
Abstract
Background:
Type 2 Diabetes Mellitus (T2DM) presents a significant public health challenge, particularly in developing countries, where healthcare resources are limited. Community-Based Interventions (CBIs) have been explored as a strategy to improve glycemic control, yet evidence regarding their efficacy in reducing HbA1c levels in these settings remains limited.
Aim:
This study aimed to evaluate the efficacy of community-based interventions in improving HbA1c levels among patients with T2DM in developing countries.
Methods:
A systematic review and meta-analysis were performed following PRISMA guidelines. A comprehensive literature search was conducted in PubMed, Scopus, Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, Ovid-Medline, and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases for full-text randomized controlled trials (RCTs) published between 2015 and 2024. Studies conducted in developing countries focusing on community-based interventions targeting HbA1c outcomes were included. Quality appraisal was conducted using the Joanna Briggs Institute (JBI) critical appraisal tools. Statistical analysis employed a random-effects model to calculate the pooled mean difference (MD) with 95% confidence intervals (CI). Heterogeneity was assessed using the I2 statistic. Potential publication bias was assessed using Egger’s test, the Trim-and-Fill method, and a funnel plot.
Results:
Twenty RCTs involving 4914 participants across developing countries were included. CBIs significantly reduced HbA1c levels compared to usual care, with a pooled MD of −0.54 (95% CI = −0.71, −0.36; P < .00001; I2 = 92%). Subgroup analysis showed that education-focused interventions (MD = −0.67; 95% CI = −1.02, −0.31) and physical activity-focused interventions (MD = −0.67; 95% CI = −1.14, −0.20) were the most effective. Analysis by income level revealed no significant differences in efficacy between lower-middle-income and upper-middle-income countries (P = .29). The greatest HbA1c reduction was observed during the 0- to 3-month measurement period (MD = −0.56; 95% CI = −0.90, −0.23).
Conclusion:
CBIs are an effective strategy for reducing HbA1c levels among patients with T2DM in developing countries, with significant benefits across diverse economic contexts and intervention models. These findings highlight the adaptability and scalability of CBIs, underscoring their potential to enhance diabetes management in resource-limited settings.
Keywords
Introduction
Type 2 diabetes mellitus (T2DM) is a major global public health challenge, affecting 1 in 11 adults worldwide and accounting for 11% of annual deaths.1,2 It was estimated that 415 million people were affected by diabetes in 2015, with projections indicating that this number will rise to 642 million globally by 2040. 3 While historically more common in high-income countries, the prevalence of type 2 diabetes is projected to rise significantly in middle-income nations. 4 It places significant strain on individuals’ socioeconomic status and imposes a substantial financial burden on global healthcare systems. 5
The management of diabetes is crucial in reducing hemoglobin A1c (HbA1c) levels among patients with T2DM by enhancing their knowledge, skills, and abilities for effective self-care. 6 Studies indicate that a 1% reduction in HbA1c levels is associated with a 21% lower risk of developing diabetes-related complications. 7 HbA1c is considered as the gold-standard assessment and biomarker of diabetic patients to monitoring the levels of glucose.7,8
For the management of all diabetic patients, the primary therapeutic goal is to achieve and maintain good glycemic control, thereby preventing macro and microvascular complications. 9 The evidence of the advantage of glycemic control included reducing macro and microvascular risk complications, 10 reducing 9% in the risk of major adverse cardiovascular events, 11 lowering HbA1c, 12 and preventing or delaying the progression of nephropathy, retinopathy, and neuropathy. 13
Community-based interventions (CBIs) have been widely employed to enhance glycemic control in patients with type 2 diabetes mellitus (T2DM). These interventions are tailored to the specific cultural, social, and economic contexts of the target population. 14 CBIs actively involve patients in their care plans, empowering them to take ownership of their health. 15 CBIs are cost-effective, as they often utilize local resources and infrastructure. 14
Any type of CBI, including group education focused on empowerment for individuals with T2DM, has been shown to effectively reduce HbA1c levels by enhancing patient self-awareness and improving their ability to manage the disease through psychological, habitual, and behavioral changes.2,16 -18 Moreover, a preceding systematic review determined that health behavior interventions aimed at enhancing T2DM management are effective strategies for improving the quality of life (QoL) of diabetic patients with limited resources in developing countries. 19
Despite the recognized benefits of CBIs, evidence regarding their efficacy in improving HbA1c levels among patients with T2DM in developing countries remains limited. While a systematic review has examined the impact of CBIs, its focus has been on prevention programs rather than targeted patients diagnosed with T2DM. 20 Another systematic review also explored CBIs in T2DM prevention without employing meta-analysis, which cannot provide a pooled quantitative estimate of their effectiveness. 14 This systematic review and meta-analysis aim to evaluate the efficacy of CBIs in reducing HbA1c levels among patients with T2DM in developing countries. It seeks to identify the most effective intervention models, assess the influence of income level, and determine the optimal follow-up duration for achieving meaningful HbA1c reductions. Thus, addressing these gaps will provide evidence-based recommendations to strengthen diabetes management in resource-limited settings.
Materials and Methods
Study Design
This study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 21 The review was registered with the International Prospective Register of Systematic Reviews (PROSPERO; Registration Number: CRD42025631051). The PICOS (Population, Intervention, Comparison, Outcomes, and Study/Settings) framework was developed to outline the components of this review.
Eligibility Criteria
Inclusion Criteria
Population (P)
This review considered all studies involving adult patients diagnosed with T2DM, including both controlled and uncontrolled T2DM cases.
Intervention (I)
The review included RCTs that employed community-based interventions targeting T2DM management. These interventions could involve group-based programs or personalized care implemented within a community framework, addressing lifestyle changes, glycemic control, and self-management practices. Both remote-based interventions and conventional modes of delivery were considered.
Comparator (C)
Studies with any alternative interventions or no intervention (usual care) as comparators were included.
Outcome (O)
The primary outcome measured was the change in HbA1c levels. Only studies reporting HbA1c with means and standard deviations were included.
Study and Settings (S)
The review included all RCTs conducted in developing countries, as defined by the World Bank classification for 2024, encompassing low-income countries (LICs), lower-middle-income countries (LMICs), and upper-middle-income countries (UMICs).22,23
Exclusion Criteria
Studies were excluded if they: (1) focused on diabetes types other than T2DM (eg, type 1 diabetes, gestational diabetes, or juvenile diabetes); (2) patients with comorbidities such as hypertension, where outcomes were not specific to T2DM; (3) addressed diabetes prevention rather than management of patients has been diagnosed with T2DM; (4) did not report HbA1c levels as mean ± standard deviation (unless data could be calculated from the provided information); (5) did not use an RCT design (eg, qualitative studies, quasi-experiments, or case-control studies); or (6) were review articles, study protocols, or abstracts from conference proceedings without full-text availability.
Search Strategy
The search strategies were designed to capture all relevant studies published between 2015 and 2024, ensuring the inclusion of the most recent evidence on the topic. Only studies published in English were included to prevent translation-related challenges and potential misinterpretation. The search was conducted across 6 databases: PubMed, Scopus, CINAHL, Web of Science (WoS), Ovid Medline, and CENTRAL. To enhance the comprehensiveness of the review, hand-searching was performed by manually screening the reference lists of relevant articles, which helped identify studies that may not have been captured through database searches and strengthened the robustness of the search process. 24
The keywords were refined using Medical Subject Headings (MeSH) for PubMed, and Boolean operators (“AND” and “OR”) were applied to optimize the search strings. The concept keywords used in this manuscript included terms related to group interventions, glycemic control, and type 2 diabetes mellitus. The searches were conducted from inception until December 12, 2024. Supplemental File 1 provides detailed search strings and keywords used for each database.
Study Selection
The search results were imported into Covidence (Veritas Health Innovation, Melbourne, Australia), a systematic review management software. Using Covidence, 2 reviewers (I.S.H and H.I.M) independently screened the identified articles through their titles and abstracts. The full texts of the selected studies were then independently screened and assessed against the eligibility criteria. Any disagreements were resolved through discussion with the lead author (L.L) as needed.
Data Extraction
Two independent authors (D.P. and M.A.M.) independently extracted data from the included studies using a spreadsheet developed by the lead author and the 2 review authors. To ensure the accuracy of the data, all authors convened via Zoom to discuss any discrepancies and cross-check all extracted data. The data collected in the spreadsheet included study characteristics (eg, author, year, country, and study design), participant characteristics (eg, age and gender), and trial details (eg, total sample size, intervention sample size, and control group sample size). Intervention details were also extracted, including the type of intervention, control group details, follow-up, duration, and frequency of the intervention. Key outcomes, specifically post-intervention HbA1c (%) for both the intervention and control groups, were included in the data extraction process.
Assessment of Risk of Bias
The included studies, after full-text screening, were assessed and critically appraised for risk of bias by 2 review authors (I.J.W. and I.S.H.) using the methodological quality standards outlined in the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for RCTs. 25 The checklist includes 13 items, with each criterion rated as “yes,” “no,” “unclear,” or “not applicable,” and a total score assigned based on these ratings. A study was considered high-quality evidence if it achieved a “yes” rating for at least 69% of the checklist items. Studies were classified as moderate-quality evidence if they achieved a “yes” rating for 53% or below of the checklist items. 26
Data Synthesis and Analyses
The data analysis for this meta-analysis was conducted using Review Manager (RevMan; Computer program), Version 5.4, The Cochrane Collaboration, 2020. Outcomes were reported as continuous data, specifically HbA1c levels, which were measured consistently across the included studies. The summary statistics used were Mean Difference (MD), as HbA1c was measured in the same units across all studies. An inverse-variance method was applied during the meta-analysis.
The summary intervention effects of the CBIs were calculated as a weighted average of the intervention effects in each study and is presented as Cohen’s d. To assess heterogeneity among the studies, the χ2 test and I2 statistic were calculated using RevMan. The I2 values were interpreted as follows: low heterogeneity (I2 ≤ 25%), moderate heterogeneity (I2 = 26%-75%), and high heterogeneity (I2 > 75%). 27 A random-effects model was applied initially, as heterogeneity was anticipated due to variations in intervention models employed across the included studies. 28
Sensitivity analyses were conducted to exclude outlier studies and determine their influence on the overall heterogeneity. 27 Subgroup analyses were performed to explore potential sources of heterogeneity, based on income levels (LICs, LMICs, and UMICs) and HbA1c measurement periods (0-3, 4-6, 7-9, and 10-12 months). Sub-groups by intervention types were categorized into 5 models: education-focused, comprehensive behavioral, supportive counseling, remote-based, and physical activity–based. The education-focused and supportive counseling interventions were grouped separately because the former provided education only without counseling, while the latter centered on counseling and psychosocial support. Publication bias was assessed using a funnel plot, Egger’s test, and the Trim-and-Fill method.
Results
Study Selection
The study selection process is summarized in the PRISMA flow diagram (see Figure 1). A total of 1574 records were identified from database searches across PubMed (n = 418), CENTRAL (n = 418), Scopus (n = 404), CINAHL (n = 174), Web of Science (n = 133), and Ovid Medline (n = 19). An additional 6 records were identified through hand-searching reference lists, resulting in a total of 1580 records before duplicates were removed. After removing 332 duplicate records, 1242 unique records were screened based on titles and abstracts of these; 1153 were excluded for not meeting the inclusion criteria. The remaining 89 full-text reports were retrieved and assessed for eligibility. During the eligibility assessment, 75 reports were excluded for various reasons (see Figure 1). Ultimately, 14 studies were included from the initial database search, with an additional 6 identified through citation searching, resulting in a total of 20 articles included in the final analysis.

PRISMA flow diagram of study selection process.
Study Characteristics
The characteristics of the included studies are summarized in Table 1. A total of 20 studies, encompassing 4914 participants, were included in this review. Sample sizes ranged from 64 to 1190 participants, with intervention durations varying from 3 weeks to 24 months. The studies were conducted across various countries, categorized as LMIC (n = 3) and UMCs (n = 17). To streamline the analysis, the interventions were grouped into 5 categories: Remote-Based Interventions,29 -33 Education-Focused Interventions,34 -39 Supportive Counseling Interventions,40,41 Comprehensive Behavioral Interventions,42 -46 and Physical Activity-Focused Interventions. 47 For more detailed information, Supplemental File 2 provides a comprehensive overview of the included studies, including the country, intervention type, sample size, and HbA1c measurement timeline.
Characteristics of Included Studies (n = 20).

Abbreviations: CG, control group; IG, intervention group; LMICs, low- and middle-income countries; UMCs, upper-middle-income countries.
Efficacy of Community-based Interventions Compared to Usual Care
Figure 2 highlights the superior efficacy of CBIs compared to usual care in reducing the HbA1c. The pooled mean difference was −0.54 (95% CI = −0.71, −0.36, P < .00001), indicating an average reduction of 0.54 units in favor of CBIs, with strong statistical significance (P < .00001).

Efficacy of CBIs versus usual care.
However, due to high heterogeneity (I2 = 92%, χ2 P < .00001), a leave-one-out sensitivity analysis was performed to test the robustness of the results. As shown in Figure 3, sequential exclusion of high-weight studies33,36,41 reduced the overall pooled MD to −0.46 (95% CI = −0.69, −0.23, P < .0001). This adjustment reaffirms the consistent benefit of CBIs despite variations in individual study contributions.

Sensitivity analysis of the efficacy of CBIs versus usual care.
Subgroup Analysis of the Efficacy of CBIs in Reducing HbA1c
Table 2 summarizes the subgroup analysis conducted to evaluate the efficacy of various categories of CBIs in HbA1c reduction. Among CBIs intervention types, education-focused interventions demonstrated a substantial MD of −0.67 (95% CI = −1.02, −0.31, P < .00001, I2 = 90%), indicating that participants in the intervention group using education-focused approaches reduced their HbA1c levels by an average of 0.67 percentage points. Similarly, physical activity-focused interventions showed a significant mean difference of −0.67 (95% CI = −1.14, −0.20, P = .005), suggesting comparable efficacy to education-focused interventions. In contrast, remote-based interventions exhibited the smallest pooled effect, with a mean difference of −0.41 (95% CI = −0.92, 0.11, P = .12, Z = 1.54), reflecting no statistically significant impact. The overall test for subgroup differences (χ2 = 1.56, df = 4, Z = 5.99, P = .82) indicated no statistically significant differences between intervention types, suggesting comparable efficacy across subgroups.
Subgroup Analysis of the Efficacy of CBIs on HbA1c Reduction.
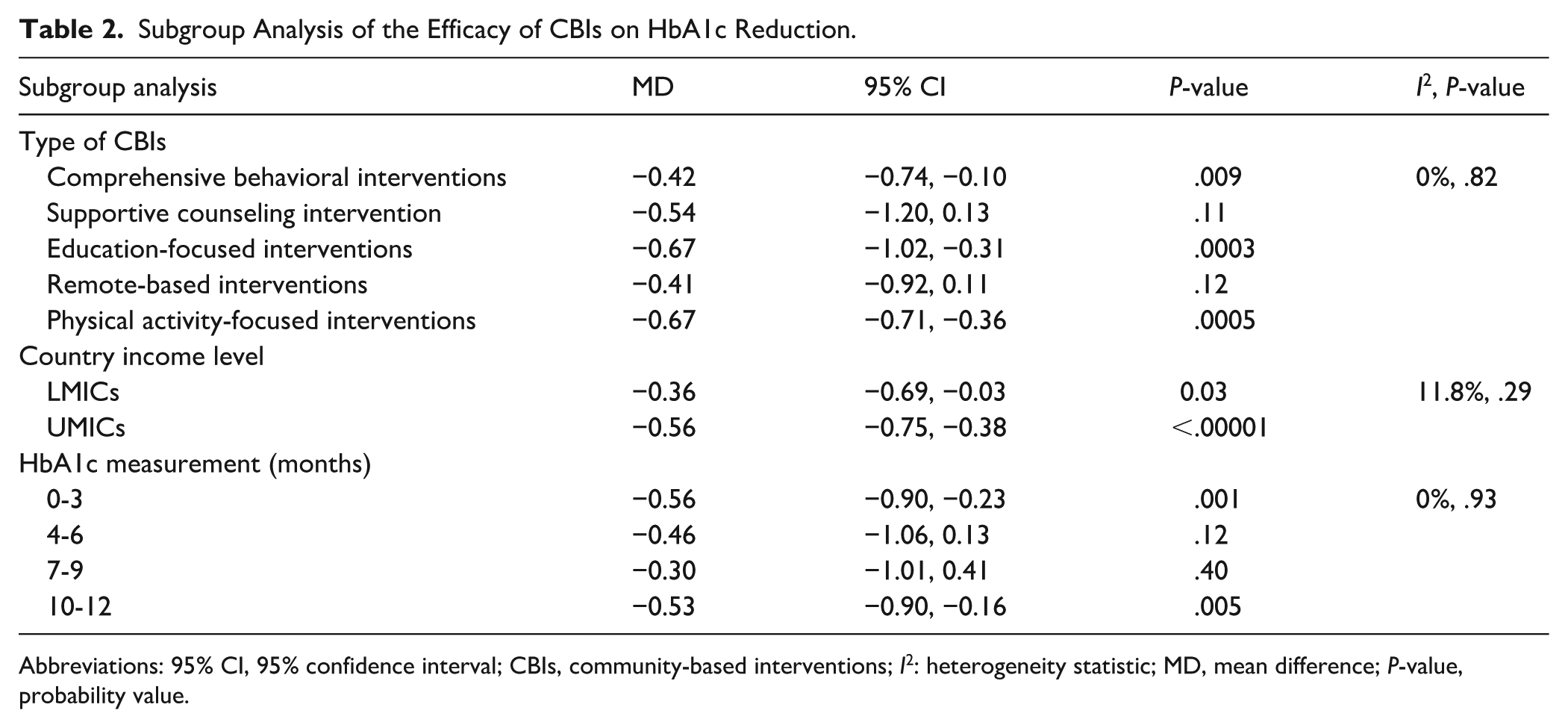
Abbreviations: 95% CI, 95% confidence interval; CBIs, community-based interventions; I2: heterogeneity statistic; MD, mean difference; P-value, probability value.
LMICs achieved a moderate but statistically significant mean reduction in HbA1c of −0.36 (95% CI = −0.69, −0.03, P = .03, I2 = 24%). In contrast, UMICs demonstrated a larger mean reduction of −0.56 (95% CI = −0.75, −0.38, P < .00001, I2 = 93%). Despite this numerical difference, the test for subgroup differences (P = .29) indicated no statistically significant difference between the 2 income groups. For HbA1c measurement periods, the most significant reductions were observed at 0 to 3 months (MD = −0.56, 95% CI = −0.90, −0.23; P = .001) and 10 to 12 months (MD = −0.53, 95% CI = −0.90, −0.16; P = .005), despite high heterogeneity (I2 = 89% and 95%, respectively). In contrast, the 4 to 6 months period (MD = −0.46, P = .12) and the 7 to 9 months period (MD = −0.30, P = .40) showed no statistically significant reductions. These findings suggest that CBIs are most effective during early follow-up (0-3 months) and later follow-up (10-12 months), while mid-term durations lack a significant impact on HbA1c reduction. For detailed subgroup analysis, Supplemental File 3 presents the forest plot results based on the model of community-based interventions, country income levels, and HbA1c measurement follow-up duration.
Publication Bias
The funnel plot in Figure 4 revealed notable asymmetry, indicating potential publication bias, which was further confirmed by the Egger test (P = .0052). To address this, the Trim-and-Fill method included 3 additional studies in the analysis. After adjustment, the random-effects model yielded a pooled SMD of −0.3144 (95% CI = −1.2994, 0.6706; P = .5316). The prediction interval ranged from −5.3958 to 4.7671, reflecting substantial uncertainty in the true effect size across various settings. Heterogeneity remained high, with an I2 of 97.3% (95% CI = 96.7%, 97.8%) and a τ² of 5.7510, suggesting significant variability among the included studies. The Trim-and-Fill analysis highlights the robustness of the findings but also underscores the need for cautious interpretation due to the variability and potential for missing data in the available evidence. Supplemental File 4 contains the results from Egger’s test and the Trim-and-Fill analysis.

Funnel plot with trim-and-fill adjustments.
Risk of Bias
Figure 5 illustrates that the majority of studies demonstrated moderate to high methodological rigor. Most studies exhibit a low risk of bias in key domains, such as the randomization process (D1) and baseline group comparability (D3). However, higher risks of bias were observed in domains related to blinding, particularly the blinding of participants and personnel (D4 and D5), where several studies encountered challenges in implementing proper masking due to the nature of the interventions. Additionally, blinding of outcome assessment (D6) showed moderate to high risks of bias in a subset of studies.
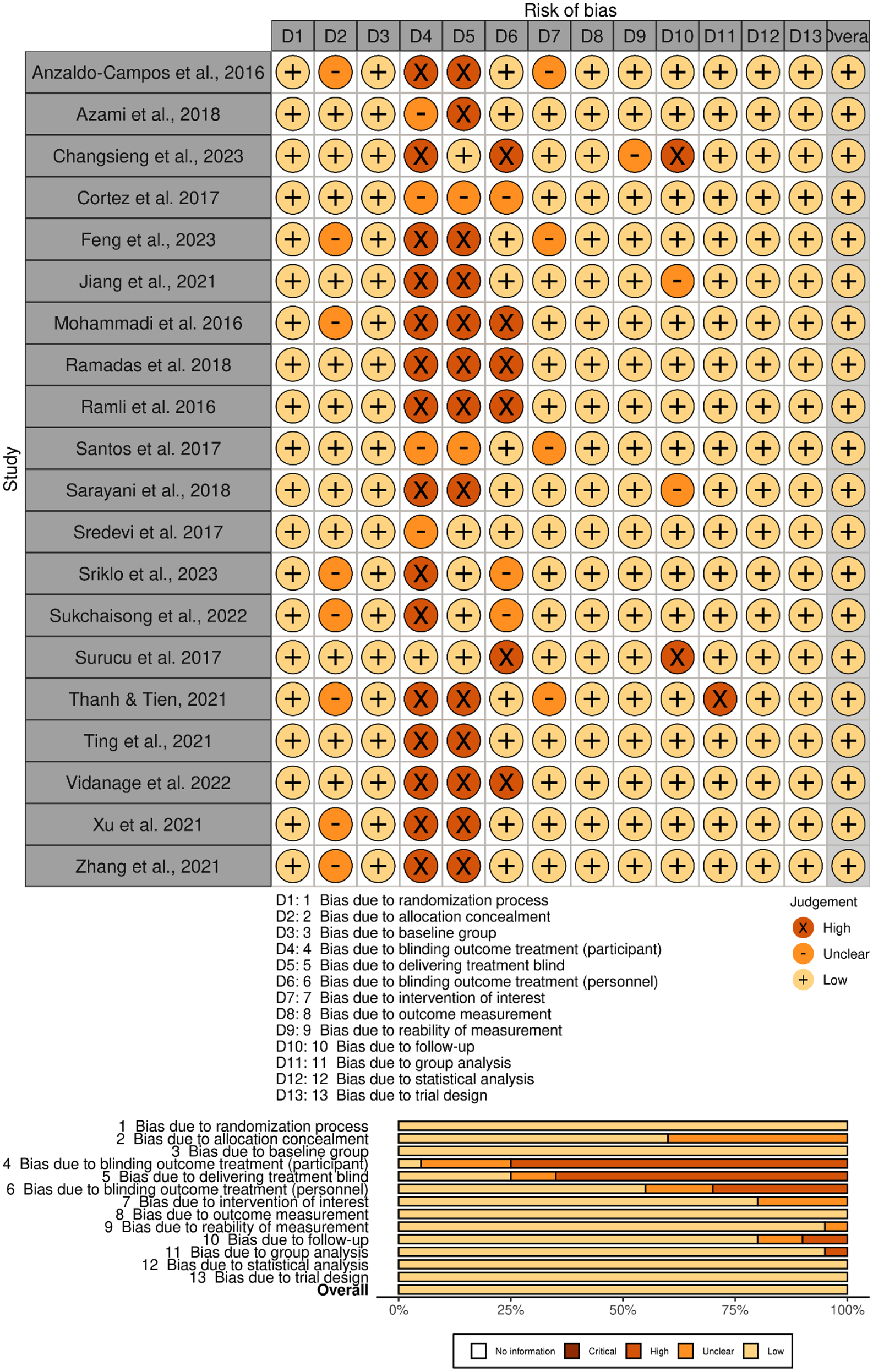
Risk of bias assessment visualization.
Most studies scored between 69.23% and 76.92%, reflecting an adequate level of methodological robustness. Studies such as34,37,39 demonstrated strong adherence to methodological standards and a high degree of reliability in their design and execution. In contrast, Thanh and Tien, 38 which scored 61.54%, indicated methodological concerns that warrant attention, particularly in areas such as randomization and outcome measurement reliability. Supplemental File 5 provides a detailed risk of bias assessment, including the JBI Risk of Bias Assessment scores for the included studies.
Discussion
This systematic review and meta-analysis confirm that CBIs are significantly more effective than usual care in reducing HbA1c levels among T2DM patients in developing countries. The most significant reductions in HbA1c were observed with group education-focused and physical activity-focused interventions. While interventions in UMICs showed slightly better outcomes compared to those in LMCs, the differences were not statistically significant. Substantial reductions were noted during short-term follow-up periods (3 months), while longer follow-up durations exhibited greater variability in HbA1c outcomes.
CBIs are effective in enhancing patients’ self-awareness about the importance of managing diabetes, including maintaining a healthy diet, engaging in regular physical activity, and adhering to prescribed medications. 19 CBIs also address the psychological burden of T2DM, as patients often experience chronic stress due to the demands of disease management. 37 Social support, a common component of CBIs, effectively reduces psychological stress, promotes emotional well-being, and improves overall diabetes management. 19 To maximize their efficacy, CBIs must be tailored to the specific cultural, social, and economic contexts of the target population. 38
The significant improvements in glycemic control observed in this study align with findings from prior systematic reviews and meta-analyses. Shirvani et al 51 reported substantial reductions in fasting blood glucose, HbA1c, and BMI through community-based educational interventions. Similarly, Tay et al 52 demonstrated the efficacy of lay-led group-based interventions in improving HbA1c and self-efficacy, reinforcing the role of community-driven approaches. Kobashi et al 53 further highlighted that community-based educational interventions led by non-healthcare staff significantly improved outcomes related to hypertension and diabetes in resource-limited rural settings, showcasing the scalability and adaptability of CBIs in addressing non-communicable diseases.
Educational interventions remain the most effective strategy for managing T2DM, demonstrating the most significant reductions in HbA1c. By targeting self-efficacy, knowledge, and quality of life, these programs equip patients with essential tools to monitor blood glucose, adhere to medication, improve diet, and incorporate physical activity.54,55 Health professional-led–led education fosters sustained clinical and lifestyle benefits through collaborative learning and group leadership, which promote shared experiences, problem-solving, and peer support.33,35,39,50 Session content can be adapted to include brainstorming, realistic goal-setting, and transformative learning methods. 48 Grounding these interventions in the health belief model, self-efficacy theory, and social support theory strengthens their impact by emphasizing risk awareness, instilling confidence in personal capabilities, and cultivating communal reinforcement. 39 Group-based education consistently enhances diabetes knowledge and health outcomes, including favorable changes in FBS, HbA1c, BMI, and waist circumference.51,53,54
Comprehensive behavioral and group-based physical activity interventions also show potential by combining education, exercise, and behavioral strategies. However, supportive counseling alone did not achieve statistically significant improvements, potentially because its focus on emotional support lacks the depth of behavior change or skill-building.41,56 Likewise, remote-based interventions have yet to produce significant results, possibly due to barriers such as limited technology access, reduced patient engagement, or insufficient tailoring to individual needs.57,58
This study also demonstrated that CBIs are effective in reducing HbA1c levels in patients with T2DM in both LMCs and UMCs. The efficacy of these programs can be attributed to the supportive and positive environment fostered through group-based interventions, which encourages knowledge sharing, behavior change, and mutual motivation.59 -61 This collective atmosphere promotes healthier lifestyle choices, ultimately contributing to improved glycemic control. Previous research supports this, showing that CBIs are effective in reducing HbA1c and fasting blood glucose levels in resource-limited settings, highlighting their adaptability to diverse socio-economic and cultural contexts. 14 However, several challenges hinder chronic disease management in LMICs, including complex health systems, limited community engagement, insufficient healthcare provider training, inadequate interdisciplinary collaboration, and financial constraints.62,63
In contrast, CBIs appear more effective in UMICs, potentially due to well-established healthcare systems that facilitate the implementation of sustainable health programs. 64 These systems benefit from secure financial investments, strong collaboration among healthcare providers and volunteers, and equitable resource distribution, ensuring comprehensive coverage for vulnerable populations. 65 Additionally, active community participation enhances implementation efficiency and contributes significantly to improved health outcomes. 66
Moreover, it is noteworthy that the 3-month follow-up period for HbA1c measurement demonstrated significant reductions in HbA1c levels. Kim et al 67 reported that achieving glycemic control within 3 months was associated with a 34.5% likelihood of maintaining long-term glycemic stability, highlighting the importance of early target achievement in managing T2DM. 67 These findings align with studies showing that interventions with follow-up periods of less than 6 months yield significantly better HbA1c reductions compared to follow-ups beyond 6 months. 17 This efficacy may be attributed to heightened patient motivation, stricter adherence to prescribed treatments, and active engagement in lifestyle modifications during the initial stages of intervention, which often diminish over time. 68
These findings highlight the significant potential of CBIs for diabetes management in developing countries. CBIs, tailored to local cultural contexts, offer a cost-effective, adaptable, and practical solution for resource-limited settings. Interventions focusing on physical activity and group based-education have demonstrated substantial improvements in diabetes management outcomes, requiring minimal financial investment and infrastructure. CBIs, with relatively short follow-up durations, effectively reduce HbA1c levels while alleviating strain on healthcare systems, promoting long-term program sustainability. To maximize their impact, integrating CBIs into national diabetes strategies and enhancing local capacities is crucial. This approach can reduce dependence on hospital-based care and improve healthcare accessibility for vulnerable populations. 69
Limitation
This review focused on RCTs conducted over the past decade to ensure the inclusion of recent evidence. However, this approach may have excluded older studies that could provide additional insights or historical context on the efficacy of CBIs in managing T2DM. Future reviews should adopt a broader time frame to capture long-term trends and evaluate the sustained impact of these interventions. Additionally, while the analysis demonstrated the overall efficacy of CBIs in reducing HbA1c levels, it primarily focused on the HbA1c as the primary endpoint. Secondary outcomes, such as improvements in quality of life, patient satisfaction, and long-term treatment adherence, were not comprehensively evaluated. Incorporating these outcomes in future studies would provide a more holistic understanding of the broader benefits of CBIs.
Moreover, the included studies were conducted only in LMICs and UMICs, with no studies from LICs, which may limit the generalizability of the findings. Future studies in LICs are warranted to provide more representative evidence. Lastly, significant heterogeneity was observed across the included studies, stemming from variations in intervention design, follow-up durations, and population characteristics. This variability may affect the generalizability of the findings to all developing countries. Future research should aim to standardize reporting and methodologies to enhance the comparability and reliability of results.
Conclusion
This systematic review and meta-analysis demonstrate that CBIs effectively reduce HbA1c levels among patients with T2DM in developing countries. By leveraging community-driven and culturally adapted approaches, CBIs enhance their applicability, sustainability, and cost-effectiveness in resource-limited settings. These findings highlight the scalability and adaptability of CBIs as a viable strategy for diabetes management. Policymakers and healthcare providers are encouraged to priorities CBIs in diabetes care, tailoring them to local cultural and healthcare contexts to maximize their impact. Future research should focus on identifying optimal implementation strategies and addressing potential publication bias to further strengthen the evidence base for global diabetes management.
Supplemental Material
sj-pdf-1-jpc-10.1177_21501319251391593 – Supplemental material for Efficacy of Community-based Interventions in Reducing HbA1c Levels Among Patients With Type 2 Diabetes Mellitus: A Systematic Review and Meta-analysis of Recent Studies Conducted in Developing Countries
Supplemental material, sj-pdf-1-jpc-10.1177_21501319251391593 for Efficacy of Community-based Interventions in Reducing HbA1c Levels Among Patients With Type 2 Diabetes Mellitus: A Systematic Review and Meta-analysis of Recent Studies Conducted in Developing Countries by Lutfian Lutfian, Izdihar Javier Wardika, Muhammad Amirul Mukminin, Ibnu Syarifudin Hidayat, Riki Wartakusumah, Hatifah Ihsanda Tien Melati, Dinar Perwitasari, Fahmi Wildana, Nur Widayati, Fulgence Niyibitegeka and Jonathan Hasian Haposan in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to express their deepest gratitude to Lembaga Pengelola Dana Pendidikan (LPDP) for supporting the publication charges and sponsoring the authors’ studies (L.L., I.S.H., H.I.T.M., J.H.H., and D.R.P.). Special thanks are also extended to Monash University for providing support throughout the review process and enabling its successful publication. The authors also acknowledge open access publishing facilitated by Monash University through its agreement with the Council of Australian University Librarians.
ORCID iDs
Author Contributions
L.L. conceptualized the study, developed the review protocol, led manuscript drafting, and supervised the overall process. I.J.W. and M.A.M. conducted the literature search, performed the risk of bias assessment, and contributed to data extraction and manuscript review. I.S.H. and I.J.W. supported the study design, performed study screening, and contributed to the sensitivity analysis. R.W. and H.I.T.M. contributed to subgroup analysis and results interpretation. D.P. and F.W. supported data extraction and provided input for the discussion. N.W. contributed to the introduction section. F.N. ensured data accuracy, reviewed included articles, refined data presentation, and contributed to revisions in the discussion and recommendation sections. J.H.H. provided statistical expertise, reviewed the meta-analysis methodology, interpreted findings, and conducted a comprehensive review of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.