Participants were compensated $50. We conducted focus groups from March to July 2024.
Data Analysis
The analysis team consisted of 4 qualitative researchers with expertise in biomedical informatics, anthropology, and public health (JH, LLN, EB, and KL). An inductive-deductive thematic analysis approach was adopted. 42 To develop the codebook, an initial set of deductive codes representing the HEIF was set up in Dedoose®.40,43 The HEIF was used as a foundational coding scheme to capture topics relevant to our research questions, specifically interactions in clinical encounters and societal context. 40 Using an inductive approach to identify themes directly arising from the data, team members also coded transcripts for implementation barriers and facilitators. Two team members (JH and LLN) independently coded 2 focus group transcripts, selecting excerpts and tagging them with 1 or more codes. To establish trustworthiness, they organized routine consensus meetings to discuss emerging code application and interpretation, resolving discrepancies through discussion and documentation of decisions in Dedoose. The coders then re-coded the first 2 transcripts using the refined codebook to ensure consistent and accurate coding of remaining transcripts. The analysis team convened weekly to address the project’s research questions. The team exported coded excerpts to Microsoft Excel for subsequent summarization and analysis. Insights from excerpts were summarized for each of the research questions, and the team reviewed associated coding for additional insights. The result was a matrix of insights for each research question, stratified by each group.
The researchers engaged in ongoing reflexivity throughout the research process, including reflecting on their roles as part of an implementation team, the contextual knowledge they had as members of the institution where the HRSN initiative would be implemented, the pragmatic scope of the study, and their own personal patient experiences. The researchers also regularly reflected during team meetings to discuss data interpretations, insights, and challenges, and to mitigate potential biases due to their professional and academic backgrounds.
Results
Across our 4 interest-holder groups, we conducted a total of 6 focus group discussions (N = 31): 2 with clinicians (n = 9), 1 with clinic staff (n = 6), 2 with patients (n = 11), and 1 with community organizations (n = 5). Table 1 provides participant characteristics. Table 2 includes representative quotes organized by theme/insight and participant type. Key themes are described below.
Participant Characteristics.
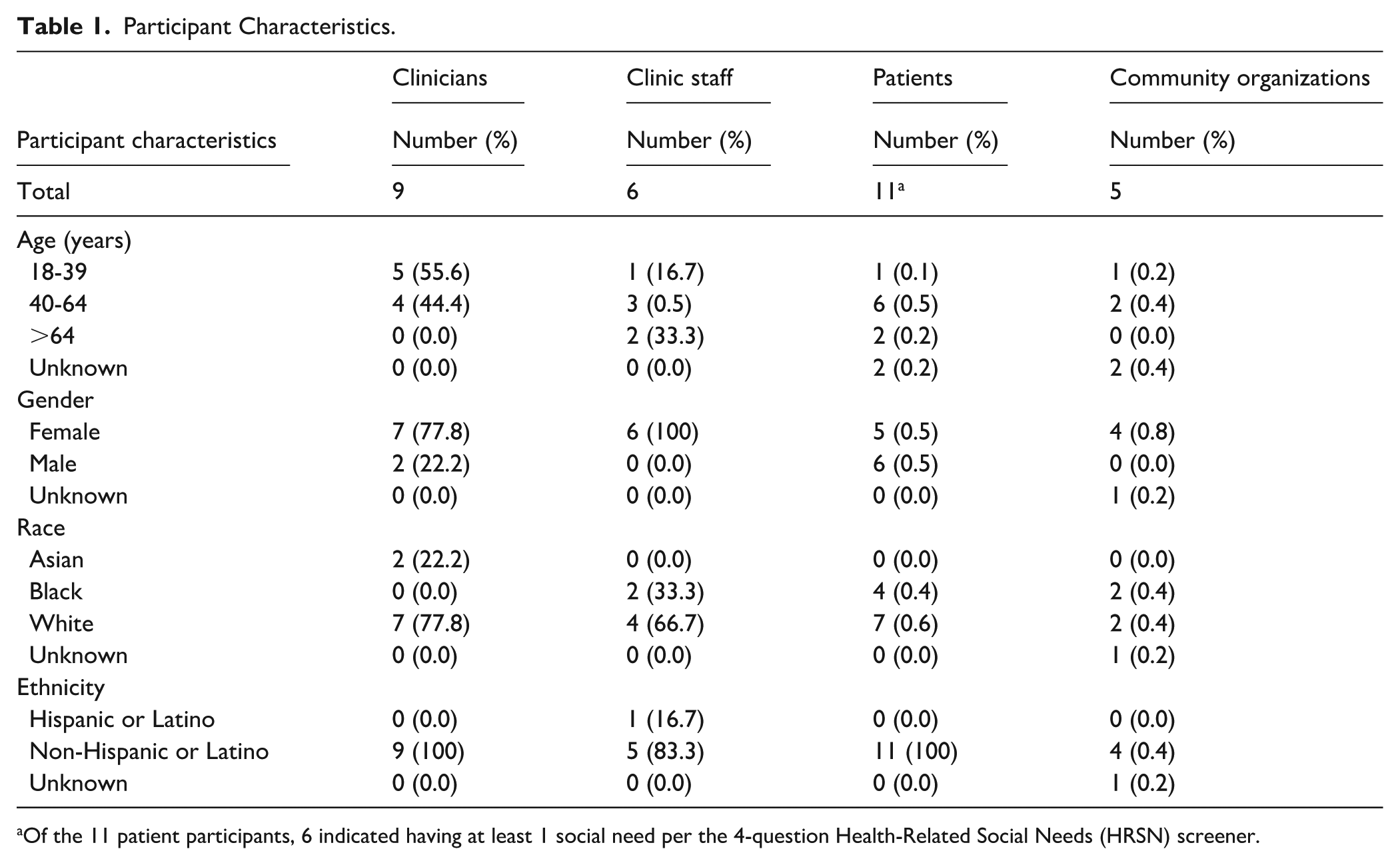
Of the 11 patient participants, 6 indicated having at least 1 social need per the 4-question Health-Related Social Needs (HRSN) screener.
Representative Quotes by Participant Type.

HRSN Data Collection and Resource Connection as Intrinsically Linked
Across clinicians, staff, and patients, there was a consensus that HRSN data collection should be accompanied with actionable support. Clinicians and staff expressed concern about HRSN screening without a robust infrastructure for addressing HRSN once identified (see Table 2, Quote 1 [Q1]). They reported a stronger preference for asking patients about needs they deemed clinically actionable (eg, medication affordability and transportation), rather than more complex needs (eg, housing), but wanted to ensure support for those needs was readily available [Q2].
Similarly, patients felt strongly about addressing identified HRSN during clinic visits. However, patients were skeptical that sharing HRSN information would lead to action, recalling prior experiences where their concerns were not addressed [Q3]. They also questioned how HRSN data are stored, shared, and tracked. They expressed clear expectations that if HRSN questions are asked, then the provider should acknowledge and act on disclosed needs, even if not the primary reason for the visit.
Clinicians, staff, patients, and community organizations all advocated for on-demand connection to resources. Staff and patients thought it would be helpful if patients received printed information about resources and how to access them during their visit [Q4]. Clinicians, staff, and community organizations recommended that healthcare systems invest in on-site resources, such as a food pantry or subsidized food pharmacy, which they believed could reduce access barriers and help address more immediate needs [Q5].
Organizational and Interpersonal Communication to Facilitate HRSN Practices
Clinicians, staff, and patients emphasized the need for organizational and interpersonal communication to create environments that facilitate HRSN screening and support. Clinicians and staff shared experiences where patients seemed uncomfortable disclosing HRSNs and only learning of patients’ social needs after several visits or indirectly when asking other questions [Q6 and Q7]. In addition, staff reported having limited organizational guidance for the collection and use of HRSN data [Q7]. Staff and clinicians agreed that effective and structured communication can help normalize HRSN discussions, thereby reducing discomfort and stigma and creating safe environments for sharing HRSN information [Q8].
Similarly, patients shared experiences where poor patient-provider communication caused patients to withhold information. One patient recalled feeling rushed during a visit and was uncomfortable shifting the conversation to discuss their social needs [Q9]. Conversely, another patient appreciated when their provider initiated the conversation about accessing services but also recognized the value of patients advocating for themselves to ensure their voices are heard [Q10]. Overall, patients desired a judgement-free, safe space where their concerns are taken seriously and open communication about HRSN is prioritized.
Standardizing HRSN-Related Practices for Screening and Referral
Clinicians, staff, and patients discussed the need for streamlined data collection processes, especially those that mitigate patient barriers to providing this information. Namely, all 3 groups preferred an annual cadence for screening, given the already extensive set of intake questionnaires for each visit. Some staff reported a lack of guidelines and standard practices for conducting HRSN screening and providing support. Staff mentioned that they often collect HRSN data only when completing annual Medicare wellness exams and that established protocols for acting on the self-reported data did not exist [Q11]. Clinicians stressed the importance of data collection methods that are inclusive and accessible, and minimize the burden placed on patients [Q12]. They explained that online pre-visit forms might create challenges for some patients, especially those with limited digital literacy and/or access to technology.
Patients noted differences in the collection and use of HRSN within clinics and across primary care locations. Inconsistences sometimes led to confusion and inefficiencies, suggesting a need for a more uniform approach across clinical settings [Q13]. Patients also recommended reducing redundant questions and sharing responses across providers to avoid repeat screenings and embarrassment from re-sharing sensitive information [Q14].
Assessing Staffing Models and Practice Alignment
Clinicians and staff believed social work and other in-clinic support staff (eg, case management, pharmacists, and dietitians) were essential to support patients’ social needs. They suggested integrating these roles into staffing models and clinical workflows, perceiving a lack of adequate staffing to support HRSN initiatives [Q15 and Q17]. Notably, they felt strongly there should be institutional buy-in and financial resource commitment to hiring full-time staff, particularly social workers [Q16 and Q17]. Both clinicians and staff felt appropriate staffing would be especially helpful given clinical time constraints and the added burden of HRSN screening. Clinicians explained that focusing on patients’ chief complaints during visits would leave little time for collection of HRSN data and effective engagement in service referrals [Q18]. Staff alluded to concerns about practice alignment and recalled instances when they had to perform HRSN-related tasks in the absence of social work or other more qualified personnel [Q17].
Leveraging the EHR to Bridge and Automate Clinical Workflows
Clinicians’ perspectives were most prevalent in discussions about leveraging the EHR to optimize workflows. They highlighted the importance of building EHR features that streamline screening, referral, and follow-up processes. This included making HRSN information easily accessible at the point of care and flagged for follow-up [Q19]. They advocated for clinical decision support (CDS) tools with minimal disruption to workflow and efficient pathways to connect patients with resources and support (eg, referrals to clinic-based social workers [Q20] or community organizations). Clinicians also recommended limiting the number of required steps to complete an action in the CDS, emphasizing that a goal should be saving time.
A closed-loop referral system and the ability to auto-populate resource information were among clinicians’ top EHR preferences. Closed-loop systems allow clinicians to directly refer patients to HRSN services while providing a real-time view of whether the service was accessed. Clinicians wanted closed-loop tracking integrated within the EHR to stay informed about patients’ status and outcomes. One clinician proposed embedded smart links that integrate into progress notes to more easily track patients’ HRSN [Q21]. Additionally, clinicians thought the after-visit summary was a suitable place for the EHR to auto-populate information about HRSN services and resources, particularly in the patient’s preferred language [Q22]. This was proposed as one way to provide patients with easy access to the support they need.
Optimizing Referral Processes
Staff, community organizations, and patients all expressed concerns about limitations with existing referral processes and being able to adequately address HRSN. Staff noted that limited capacity from community organizations greatly impacted their ability to make referrals and patients’ ability to access resources. Community organizations agreed, reporting challenges related to resource availability and capacity to meet increasing demands for HRSN services [Q23]. Both groups also identified eligibility requirements as a barrier to providing referrals. Namely, community organizations operate under specific criteria for whom they can provide services and often patients do not qualify [Q23 and Q24]. One community organization added that navigating eligibility hurdles requires robust case management beyond their provisions. Patients expressed a strong desire for closed-loop processes wherein the referring provider or clinic follow up with the patient to ensure a successful connection [Q25].
Community organizations highlighted the need for improved referral processes that facilitate information sharing between healthcare and community organizations and connection to services. Community organizations require referral-specific information to provide high-quality referrals but typically receive limited information. Further, patients are often left to navigate referrals on their own and when they show up to receive assistance, they are not sure why they were referred. Community organizations thought direct involvement from clinicians, namely filling out an online referral form for patients, emailing the organization about the nature of the referral, or initiating a warm handoff, would help create more effective workflows [Q26]. Additionally, although focus group participants thought social service resource locator (SSRL) vendors (eg, FindHelp and Unite Us) could facilitate access to resources, 1 community organization expressed concerns due to their perceived unfair business model that incentivizes vendors but overburdens local non-profits that already have limited capacity to serve the community [Q27].
Although experiences interacting with healthcare organizations varied, community organization participants agreed that establishing intentional and direct partnerships between healthcare systems and community organizations is a crucial component of HRSN initiatives. They provided examples of how successful collaborations facilitated better resource provision for social needs and achieved shared goals. This included working with healthcare systems to deliver medical care via mobile clinics, establishing on-site food pharmacies, and training personnel on navigating community resource databases.
Discussion
HRSN initiatives are becoming more common in clinical settings, with many demonstrating improvements in process, clinical, and social outcomes.5,6,20-23,27 However, there is still a need to optimize implementation across both clinical and community contexts. Addressing structural and operational gaps is essential to improve social needs care and facilitate long-term success of HRSN initiatives.6,21-23 This study provides a novel contribution to understanding and addressing these gaps by incorporating insights from multiple interest-holder groups spanning the continuum of HRSN care—from screening to resource connection—and seeks to provide guidance that has practical relevance. We gathered perspectives from clinicians, staff, patients, and community organizations to guide the implementation of an HRSN screening and support initiative within adult primary care clinics at an academic health center. Insights from the interest-holders represented their problem-solving around the gaps in existing systems and tensions that can arise around role clarity, clinical priorities, organizational responsibility, and effective communication. Taken together, our findings point to several key recommendations for developing organizational capabilities to successfully engage in HRSN-related endeavors.
Recommendation 1: HRSN Initiatives Should Involve Pre-implementation Planning and Investment in Areas That Position Them for Success
Pre-implementation planning includes assessing current practices and systems and making strategic choices about the initiative, such as data collection procedures, resource allocation and prioritization, planning for hiring and training personnel, and planning for interactions with community organizations. Moreover, HRSN initiatives require commitment to investing in and maintaining these systems, as well as securing leadership buy-in to tackle systemic gaps that hinder the success and sustainment of HRSN programs.17,20,21 Organizations should also invest in a robust EHR infrastructure, which might require funding to develop and maintain EHR features and to support dedicated effort for health IT personnel. 22 Planning should also establish clear protocols to ensure that screening leads to tangible strategies and support for addressing identified HRSN, such as adjusting care or providing referrals to community organizations, and processes to assess successful referral connections and determine whether social needs were addressed.44-46 This is essential for bolstering patients’ trust in the healthcare system’s ability to support their needs, improving job satisfaction and perceived quality of care for clinicians and staff, and moving the needle to impact patient outcomes.
Data privacy protections should continue to be at the forefront of decision-making around HRSN in healthcare systems, including confidentiality and data sharing across organizations.17,44,47 There is also a desire for data to be shared with community organizations by healthcare systems for better collaboration to meet patients’ needs; however, data interoperability standards are still being developed.45,48
Finally, organizational commitment must include investment in leadership to manage relationships through engagement with community organizations.21,33,49-51 To move toward a closed-loop care coordination infrastructure that works with community services to better meet patient needs, implementation of HRSN initiatives should be approached as a collaborative effort.7,51
Recommendation 2: Ensure Appropriate Expertise Is Present to Support an Effective HRSN Initiative
Trained social workers or equivalent health professionals are needed for effective screening, referral, patient navigation, and follow-up. Depending on the clinical setting, this may include full-time social workers or other support staff. For example, HRSN-based quality improvement and research projects have effectively utilized community health workers, case managers, and social workers in their workflows.20,27,50,52-55 Implementing such a staffing model could improve the quality of HRSN data collection and timeliness of resource connection and ensure sensitive issues are handled appropriately. It could also alleviate competing demands and time constraints experienced by already stretched primary care clinicians and staff.17,19,20,45
In addition to bringing in trained personnel for frontline patient interaction, organizations need to train health professionals in a team-based approach to care, in which the clinicians, nurses, social workers, and other health professionals integrate their varied forms of expertise into fast-paced clinical settings. A collaborative model, coupled with proper training, can help encourage an organizational culture that prioritizes holistic and quality care and increase the potential effectiveness of HRSN initiatives at improving health outcomes.17,19,27,45
Recommendation 3: Ensure Resources Are Available for Effective HRSN Screening and Follow-up
Key resources identified by focus group participants include EHR infrastructure for HRSN workflows, on-site resources for addressing HRSN, and EHR-integrated community resource directories. Although the evidence base for EHR integration into HRSN initiatives is still emerging, 22 our study participants emphasized that EHR features should be designed to minimize disruptions in clinical workflows while providing essential information and support. Features that can contribute to success are clinical decision support tools, documentation to enhance collaboration between team members, information that is readily available during patient visits and closed-loop referral capabilities.20,56,57
Focus group participants specifically recommended on-site resources to streamline meeting patients’ social needs by making resources immediately available during clinic visits. This would require developing internal social needs services, and could include simpler solutions, such as having clinic-based community resource lists available for patients, to more involved solutions, such as an on-site food pantry or internal referral to a social worker, pharmacist, or legal help.8,20,51 Potential benefits include reducing barriers related to time, transportation, accessibility, and difficulty navigating the referral process, potentially leading to more effective HRSN initiatives. However, on-site services may require funding, additional personnel, space, and a negotiated arrangement with 1 or more service providers.
A community resource directory with EHR integration could help providers identify and refer patients to community organizations. While some healthcare systems have their own built-in EHR resource directory, not all enable systematic referral tracking and typically require regular upkeep, which can be time- and resource-intensive.22,58 Alternatively, third-party SSRL vendors, which are for-profit entities that provide electronic resource directories and facilitate referrals, have emerged as promising tools for supporting workflows.48,58-60 Potentially, SSRLs can optimize referral processes, facilitate resource connection, and enable referral tracking. However, the usefulness and utility of SSRLs are still being understood, such as referral functionality, maintenance costs, longevity and sustainability, interoperability, and uptake among community organizations.21,48,58-60 Additionally, as our research and other studies have shown, there is skepticism about the benefit of SSRLs to community organizations as they can increase demand without contributing resources (ie, funding) to also increase capacity and can be burdensome to adopt.21,48,60 Healthcare organizations should formally weigh the tradeoffs of investing in an SSRL versus building their own communication system with community organizations, while being mindful that community capacity and buy-in from local community organizations are critical factors requiring intentional investment and engagement for effective resource provision.58,61
Recommendation 4: Effectiveness in Addressing HRSN Hinges on Optimizing the Program for the Local Setting
The system required to successfully address HRSN in a community involves meaningful engagement and bidirectional information sharing between organizations. Communities are unique ecosystems, which have varied relationships among local healthcare and community-based organizations.21,49 Relationships should be nurtured in a systematic way, enabling all who need potentially dynamic information about a community organization (eg, wait time for services, revisions to services offered, etc.) to access it on demand, rather than through word of mouth or informal colleague networks. This requires intentionally building effective and solution-focused partnerships, as well as sustaining these relationships, so that processes between the healthcare system and non-health care setting properly function.21,22,44,48,50,57,61
Furthermore, the ability for local community organizations to fulfill social needs referrals depends on the type of social need, infrastructure, local capacity, and availability of resources.6,21,33,45,61 For example, participants in our study identified food insecurity, transportation, and medication affordability as top actionable social needs; however, they also noted that capacity to address food insecurity was low and eligibility requirements for transportation was a limiting factor in resource connection. Both social needs prevalence and community capacity should be considered for HRSN initiatives, which involve collaborations between the healthcare systems and community organizations.21,33,49
Limitations
This study has some limitations. First, although we included several different types of community organizations, we were only able to recruit 5 community organization participants due to a low response rate from the organizations we contacted. This sample size may have restricted our ability to fully capture perspectives from community organizations and could affect the generalizability of our findings. Second, patients were only recruited using the patient portal so a selection bias may have occurred, potentially favoring patients who more actively use technology. Third, because our HRSN initiative is targeting patients with diabetes, we prioritized recruiting individuals from this population for the focus groups which may limit generalizability to other patient populations; notably, our focus group guides did not specifically ask about or refer to diabetes. Fourth, a key strength of focus groups is their ability to foster dynamic exchange of ideas and experiences; however, they also carry inherent biases such as groupthink, social desirability, and moderator influence. Supplementing our focus groups with in-depth interviews could have allowed for deeper exploration of individual perspectives and mitigated some of these biases, but this was not feasible within our grant timeline. Fifth, given timeline constraints and difficulty recruiting certain groups, we acknowledge that data saturation may not have been met; however, there was strong consensus within focus groups. Lastly, geographic location and context should be considered when interpreting findings as some of the challenges posed and recommended solutions might not be applicable to other settings.
Conclusions
This study adds to the growing body of work on HRSN screening and support and offers a unique contribution by synthesizing perspectives across multiple interest-holder groups for shaping effective HRSN initiatives within primary care settings. The successful development and integration of HRSN initiatives requires a multifaceted approach that includes dedicated staffing, standardizing data collection, providing resources and support for meaningful action from healthcare providers during clinical encounters, streamlining EHR functionalities, and ensuring all key players are properly trained. Organizational commitment is another crucial aspect for initiatives to be successful and should not be overlooked. Furthermore, HRSN initiatives must consider the role of community organizations and their capacity to provide services that address social needs. Recommendations from this research are broadly applicable and can help guide pre-implementation and implementation in other large academic centers to effectively identify, support, and address HRSN.
Footnotes
Acknowledgements
None.
ORCID iDs
Ethical Considerations
The study was approved and received exempt status from Vanderbilt’s Institutional Review Board (IRB #232040) on January 18, 2024.
Consent to Participate
This study received an exempt status; therefore, the study was exempt from the requirement for informed consent to participate by the Institutional Review Board. Prior to focus groups, facilitators provided information to participants about the study and what to expect. Specifically, participants were made aware that the study was considered research and their participation was voluntary. They were told about the study’s purpose, duration, and procedures. They were informed that the focus group sessions would be recorded and that their information would be de-identified and not shared outside of the research team. They were also told who to contact for questions about the research and research participants’ rights.
Consent for Publication
Not applicable.
Author Contributions
Kelsea LeBeau: Conceptualization; data curation; formal analysis; investigation; methodology; project administration; resources; validation; writing—original draft; and writing—review and editing. Erin M. Bergner: Conceptualization; formal analysis; investigation; methodology; validation; writing—original draft; and writing—review and editing. Joyce W. Harris: Conceptualization; data curation; formal analysis; investigation; methodology; validation; writing—original draft; and writing—review and editing. Laurie L. Novak: Conceptualization; data curation; formal analysis; investigation; methodology; validation; writing—original draft; and writing—review and editing. Isaac Schlotterbeck: Conceptualization; investigation; project administration; and writing—review and editing. Sunil Kripalani: Conceptualization; funding acquisition; resources; supervision; and writing—review and editing. Lyndsay A. Nelson: Conceptualization; funding acquisition; methodology; resources; supervision; and writing—review and editing. All authors contributed to the work and provided final approval of the version submitted for publication and agreed to be accountable for all aspects of the work as presented.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Minority Health and Health Disparities (NIMHD) under Award Number P50MD017347-03S3. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Per IRB approved protocol and for participant anonymity, non-aggregate data will not be available by request.