
Abstract
Cardio-renal-metabolic syndrome (CRM) poses a critical and escalating threat to public health across Europe, demanding a unified and proactive approach. Current clinical practice is significantly limited by the absence of comprehensive, evidence-based CRM guidelines specifically designed for primary care physicians (PCPs). This deficiency leads to fragmented care and delays crucial early interventions. This article is a call to action for the immediate development of standardized European guidelines that enable the holistic management of CRM, prioritizing their swift adoption and implementation by PCPs across Europe. We urge a paradigm shift toward proactive screening, very early detection, and tailored, stage-specific management, recognizing PCPs as central coordinators of multidisciplinary care. To realize this, we propose concrete steps: robust PCP training in CRM diagnosis and management, the implementation of population-wide screening programs including eGFR, uACR, and NT-proBNP, and the removal of systemic barriers hindering access to optimal care. Moreover, we underscore the vital role of patient empowerment through education and support for self-management. This initiative aims to align national healthcare strategies with EU policy directives, fostering collaborative efforts among stakeholders to develop and implement contextually relevant guidelines. By establishing concise, actionable European guidelines, we can transform the management of hitherto separated medical disciplines spanning the CRM continuum, thereby improving patient outcomes and alleviating the substantial economic burden associated with this complex syndrome.
Introduction
Cardio-renal-metabolic syndrome (CRM), also known as cardiovascular-kidney-metabolic syndrome (CKM), 1 highlights the interconnectedness of cardiovascular, renal, and metabolic health.2,3 This syndrome, characterized by insulin resistance, chronic inflammation, and oxidative stress, drives conditions like type 2 diabetes (T2D), heart failure (HF), and chronic kidney disease (CKD). 4 CRM patients are often asymptomatic in their early stages, challenging early detection, hence leading to increased morbidity and mortality. Genetic, environmental, and socioeconomic factors further complicate risk assessment.
Effective CRM management requires a coordinated, systems-based approach integrating treatment with preventive measures, crucial for altering disease trajectory. This necessitates simple diagnostic tools and personalized therapies. Despite ongoing research, a gap exists in translating knowledge into practical clinical guidelines, especially for primary care physicians (PCPs).
Specialists have detailed protocols, but PCPs often lack consolidated best practice recommendations for holistic CRM management. This leads to fragmented care, delayed diagnosis, and suboptimal treatment, escalating CRM-related complications. Therefore, comprehensive, evidence-based guidelines tailored for PCPs across European countries are urgently needed.5,6 This initiative proposes developing such guidelines, empowering PCPs to implement preventive and therapeutic strategies, including lifestyle modifications, 7 shifting from mere reactive clinical symptom management to proactive prevention employing targeted screening, monitoring, and structured treatment strategies. Critically, these guidelines are essential for PCPs to serve as central hubs of connection between specialists and patients, ensuring seamless, coordinated CRM care. 8 Guidelines should consider existing local primary care capabilities while setting ambitious benchmarks for improved CRM management.
Patients at Risk
Definition
CRM is a progressive condition often initiated by a combination of biological, social, and environmental factors. These lead to unhealthy adipose tissue build-up, chronic inflammation, and oxidative stress, with insulin resistance being the common underlying pathophysiological denominator. 9 These conditions, especially insulin resistance, trigger further complications like arterial hypertension, dyslipidemia, and eventually T2D. 10 Over time, these interconnected pathways significantly increase cardiovascular morbidity and mortality risk, escalating exponentially with the development of end-organ damage such as heart failure, stroke, or CKD. Early identification and quick intervention are crucial, even in asymptomatic patients, to prevent or ameliorate cardiovascular morbidity and mortality. Studies consistently show that early detection and treatment of CRM risk factors lead to better outcomes. To improve understanding, the American Heart Association has characterized this syndrome into different stages: Stage 0 with no risk factors, Stage 1 with excess body fat, Stage 2 with metabolic risk factors and chronic kidney disease, Stage 3 with subclinical cardiovascular disease (CVD), and finally, Stage 4 with overt CVD in individuals with existing CKM risk factors. 2
Epidemiology of CRM
CRM encompasses a complex interplay of health conditions that synergistically heighten the risk of CVD, T2D, and CKD, all of which have significant incidence and prevalence across Europe.11,12 CVDs cause 42.5% of EU deaths. 13 Obesity14,15 and metabolic syndrome 16 promote CVD risk. T2D affects 61 million Europeans, projected to reach 67 million by 2030, with many undiagnosed or untreated.17,18 T2D often co-occurs with obesity and metabolic syndrome, linked to CVD and CKD,17,19 and contributes to their complications. 20 CKD affects 100 million Europeans and may be the fifth leading cause of death globally by 2040. 21 CKD increases mortality 21 and is an independent CVD risk factor, 22 worsening existing cardiovascular conditions. 23 Metabolic syndrome elevates CKD risk, with its components also increasing CVD risk.24,25 While obesity is linked to metabolic dysfunction-associated liver disease. 26
These conditions are locked in a vicious, bidirectional cycle (Figure 1). For example, while T2D is a risk factor for HF, HF can also contribute to T2D via increased insulin resistance, chronic inflammation, and endothelial dysfunction,27,28 while these inflammatory states heighten cardiovascular risk. 29 The neurohormonal activation and reduced physical activity in HF patients impair glucose utilization and insulin sensitivity.30,31 Similarly, diabetes mellitus is a leading cause of CKD through mechanisms like glomerular hyperfiltration and declining GFR, 32 and the presence of CKD in turn worsens T2D. 33 Finally, the heart-kidney connection is underscored by CKD being the greatest predictor for hospitalization in HF patients. 34 Additionally, hyperuricemia impacts renal disease and diabetes, its coexistence with diabetes synergistically raises the risk of all-cause mortality and end-stage renal disease (ESRD) in those with CKD.35,36 Awareness of these complex relationships is vital for effective prevention and treatment. 37
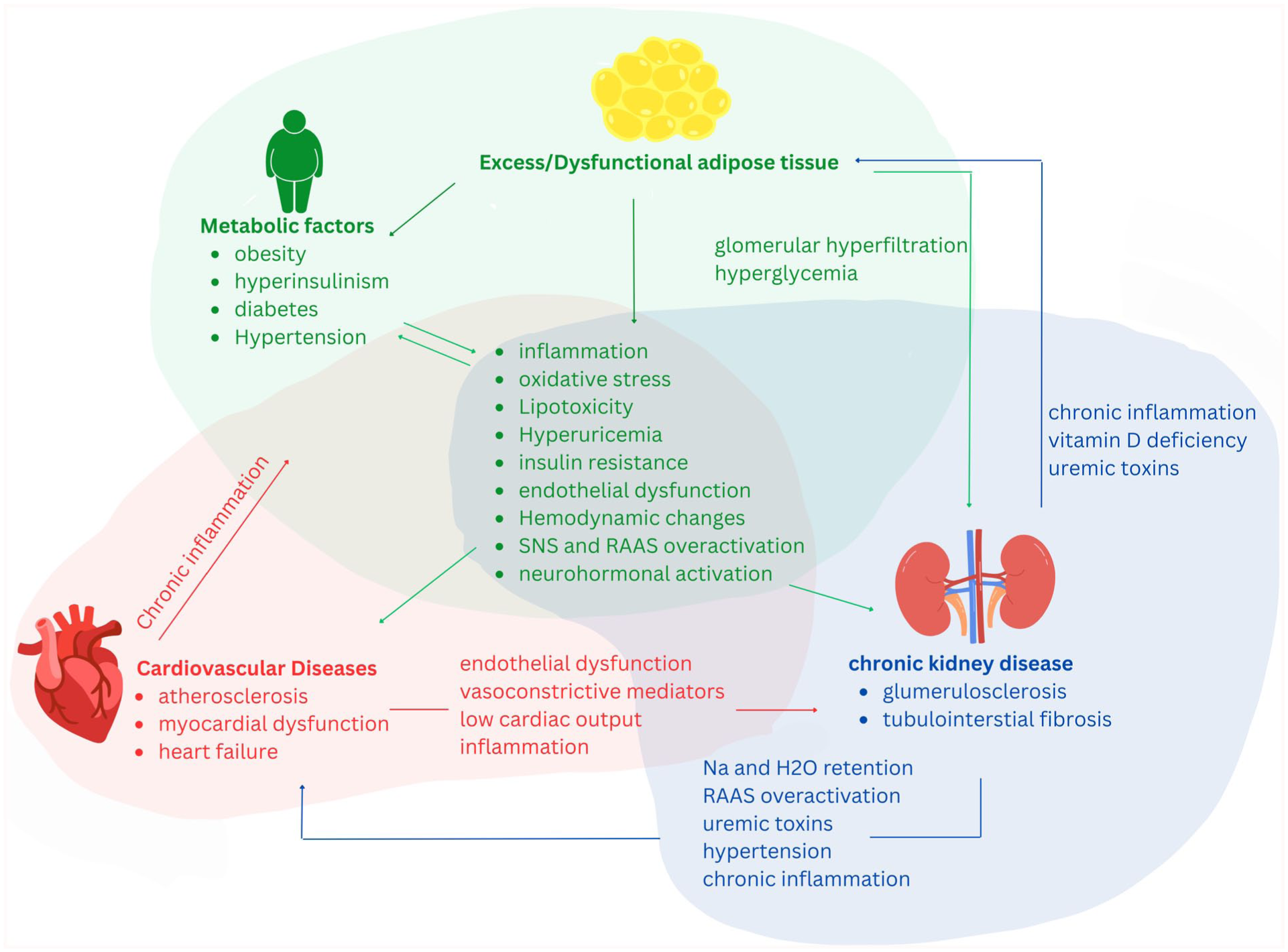
The interplay of excess adipose tissue, metabolic factors, cardiovascular, and kidney disease. Metabolic factors, including obesity, hyperinsulinism, diabetes, and hypertension, are linked to dysfunctional adipose tissue. These conditions trigger a cascade of systemic issues, such as inflammation, oxidative stress, lipotoxicity, insulin resistance, and activation of the sympathetic nervous and renin-angiotensin-aldosterone systems. This central pathological cluster simultaneously contributes to cardiovascular diseases, including atherosclerosis and heart failure, and chronic kidney disease, with glomerulosclerosis and tubulointerstitial fibrosis. The diagram emphasizes the central role of chronic inflammation, which creates a positive feedback loop that perpetuates damage in both the heart and kidneys, highlighting the interconnected and progressive nature of this multi-organ syndrome.
Determinants of CRM
The risk and progression of CRM are influenced by a complex interplay of factors beyond pathophysiology. Certain demographic groups, family history of diabetes or CKD, and lifestyle factors like sleep and mental health all contribute to elevated risk.7,38 -43 Women face unique risk factors due to hormonal impacts on cardiometabolic health. 44 Furthermore, early life exposures, such as maternal obesity or gestational diabetes, can have long-lasting effects on CRM predisposition.9,45,46 Additionally, chronic inflammatory conditions can increase CRM risk due to their contribution to both CVD and CKD. 47 Finally, social determinants of health (SDOH), encompassing factors like access to healthy food, safe housing, and quality healthcare, profoundly influence CRM risk by creating barriers to healthy lifestyle choices and disease management.48 -50 Table 1 shows a high prevalence of risk factors, which contribute to the high occurrence and incidence of CRM syndrome, posing a significant public health challenge.
Key Risk Factors for CVD, T2D, and CKD, Including Prevalence in Europe (Where Available), Association With Mortality, and Specific Disease Links.
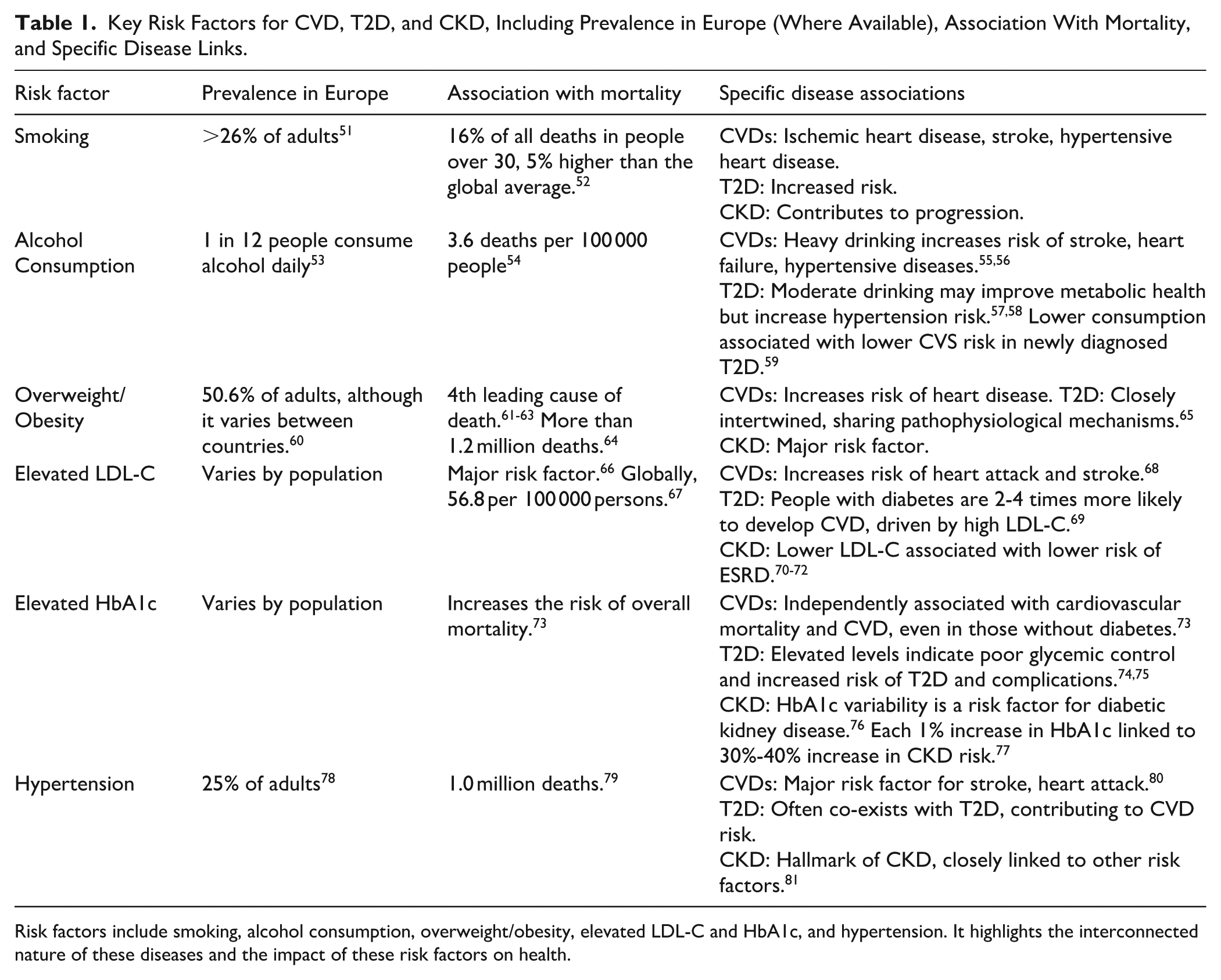
Risk factors include smoking, alcohol consumption, overweight/obesity, elevated LDL-C and HbA1c, and hypertension. It highlights the interconnected nature of these diseases and the impact of these risk factors on health.
Screening and Identification of High-Risk Groups
CRM is a significant public health concern in Europe and we propose that early identification of high-risk individuals is vital for effective intervention, improved health outcomes, and reducing the economic burden of CRM.
To this end, we suggest a progressive screening strategy is recommended to optimize PCPs’ efficacy. In this model, high-risk individuals should undergo annual assessments: BMI, waist circumference, blood pressure, fasting glucose, and a lipid panel (HDL-C, LDL-C, triglycerides).2,82 Tools like the ADA risk test and UKPDS risk engine refine risk stratification for future diabetes and guide interventions.83,84 Adults with early metabolic issues, such as excess weight, should be screened for metabolic syndrome. Adults with Stage >2 CKD need at least an annual kidney function assessment.85,86 The KDIGO heat map (Figure 2), using eGFR and albuminuria, stages CKD and guides personalized care. KDIGO recommends the Kidney Failure Risk Equation (KFRE) for kidney prognosis in individuals with eGFR < 60 ml/min, alongside other tools for comprehensive risk assessment.

CKD classification – KDIGO heat map: based on Albuminuria (A), GFR (G). Green – Low risk (if no other markers of kidney disease, no CKD). Yellow – Moderately increased risk. Orange – High risk. Red – Very high risk. 85
We propose that patients with metabolic dysregulation or renal dysfunction should undergo comprehensive cardiovascular risk assessment using scores like Framingham Risk Score, SCORE, or SCORE2.87 -89 CVD assessment also considers hypertension, coronary artery disease, HF, and stroke.90,91 Algorithms like H2FPEF and HFA-PEFF predict HF with preserved ejection fraction (HFpEF), often linked to T2D and CKD.91 -93 Advanced diagnostics, including CAC scoring, echocardiography, and biomarkers (BNP, NT-proBNP), are for those with elevated cardiovascular risk or specific symptoms.94 -97 CRM risk factors can begin pre-birth; maternal health, including obesity and hypertension, influences offspring risk via genomic imprinting. 47 This necessitates a life-course CRM screening approach, starting in childhood. Targeted lipid panels and glucose tolerance assessments are recommended for overweight or obese children at higher risk for T2D and metabolic dysfunction-associated steatotic liver disease. 2
Beyond biology, CRM health is significantly influenced by SDOH,98,99 contributing to disparities in cardiovascular health behaviors, CKD, and cardiovascular events and mortality.45,100 Various screening tools assess SDOH, covering financial strain, education, literacy, safety, mental health, physical activity, and substance use. 2 We believe interventions addressing adverse SDOH can improve CRM-related outcomes. 101
Management and Integration of Care in CRM Patients
We propose that effective CRM management requires early detection, comprehensive risk assessment, and holistic patient-centered care. As a summary of suggestions, Table 2 outlines a potential approach for achieving these goals. A crucial component of this approach is a management strategy that adapts to disease progression. This includes fundamental lifestyle modifications, followed by weight management (lifestyle changes, pharmacotherapy, and bariatric surgery as needed). 102 For patients with metabolic risk factors and CKD, we recommend comprehensive interventions, including cardiovascular risk optimization. 103 Intensified preventive measures with aggressive risk factor modification and targeted therapies are crucial for subclinical CVD and risk equivalents.104,105
Progressive Stages of CRM and a Framework for Clinical Intervention.

Outlined are management strategies, including lifestyle interventions, pharmacological therapies, treatment strategy, clinical guidelines, and the role of multidisciplinary specialists, tailored to each stage of CRM risk.
We suggest that pharmacological management is vital throughout the disease course, though not always indicated early. In a shift to a comprehensive CRM strategy, therapies like SGLT-2 inhibitors (SGLT-2i), glucagon-like peptide-1 receptor agonists (GLP-1-RAs), and RAAS inhibitors (RAASi) have become foundational. SGLT-2i are a cornerstone and can be considered first-line, as they improve glycemic control while providing cardiorenal protection by causing systemic and intrarenal hemodynamic changes.106 -108 Similarly, GLP-1-RAs offer significant benefits beyond blood sugar regulation, including weight management and powerful anti-atherogenic effects that manage cardiovascular and renal risk. 109 RAASi also play a critical role by managing blood pressure and offering robust cardio- and nephroprotection. 110 However, we recognize that while clinical trials and large databases validate the efficacy of these therapies, showing that combined use leads to greater reductions in mortality and heart failure hospitalizations, 111 their real-world applicability faces significant challenges. Patient adherence is often limited by side effects like gastrointestinal issues and genital infections, and cost remains a major barrier, particularly in low-income regions.111,112 These challenges must be addressed for these pharmacological suggestions to be widely adopted.
Patient education and self-management are critical, as is the treating physician’s awareness of all affected organ systems. PCPs are crucial in early detection, risk assessment, lifestyle counseling, initiating pharmacotherapy, and monitoring. They are the cornerstone of multidisciplinary CRM care, acting as a vital communication hub. Managing multiple CRM factors and selecting therapies requires careful consideration of individual patient characteristics, potential drug interactions, and adverse events.107,113 PCPs should integrate specialized care, ensuring therapeutic compatibility and minimizing polypharmacy risks. They are essential in collaboratively developing patient-centered, shared care plans, leveraging their comprehensive patient knowledge. 114 The PCP promotes interdisciplinary communication, coordinating referrals to specialists to ensure unified therapeutic objectives. Furthermore, they advocate for the patient, navigating the healthcare system and addressing needs. Continuous PCP care, including meticulous monitoring and adjustments, is paramount. A comprehensive Primary Health Care (PHC) team, beyond physicians, is essential for effective patient care.
Finally, we advocate for integrated care models to enhance CRM management by improving patient experiences and health outcomes. 115 These models often combine strategies like patient engagement, multi-professional collaboration, evidence-based clinical pathways, and aligned incentives. Successful integrated care models include case management, individual care planning, patient-centered medical homes, and personal health budgets.114,116 Sustainable transformation requires integrated care models to act at all health system levels: organizational, functional, professional, and service delivery.
Call for Action
Urgent, concerted action is needed across European healthcare systems to move beyond fragmented care to a comprehensive, integrated approach for CRM, improving patient outcomes. Implementing effective CRM syndrome management requires strategies tailored to the diverse realities of European healthcare, as national and regional systems vary significantly in their structures, funding, and resource access. 117 Social insurance models may create unequal access to new therapies due to different reimbursement policies, while tax-funded systems may face budget constraints.
The financial burden of CRM, driven by hospitalizations, necessitates cost-effective, early screening programs. While a complete, single dataset for all CRM conditions across Europe may be scarce, the available data on its individual components clearly demonstrates a significant and escalating economic burden. 118 The cost for cardiovascular disease alone was an estimated €282 billion in 2021, and this figure doesn’t account for the tens of billions of euros from chronic kidney disease and diabetes.119 -121 These costs are a major concern for healthcare systems, as they include not only direct medical expenses but also the significant indirect costs of informal care and lost productivity. A key strategy to mitigate these costs is to shift from reactive, in-hospital care to proactive, community-based prevention and management, leveraging digital health technologies and strengthening primary care.
Training for PCPs in Europe faces a number of practical challenges, including the lack of a standardized European training curriculum, with some countries emphasizing a general practice approach while others focus on a more holistic model.122,123 This inconsistency complicates professional mobility and can lead to variations in the quality of care. A "digital divide" also exists, as digital maturity varies widely among member states. While European healthcare IT infrastructure is moving toward an integrated and interoperable system—guided by initiatives like the European Health Data Space (EHDS)—this variation in digital access and maturity remains a barrier to advanced care.124 -126
Inconsistent guidelines from bodies such as the ESC, ADA, and KDIGO create clinical confusion and hinder effective patient management. For example, mandatory eGFR and uACR testing may be absent in standard primary care check-ups.127,128 Additionally, there is a lack of standardization in thresholds for NT-proBNP levels to indicate SGLT-2i cardioprotective treatment, as well as in HbA1c, eGFR, and uACR values for initiating treatment and specialist referral.129 -131 These inconsistencies, combined with other barriers, limit timely screening, diagnosis, and treatment. Additional challenges include restrictive indication criteria, prescription and reimbursement limitations for drug combinations (e.g., SGLT-2i and GLP-1 receptor agonists), and patient-related restrictions.128,130 These “artificial barriers” contradict evidence-based medicine and must be progressively removed.
To address these challenges, collaborative efforts are essential to develop contextually relevant, evidence-based solutions. A critical appraisal of key clinical and policy controversies, such as unequal access to therapies, is needed. The goal is to empower PCPs with the full capacity for CRM screening, diagnosis, and treatment initiation. Future research should focus on collecting primary data to quantify the local burden of CRM syndrome within specific healthcare systems. A comprehensive framework for addressing the challenges of CRM is outlined in Table 3, detailing key elements from primary care to research.
Therefore, we urgently call for the following actions:
A Framework for Addressing CRM: Outlining the Key Elements Involved in Primary Care, Prevention, Patient Care, Multidisciplinary Collaboration, Technology, Patient Engagement, Research, and the Challenges and Potential Solutions Associated With Each Area.
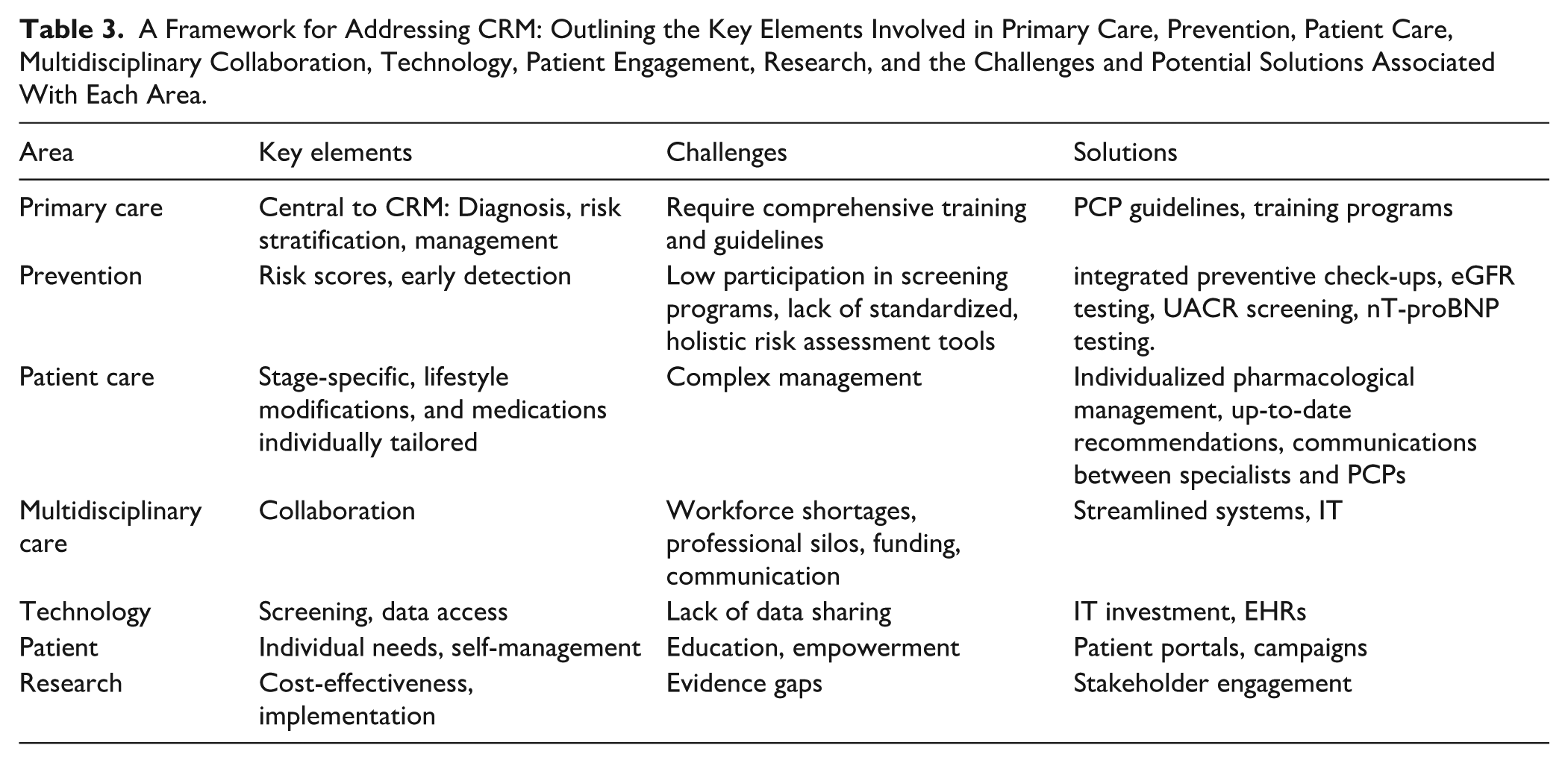
This call to action aims to be a catalyst for ongoing dialogue and collaboration among all stakeholders. We encourage policymakers, healthcare providers, patient advocacy groups, and researchers to collaborate in developing and implementing contextually relevant solutions. In Table 3, we propose a framework for addressing CRM, outlining key challenges and suggesting potential solutions. Only through collective effort can we effectively address CRM challenges and improve millions of European lives. We propose recommendations for PCPs to promote prevention, early detection, and a stage- and patient-specific approach to minimize disease progression and optimize outcomes, and a summary of these recommendations is visible in Figure 3.

Clinical approach to managing CRM syndrome: the key recommendations for developing guidelines to CRM syndrome begin with a risk assessment based on a scoring system that considers factors like age, BMI, and family history. This leads to a risk classification of low, moderate, or high. Next, a comprehensive patient evaluation and a series of laboratory investigations are conducted to gather essential diagnostic information. The final step, management, outlines a personalized treatment plan that combines lifestyle modifications, pharmacological therapy, and, when necessary, referrals to specialists. This systematic process is designed to help clinicians efficiently and accurately assess and manage patients with CRM syndrome.
Conclusion
The escalating public health and economic burden of CRM syndrome necessitates a fundamental shift in our healthcare approach. This manuscript has highlighted a critical deficiency: the absence of a unified, primary care-centric clinical guideline tailored to the diverse realities of European healthcare. This gap leads to fragmented care, delayed interventions, and suboptimal patient outcomes.
Our call for action is built on the core insight that proactive, integrated management is the most effective way to combat this complex condition. We have provided a detailed framework for achieving this, emphasizing the importance of empowering primary care physicians as central coordinators of care. The establishment of a new pan-European guideline must not only synthesize existing evidence but also confront real-world controversies, such as restrictive access to modern therapies and systemic barriers to implementation. By fostering a collaborative effort among all stakeholders, we can move from a reactive disease management model to a proactive, preventive, and patient-centered one, with the potential to transform patient care and alleviate immense economic strain on healthcare systems
Footnotes
Acknowledgements
MSci Claudia Dompe of Proper Medical Writing, Warsaw, Poland, provided assistance in writing, editorial support, and formatting assistance, which was contracted and funded by Boehringer Ingelheim.
Boehringer Ingelheim was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations. The study was supported and funded by Boehringer Ingelheim
Ethical Considerations
The article is a review of the literature and does not require ethical approval.
Author Contributions
M.S. Writing – original draft, Supervision; A.B. Writing – review & editing, Visualization; M.S. Writing – review & editing, Conceptualization; N.L. Writing – original draft, Supervision;
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.