
Abstract
Background:
Screening coverage for cervical cancer remains suboptimal in Flanders, Belgium. The upcoming transition to primary HPV screening in January 2025 presents an opportunity to offer self-sampling kits (SSKs) as an alternative to conventional Pap smears, with the potential to increase participation rates. General practitioners (GPs) can play a crucial role in reaching under-screened populations. Hereto it is essential to understand the needs and preferences of GPs regarding the integration of SSKs into their routine practice.
Methods:
Semi-structured interviews were conducted with GPs participating in an implementation study on the added value of SSKs for long-term non-screened women, focusing on their experiences, challenges, and suggestions regarding the provision of SSKs to these patients.
Results:
The interviewed GPs recognized the potential of SSKs to increase participation, particularly due to their less invasive nature, which makes them more acceptable to underscreened women. Time constraints, technical software challenges, limited knowledge and doubt about SSK accuracy were identified as key barriers to implement SSKs in routine practice. GPs emphasized the need for adaptability in the distribution methods of SSKs, with many preferring a combination of mailing the SSKs and providing them in person. Personalized communication and tailored explanations were considered as crucial to ensure patient acceptance and the correct use of the tests.
Conclusion:
This study shows that while GPs recognize the potential of SSKs to enhance cervical cancer screening, several challenges need to be addressed for their effective integration into primary care. A successful approach should incorporate streamlined support systems, tailored approaches to implement reminders for GPs and improved education for GPs. Future research should consider quantitative data on the effectiveness and cost-efficiency of SSKs in the specific context of Flanders and the perspectives of a broader range of stakeholders, including patients, practice nurses, gynecologists and policymakers, to develop more comprehensive strategies for the successful implementation of SSKs.
Keywords
Background
In 2020, the World Health Organization (WHO) launched its strategy to eliminate cervical cancer as a public health issue in the European Region. To fulfill this goal, vaccination uptake is important, alongside regular screening. 1 Early detection of cancer and precancer through screening enhances the decrease in incidence and mortality rates of cervical cancer.2,3 In Flanders, Belgium, the population-based cervical cancer screening (CCS) program is organized since 2013 by the regional screening organization, the Centre for Cancer Detection. The program invites women between 25 and 64 years old who did not have a cervical specimen taken in the last 3 years to have a smear taken by a healthcare provider. 4 Despite important efforts to reach all women in the target group, coverage remains suboptimal (64.5%). 5
Both patients and healthcare providers face barriers to CCS. The most common patient-related barriers toward CCS with a cervical specimen are insufficient access to information; negative emotional responses to the test including discomfort, embarrassment and fear; and logistical challenges, such as inconvenient healthcare locations or limited opening hours.6,7 These barriers contribute to low participation rates, especially for women in minority groups.8 -10 Since the effect of population-based CCS relies on the participation rates, 11 addressing these barriers is crucial. Moreover, from a fairness perspective, it is essential to ensure that every woman is able to attain the most optimal state of health. 12
Together with the launch of the strategy to eliminate cervical cancer, the WHO identified primary human papillomavirus (HPV) testing as the first-choice screening method for CCS. 1 Primary HPV testing demonstrates higher sensitivity to detecting cervical lesions than cervical cytology and is therefore more effective in reducing future cervical cancer at extended intervals.2,13 Samples for primary HPV testing can be collected by a healthcare provider by means of a cervical specimen or by the woman herself, using an self-sampling kit (SSK) for a vaginal specimen.14,15 A validated HPV DNA-test performed on a self-sample has a similar sensitivity and specificity as the same test performed on a cervical sample.14,15 The use of SSKs holds great potential to overcome patient-related barriers toward CCS by improving the acceptability and accessibility of CCS services.1,13 Women generally prefer self-sampling over healthcare provider-collected cervical specimens due to advantages like ease of use and increased privacy.10,16,17 In several European countries SSKs are used in the population-based CCS program. 18
A second strategy to increase CCS participation is the involvement of general practitioners (GPs).19,20 Because of their trusted relationship with the patient 21 and their understanding of patients’ broader contexts, GPs are well-positioned to provide a more patient-centered and supportive approach to screening.21 -23 However, GPs also face significant barriers regarding offering CCS, including high workloads, time constraints,21,22,24 difficult communication with the patient because of low CCS related health literacy and language proficiency,21,24 incorrect beliefs or insufficient knowledge about CCS, the absence of an accurate recall and reminder system, and difficulties in tracking patients’ screening status.22,25
To investigate the impact of reducing barriers encountered by patients as well as by GP, we set up a randomized controlled trial (RCT) in 2022, named “the ESSAG trial” (Efficacy of offering a Self-SAmpling device by the General practitioner to reach women underscreened in the routine cervical cancer screening program). The trial consisted of several interventions, including (1) utilizing SSKs (Evalyn Brush®, Rovers Medical Devices, B.V., Oss, Netherlands), (2) engaging GPs as key participants, and (3) incorporating tailored and accessible informational materials. In the first intervention, GPs informed long-term non-screened women consulting for any reason about CCS, using accessible, tailored informational materials and offering an SSK. In the second intervention, eligible women received a personalized letter from their GP at home, which included accessible information and an SSK. The detailed protocol of the ESSAG trial is described elsewhere. 26 The RCT ran from September 2023 to February 2024, involving 139 GPs from 48 practices across the Flemish region, aiming to include 1125 long-term non-screened patients in each arm over 6 months.
This paper reports the findings of a qualitative study that was set up alongside the ESSAG trial. The study aims to explore the needs and preferences about the different challenges the GPs participating in the first intervention of the ESSAG trial encountered, which aspects of the intervention they considered as efficient and effective, their needs, and their recommendations for changes. This study aims to fill the gap in knowledge about how GPs should be supported in offering SSKs for CCS in their practice, particularly in European healthcare settings. By exploring ways to effectively support GPs in integrating SSKs into their practice, this research provides insights into the practical application of SSKs and identifies strategies that could enhance participation in CCS through primary care. Such findings may contribute to a more patient-centered and accessible approach to screening, helping to realize the WHO’s public health goal of eliminating cervical cancer.
Method
The needs and preferences of GPs are explored through a qualitative approach using semi-structured interviews, to facilitate an in-depth understanding.
Sampling
All GPs from 48 practices who participated in the first RCT intervention were eligible for participation in this study. In the last week of the RCT intervention period, they were all invited by email and telephone. We strived for maximum variation among the participants, by undertaking additional efforts to include GPs who were less reactive to our initial invitation (ie, male GPs, GPs working in solo or duo practices, as opposed to group practices, and GPs from practices who recruited a very low number of women). Interviews continued until data saturation was reached, at which point the researchers felt no new information was found during the last interviews.
Data Collection
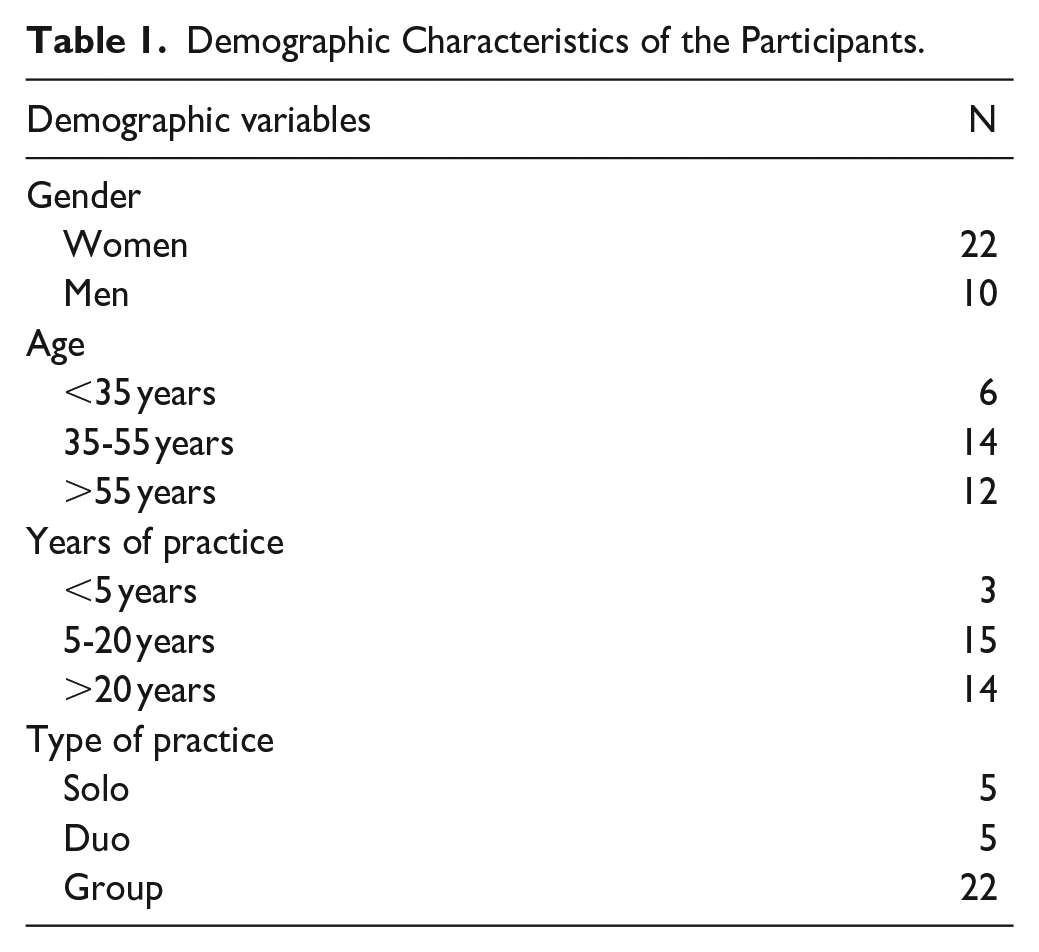
The semi-structured interviews took place online, using Microsoft Office Teams software because of practical considerations. Prior to the interview, demographic information was collected (see Table 1). An interview guide was developed and employed to allow consistency across interviews, while at the same time offering flexibility to allow GPs to raise issues that they felt were prominent. The research team developed the interview guide based on a review of the literature, supplemented with insights gained during the RCT intervention period and feedback from GPs during that time (see Supplemental Material 1). The first two interviews were conducted as pilots to assess the clarity and completeness of the questions. Since the questions proved to be clear and comprehensive, no further revisions to the interview guide were required. The interviews were conducted in Dutch, and were carried out between March 2024 and June 2024. All interviews were video-recorded. Consent was provided by all participants prior to the interviews.
Demographic Characteristics of the Participants.
Data Analysis
Interview data were transcribed verbatim, pseudonymized, and analyzed iteratively using Braun and Clarck’s 6-phase thematic analysis approach. 27 NVivo (QSR International Pty Ltd., Version 12) was used as analyzing tool. In a first step, EG, KVR, and LK entered a process of data immersion by reading and re-reading the transcripts of the first three interviews to enhance data familiarity. To generate the initial codes, EG, KVR, and LK independently coded these three transcripts. After discussing the codes and creating a common coding tree, another two interviews were coded by the three researchers. The final codes were agreed on through discussion and a final codebook was developed. The subsequent transcripts were inductively and systematically coded by EG and LK. Transcripts were examined regularly with KVR to review emerging codes and refine the analysis. In each phase, discrepancies were discussed until consensus was reached. The final codes were then structured into overarching themes, aiming to evaluate the feasibility of active GP involvement in CCS. The three overarching themes that emerged were (1) barriers the participating GPs encountered; (2) GPs needs with regard to taking an active role in offering SSKs to long-term non-screened women; and (3) their preferences regarding their role in CCS. Quotations were selected to illustrate some of the results and translated by a bilingual Dutch-English-speaking researcher. The video recordings of the interviews were deleted after transcription. Internal validity was ensured by researcher triangulation. 28 To further ensure the quality of the analysis, the emerging analysis was presented and discussed with the entire research team.
Results
Characteristics of the Participants
In total, 32 GPs from 28 different practices participated in an interview, with an interview length ranging from 10 to 64 minutes (average length was 36.43 minutes). The demographic characteristics of the sample are set out below in Table 1. Most of the GPs were women (68.8%), the mean age was 48 years (range = 28-68 years), and the majority were employed in group practices (68.8%). The length of their professional experience in primary care varied from 0 to 43 years (mean = 19 years).
Barriers Encountered by GPs in Offering an SSK During Regular Consultations
Overall, most of the participating GPs were positive about the potential of offering SSKs, mainly because they saw the benefits for both them and their patients. The GPs perceived the SSKs as an easy and efficient way to discuss and offer CCS during regular consultations and received positive feedback from most patients. Patients responded positively to the convenience of self-testing, which lowered the barrier for participation, especially for individuals who might not regularly engage in traditional CCS. Although most GPs expressed general enthusiasm for participation in the trial and offering the intervention, some barely introduced the topic of CCS to their patients due to various challenges (see Figure 1).

Barriers encountered by GPs in offering an SSK during regular consultations.
The most frequently cited challenge was a lack of time. Consultations often ran late due to a full waiting room or lengthy appointments or were disrupted by unexpected phone calls, leaving little opportunity to address additional issues. The overall busyness of the practice (eg, administrative burden, staff shortage, and vaccinations), particularly during the winter months, also played a role. This often forced GPs to prioritize and sometimes skip certain tasks, such as prevention. In addition to time constraints, some GPs simply forgot to offer the intervention to the patient despite the reminder in the medical record. Another significant factor influencing the decision to offer an SSK was the patient’s mental and/or physical condition. When patients were dealing with serious psychological problems, physical conditions, or emotional strain, GPs often found it inappropriate to discuss preventive examinations. GPs, therefore, sometimes postponed preventive investigations to a subsequent consultation.
GP14: “That’s when I think: ‘That is a patient that I will surely see in three months-time, so I will bring up the topic then.’ If I was behind with time, then this would happen more frequently.”
The social context of the consultation was also an important influencing factor. When others, such as children or partners, were present, discussing sensitive topics like CCS was often avoided.
GP6: “If I was very short on time then I just skipped it, or if there were a lot of people joining the consultation, such as their children, then, yeah, then I would not.”
Furthermore, GPs’ engagement with the trial was also influenced by having different interests and priorities, a lack of familiarity and routine with the new procedure, and insufficient confidence and knowledge to explain the topic. Additionally, they faced technical challenges with software modifications, which allowed GPs to generate lists of long-term non-screened women and implement a notification that reminded them of CCS in the medical records of their long-term non-screened patients. These challenges also reflected in GPs reference to their colleagues’ lack of engagement.
GP31: “Because that does not interest him [a male GP colleague], actually at all (. . .) I do not know if he is that conscious of it (. . .) He’s mostly involved in sports [medicine].”
GPs’ Needs Regarding Offering SSKs for CCS in Their Practice
Several barriers described by GPs can be translated into specific needs related to offering SSKs during consultations (for an overview of the needs, see Figure 2). In the ESSAG trial, we anticipated some of the barriers GPs might face in delivering the intervention. Strategies to address these challenges and respond to the needs we had already identified were incorporated in the RCT design. However, other needs emerged only during the interviews. The following sections explore these needs, focusing on how addressing them can assist GPs in incorporating SSKs into their routine practice more effectively and improve patient participation in the screening program.

GPs’ needs regarding offering SSKs for CCS in their practice.
Need for Support to Identify Long-term Non-screened Women
In Flanders, due to a lack of systematic registration of the screening status in patients’ medical records, GPs could not easily identify long-term non-screened women. Therefore, in the trial, we anticipated the need for support to identify these patients by implementing several proactive measures. First, the Centre for Cancer Detection informed GPs about their patients’ last screening dates by sending structured messages to the patient’s medical records. Additionally, the set-up of software modifications enabled GPs to generate lists of long-term non-screened women, clearly identifying those who require screening.
GPs experienced improved efficiency and time-saving, once the systems were introduced. This reduced search efforts and improved the accuracy of patients’ medical records, making it easier to advise and follow up with patients.
GP2: “You can also see it much quicker now. Previously, it was sometimes a matter of looking whether it was in the documents section or the lab results section. Now I know, it is in one place. This is a very big difference. Also, if we were not the ordering healthcare provider, then it [the test result] would not always come straight to our medical records, but now it does. Now we have a more complete overview.”
Moreover, several GPs noted that the study made them more aware of the need to discuss CCS with their patients and even encouraged some GPs to pay more attention to preventive care with their patients, in general. Some indicated that this increased consciousness would continue beyond the study. They found it very revealing to see the number of long-term non-screened women in their practice, highlighting the need to prioritize CCS.
GP10: “When I finally got the list then (. . .) it was a real eye opener like wow, we thought we were doing well in our practice with CCS and then actually, not so much."
Nevertheless, the implementation of these measures faced several challenges. Technical issues impacted their effectiveness. The information that was provided to the GPs was not always up-to-date or reliable, which sometimes led to confusion, extra work and even frustration. Some GPs were also confronted with an overload of information, as data from the Centre for Cancer Detection sometimes arrived in bulk, overwhelming the GPs.
GP31: “The most annoying thing was actually, the results, well, the date of the cervical specimens we received. That was a lot. We received some twice, or three times from the same person as well.”
Furthermore, some practices required more support than others in order to effectively perform the software modifications. Some GPs labeling themselves as not being very “IT-minded,” did not get around running the audit, causing them to neglect their participation in the project.
GP20: “I am not really a computer person (. . .) I am not really computer-minded (. . .) that first time is always a step for me. Always. That is not because it was very difficult or anything. That is just me not being computer-minded. That is just me. Nothing other than that.”
Need for a Reminder System When Long-term Non-screened Women Consult
We aimed to support GPs in remembering to bring up the topic of CCS during a consultation with a long-term non-screened patient. This was done by implementing a reminder system integrated into the scheduling module of the medical records. Apart from being a useful reminder system, it also proved to serve as a helpful tool to seamlessly integrate the topic of CCS into the consultation.
GP12: “It was good that there was a reminder in the patient file, because then you think about it more easily.”
GP17: “That is just also a very convenient way to bring it up like: ‘Oh, I am getting a reminder here that it is time for your cervical specimen, could that be right?’ (. . .) You can hardly not notice it. I was able to bring it up very quickly. (. . .) I found that helpful.”
Nevertheless, if GPs assessed that the circumstances were not appropriate, they often decided to postpone the discussion and bring it up during a more convenient consultation at a later time. This finding highlights the importance of a reminder that persists until CCS has been addressed.
Despite the reminders, GPs mentioned that there still were situations in which they forgot to discuss the topic. They felt that the reminders were not always visible enough or that they were displayed under the wrong section. Several suggestions were made for more eye-catching pop-ups that appear automatically when they open a patient’s record, and requiring active closing, for example, in order to reduce the likelihood of missed alerts.
GP6: “I used to work with another program and that pop-up, it really opened up [on the screen] like a proper pop-up when you opened the file. I found it to be more visible that way. Now, it is in the dashboard but if you do not look for it and instead immediately start opening a new consultation, then you have managed to overlook it, have you not?”
Finally, some GPs struggled to get used to check the reminders in the patients’ medical record and found it challenging to change their habits.
GP9: “It is also not quite familiar yet. It is not yet in my routine to check it. And, then that also goes back to the background very quickly if you do not have eligible patients for a few days, then you also forget to check or think about it.”
Need for Optimal Instruction of GPs
Considering that primary HPV testing and the use of SSKs is new for Flemish GPs and that the current focus is still on primary cytology, it seemed essential to properly inform the GPs and support them in implementing this new procedure in their practice. To achieve this, we provided comprehensive information for GPs via email and we visited practices to present the information and study protocol as thoroughly as possible. The research team suspected that some practices might need more encouragement than others to effectively engage patients in CCS. Therefore, we regularly contacted all practices to check how the intervention was going, if they had any questions, encountered difficulties, or needed support. This monitoring revealed that while some practices quickly started offering the SSKs, others were slower to begin.
Despite our efforts to adequately inform the GPs, it became evident that this was not always sufficient for all GPs. The interviews revealed that there were misunderstandings and misconceptions toward primary HPV testing in general, on the one hand, and toward the study protocol, on the other. For example, some GPs expressed doubts about the reliability of the test or had incorrect beliefs about the time interval for primary HPV testing. These concerns persisted even though they were addressed, supported by relevant scientific sources during the preparatory in-person practice visit. GPs who missed some of the information, felt less prepared and uncertain about the procedures and this was mentioned as a barrier to start offering the SSKs.
GP16: “I actually did not properly introduce it. So I never recommended it to my patients, actually because I did not trust I knew enough about it.”
It appeared that some information was simply forgotten or never reached the GPs who were not present at the practice visit. Nonetheless, several other GPs mentioned that once they were familiar with the procedure, it became continuously more straightforward. Some GPs themselves suggested that reminding them about CCS during less busy periods, such as during spring time could be beneficial.
Need for Information Materials to Assist in Explaining the Screening Procedure to Long-term Non-screened Patients
To further support the GPs in offering the SSKs to their patients, we provided a package that included an invitation letter, a brochure written in accessible language style, an SSK, and a pre-paid envelop. Additionally, web links to an instructional video and translated materials were available, along with pictograms to help GPs explain the procedure to non-native speakers or women with a lower educational background.
GPs reported that they mainly focused on practical explanations and demonstrations during the consultation. This involved actively opening and going over the detailed information package (especially the step-by-step guide at the back of the brochure) and demonstrating the procedures with a demo brush. Many GPs considered these steps essential for their patients’ understanding and acceptance of the procedures and appreciated the provided materials.
GP18: “I then immediately took out an envelope and I unfolded the detailed information package and I explained how it worked. I then showed the first page with the visual (. . .) so, actually I just turned the booklet over with the visual to show them (. . .) then I also took out my demo model once to show, yes, that was necessary to really show it visually (. . .) I do not think that would have gone so well without it.”
The other provided materials, a video and the pictograms, were used only sporadically by some GPs, mainly in the early stages of the trial. The translated materials were also used less frequently. According to the GPs, this was due to a low number of non-native speaking patients. GPs frequently mentioned that mass media campaigns would significantly assist in discussing the screening program with their patients and that familiarization would be helpful in the first years.
GP16: “I would maybe launch a media campaign, first and foremost. To sensitize people and to inform them beforehand on the possibilities [within CCS]. To encourage them to do it, and to leave them with the choice.”
Need for Support in Follow-up of Patients
Correct follow-up of patients included two aspects. The first implies the need for a tracking system that indicates whether the patient has mailed her sample to the laboratory. Simply providing an SSK did not ensure completion of the test, highlighting the necessity for a systematic follow-up tool. Such a tool would enable GPs to monitor patient compliance effectively and provide reminders during subsequent consultations when necessary.
The second aspect of follow-up involves managing the process after receiving the test results. In this study, GPs received support in the form of a flowchart outlining the necessary steps following a positive high-risk HPV test. The details of this process are reported in the protocol. 26 Due to GDPR restrictions, the protocol allowed for the communication of the test results only to the GP, not directly to the patient, which was noted as a limitation by the GPs.
GP22: “It is not easy now to see those who remain – ok, we have given it to them to take home, but there are no lab results. We closed the reminder when we gave the test, but you have to actively look into the previous consultation notes to see ‘Yes, I have given her the test to take home but nothing came of it.’ So, therefore the follow-up should be incorporated into the medical software we use. So that the reminder only disappears once we receive a result.”
GP15: “If it is more clearly shown, I will want to speak to them about it because I will think, ‘actually, you have not brought it back yet.’ That is no trouble, but then I would want to see it directly in the patient’s file.”
Need for Financial Support
Given that the literature identified financial incentives as motivating factors for GPs, and anticipating that recruiting practices would be challenging due to the time investment required, we decided to provide a financial incentive. We opted for an incentive per patient addressed rather than per SSK distributed in order to prioritize informed choice to participation in the screening. Opinions on the financial support varied, but most GPs viewed the compensation as an extra incentive rather than a primary motivator. Many GPs were primarily motivated by the intrinsic value of the study and the alignment with existing professional responsibilities. Nonetheless, financial incentives could still help some GPs pay more attention to prevention.
GP2: “I think that is a nice bonus, but personally, I do not do it for that. I mostly want to have more tools to help with prevention. But I do in fact think it is a nice bonus for some, in order to get an extra boost.”
GPs’ Preferences Regarding Their Role in CCS
In addition to highlighting their needs related to CCS, GPs also shared their preferences regarding their own role in the process.
Preferences With Regard to Screening Methods for Cervical Cancer
The majority of GPs supported the use of SSKs as a primary screening tool. They experienced advantages for both the GP and the patient. The SSK lowers the threshold for GPs to invite patients to participate, as it eliminates the need for a clinical examination, resulting in time-saving. However, GPs also stressed the importance of discussing other gynecological complaints or problems, such as pain during intercourse or sexually transmitted diseases, when offering the SSK. The less invasive nature of the SSK was particularly valued, as GPs believed that this increases willingness to participate, especially among hard-to-reach groups and women who refuse a traditional cervical specimen.
GP8: “It is less time-consuming than a cervical specimen. It is less invasive for the patient. They can do it perfectly from home. I mean, I think that we put in much more time when taking cervical specimens than we would with this. Even the coding [referring to all software modifications that were needed] and the follow-up, I mean. Yes, in my opinion this can be directly rolled out.”
However, some GPs preferred the traditional cervical specimen due to concerns about missing clinical and visual inspection opportunities with SSKs. They viewed the SSK only as a good alternative if the patient is not open to a cervical specimen. Another reason for preferring the traditional cervical specimen was doubt about the effectiveness of the self-sampling test, stemming from limited knowledge about its accuracy. Other participants seemed to prefer offering both options and, consequently, placing the choice with the patient.
GP2: “I would still give preference to a cervical specimen taken by a healthcare provider, how we know it, either by us [as GPs] or by a gynecologist. Why? Because the visual aspect is also still important when it comes to gynecological assessments. Then you see a lot, such as polyps for example. I mean, because, you understand, you miss out on that with the SSKs, but, there are still patients who will refuse such things [i.e., cervical specimens taken by a healthcare provider], because they do not like undergoing them, in which case I would, in a second instance, offer the SSK.”
Preferences With Regard to the Organization Strategy When Using SSKs
GPs had different ideas about how SSKs for CCS should be offered to patients. Some GPs considered mailing SSKs as an effective method to reach a broader audience, particularly those without a regular GP or with infrequent consultations. They compared it with the system used for colorectal cancer screening (in which fecal immunochemical test are mailed), noting benefits in terms of outreach and workload reduction. Additionally, the anonymity of the process could be advantageous, as some patients are uncomfortable with face-to-face interactions for such tests. Personalized letters, signed by the GP (in contrast to letters sent by the Centre for Cancer Detection) were mentioned as a way to increase the actual response rate. However, concerns existed about its effectiveness and logistical challenges, such as tests going unused and GPs not obtaining results correctly. Some GPs doubted whether sending tests without personal explanations is as effective as offering them in person, fearing many people would discard the tests.
GP16: “Both [distribution via mail or in person by the GP] can work, actually, but I think it is nice if people can take ownership and, in the first instance, decide for themselves if they would want to participate or not. After they have been informed, naturally.”
Conversely, most participating GPs stated that it would be feasible to offer SSKs in person at their practices, provided there is sufficient support and adjustments as provided during the ESSAG trial (eg, easy software modifications to identify long-term non-screened patients, and accessible information materials). They emphasized the importance of personal contact with the patient and the opportunity to provide clear explanations to ensure acceptance and correct performance of the test. Many GPs saw this as an effective way to increase participation in CCS, especially among patients reluctant to undergo a traditional cervical specimen.
GP8: “If they would send this without any explanation, I think that a lot of people would not deal with it because it looks a bit invasive at first glance.”
GPs expressed a need for flexibility and a variety of distribution models to effectively reach a broad range of patients and to foster patient-centered care. Many GPs found a combination of both methods (mailing and personal delivery) to be the most effective approach. For example, it was suggested several times that all eligible women should receive an SSK via mail, while practices should also have spare kits for women who did not respond to the mailed kit. The reminder procedure from colorectal cancer screening in which GPs receive a reminder from the Centre for Cancer Detection when a patient did not respond to a mailed kit twice, was often suggested in this context.
GP1: “I think it would be more interesting if it were complementary. I think we [GPs] should also be able to provide these SSKs. So the two should be able to co-exist. If we see that it does not happen [the woman does not send back the SSK that was mailed], we can speak to the patient about it, and then she could say ‘Yes, I do find it interesting.’ It should be possible to immediately provide an SSK instead of them having to wait for it to be mailed to them again.”
Discussion
This study provides detailed insights into the needs and preferences of GPs who provided SSKs in CCS within the national screening program in Flanders. Moreover, it also provides actionable insights for improving the practical implementation of SSKs in primary care. These findings are especially timely given the rollout of primary HPV screening across Flanders. 29
The positive reception of SSKs among GPs, driven by perceived benefits for both healthcare providers and patients, aligns with international literature.25,30 However, several barriers significantly affected the GPs’ ability to consistently offer SSKs. These challenges may have contributed to the strong variation between GPs with regard to the number of SSKs that were distributed to eligible women.
The most significant barrier identified in this study was experiencing time constraints, consistent with previous findings that GPs often prioritize acute care over preventive measures like CCS due to limited time during consultations.21,24 To mitigate this, a “whole-of-practice” approach that redistributes the workload among healthcare staff may help. 31 In particular, involving practice nurses could be a practical solution.22,32 GPs largely appreciated the introduction of reminders in the medical records; however, it remains important to adopt tailored approaches to implement these reminders-such as through customizable systems developed by software providers- effectively to ensure that offering SSKs is not overlooked and that reminders seamlessly integrate into individual daily workflows.21,33 A persistent challenge, common to this study and others, is the identification of long-term non-screened women. While technical difficulties in accessing screening records were noted, GPs appreciated the improvements made, suggesting that further refinement and optimalization of user-friendly health record systems and exchange of information between involved parties could strengthen GPs’ engagement in addressing CCS with their patients and improve the overall efficiency of offering CCS in primary care.22,25
Comprehensive, tailored information, and communication to help GPs familiarize themselves with SSKs emerged as essential components, along with ongoing education on the validity of self-collected samples. Addressing concerns about the reliability of SSKs is crucial in the future to enhance the GPs’ confidence,30,33,34 particularly as evidence shows that validated HPV tests on self-samples are as accurate as healthcare provider-collected tests. 14 Consistent with international literature, additional strategies, such as national media campaigns, are also needed to raise awareness and improve participation in cervical cancer screening programs. 30
In contrast to other studies,33,35 GPs expressed no need for multilingual and culturally appropriate materials in our study. This may be attributed to a low number of non-native or non-English/French speaking patients consulting the GP, as highlighted in the results, causing less need for the translated materials. This can suggest that the demand for such materials may be context-dependent.
While the GPs in the present study expressed few concerns about managing HPV-positive results, other studies have highlighted this as a significant concern among GPs.25,30,36,37 The absence of these concerns in this study likely reflects the effectiveness of the provided flowcharts, implying that clear and structured follow-up guidelines can help reduce clinical challenges. A recent review 31 supports the current study’s insight that, although financial incentives might provide modest supplementary motivation for some GPs, other strategies may be more important in boosting GPs’ enthusiasm to discuss CCS with their patients.
In terms of distribution, GPs expressed various preferences, with some favoring a mail-based approach similar to colorectal cancer screening in Flanders, while others preferred offering SSKs in the GP practice. Most GPs were supportive of offering SSKs in the GP practice, provided there is sufficient support and adjustments, such as those implemented during the ESSAG trial. They valued the importance of personal contact and clear communication to ensure patients’ comfort and correct test use, similar to findings by Le Goff et al. 34 Additionally, other international studies confirm that healthcare providers find SSKs compatible with existing workflows and practical to integrate into routine care.33,38 A meta-analysis by Costa et al 39 found that while all self-sampling distribution methods are more effective than conventional invitation letters encouraging women to have a cervical specimen taken by a healthcare provider, face-to-face invitations continue to result in the highest participation rates. These mixed views suggest that a one-size-fits-all approach may not be effective, and adaptability in the distribution models is essential to meet different patient needs. Integrating both strategies—mailing SSKs to all eligible women while also allowing GPs to provide kits in their practices—may be the most effective approach for maximizing participation. From a logistical perspective, this could be implemented in a manner similar to the current process for colon cancer screening in Flanders: GPs can easily order kits from the Center for Cancer Detection to distribute in their practices. However, while GPs may find this approach ideal from a public health perspective, it could pose significant challenges in terms of cost and sustainability. The increased resource consumption, alongside the potential for higher costs, suggest that a balance between public health goals, ecological impact, and economic feasibility must be carefully considered.
Strengths and Limitations
This study was conducted using purposive sampling, which, while useful for gaining initial insights, may have led to selection bias. GPs who participated may have had a stronger interest in preventive care or may have been more positively inclined toward SSKs, potentially limiting the applicability of the findings. However, considerable effort was made to ensure heterogeneity in the sample, as GPs from 28 different practices across all 5 Flemish regions were included. This diversity enhances the applicability of our findings to a broad range of practices in Flanders. Additionally, the focus on GPs with direct experience of distributing SSKs allowed for in-depth perspectives, avoiding speculative opinions. A limitation is that the study explored patient experiences only indirectly, through the lens of GPs. Nevertheless, prior research in Flanders has shown positive patient reception toward SSKs.40,41
Future Research
Future research should aim to gather perspectives from a diverse range of stakeholders, including government officials, clinical service administrators, practice nurses, gynecologists, laboratory personnel, community members, and women, to ensure a comprehensive understanding of the challenges and opportunities related to CCS with SSKs. Additionally, exploring the perspectives of GPs who are less involved in preventive care or hold more neutral or negative views on SSKs, would provide valuable insights. Such an approach will help identify the most effective strategies for implementing CCS into daily practice in Belgium (Flanders). Quantitative studies on the cost-effectiveness and clinical outcomes of SSKs in Flanders could further complement this qualitative work, providing a holistic view of how to optimize CCS strategies and improve screening outcomes for diverse populations.
Conclusion
The findings of this study indicate that GPs generally have a positive attitude toward offering SSKs for CCS in their practices, recognizing the benefits for both healthcare providers and patients. However, they face several barriers, including time constraints, technical difficulties, and a lack of knowledge regarding the reliability of SSKs. An integrated, tailored approach—combining software-based support systems, targeted education, appropriate materials for patients enhanced with national media campaigns and adaptable distribution methods—is essential to ensure that SSKs can be effectively incorporated into primary care. However, these conclusions should be interpreted with caution since the participating GPs may have been more engaged in preventive care or had a more favorable view toward SSKs, which could limit broader applicability of the findings. Nevertheless, improving participation in CCS through tailored approaches could ultimately enhance public health outcomes and contribute to the success of the national CCS program.
Supplemental Material
sj-pdf-1-jpc-10.1177_21501319251320178 – Supplemental material for General Practitioners’ Needs and Preferences Regarding the Provision of Self-sampling Tests for Cervical Cancer Screening in Flanders, Belgium
Supplemental material, sj-pdf-1-jpc-10.1177_21501319251320178 for General Practitioners’ Needs and Preferences Regarding the Provision of Self-sampling Tests for Cervical Cancer Screening in Flanders, Belgium by Eva Gezels, Sara Willems, Katrien Vanthomme, Lien Keersse and Kaatje Van Roy in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors thank the general practitioners who were willing to participate in the interviews.
Author Contributions
EG: conceptualization, methodology, formal analysis, investigation, data curation, writing (original, review/editing), visualization, supervision, and project administration; SW: conceptualization, methodology, writing (review/editing), and funding acquisition; KV: conceptualization and writing (review/editing); LK: data curation and writing (review/editing); KVR: conceptualization, methodology, data curation, writing (review/editing), and funding acquisition. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The ESSAG trial is funded by Kom op tegen Kanker (Stand up to Cancer), the Flemish Cancer Society (project ID: 12343). The funder has no involvement in any part of the project. This manuscript is published with the support of the University Foundation of Belgium.
Ethical Approval and Consent to Participate
The ESSAG project was approved by the Research Ethics Committee of Ghent University Hospital (nr. ONZ-2022-0250) and the Information Security Committee (nr. 22/258). Participation was voluntary and oral consent was provided by all the participants prior to the interview. GPs received no financial incentive for participating in the interviews.
Consent for Publication
Not applicable.
Clinical Trial Number
ClinicalTrials.gov: NCT05656976.
Supplemental Material
Supplemental material for this article is available online.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.