
Abstract
Introduction:
Eye health is an increasing concern among older populations dwelling in the community. Promoting positive eye health behaviors is essential not only for maintaining vision but also for preventing avoidable blindness. Understanding the factors that influence these behaviors is crucial for developing effective and sustainable interventions.
Objectives:
This descriptive qualitative study explored key stakeholders’ perspectives on improving eye health behaviors among older persons in a Thai community, using the PRECEDE model as a framework. The findings offer insights into contextual factors that can guide the development of culturally appropriate and sustainable interventions.
Methods:
This descriptive qualitative study was conducted using focus group discussions with 8 key stakeholders involved in primary eye care services. Participants were purposively selected to provide diverse perspectives on eye health behaviors including primary eye care services among older persons in the community. Data from the focus groups were audio-recorded, transcribed verbatim, and analyzed using thematic analysis to identify key factors influencing eye health practices. The reliability of the research instrument, based on the constructs of the PRECEDE model, was tested by calculating the Index of Item-Objective Congruence (IOC). To ensure trustworthiness, credibility was enhanced through prolonged engagement and member checking. Transferability was supported by clear descriptions of the context and participants. Dependability was addressed by maintaining an audit trail, and confirmability was ensured through reflexive journaling and peer discussions to reduce bias.
Results:
Analysis of the focus group discussions, guided by the PRECEDE model to identify administrative and policy factors and align interventions, revealed 4 key themes influencing eye health behaviors among older persons. These themes emerged from 4 main categories, which were derived from 10 main categories, 17 subcategories, and 26 corresponding codes: current policy, problems and obstacles, suggestions and needs, and resource management. The first theme emphasized primary eye care efforts, including vision screening for cataracts and glaucoma by ophthalmologists in cooperation with private hospitals. Cataract surgeries are funded by the National Health Security Office and state welfare, alongside a program providing prescription glasses to those aged 60 years and over. The second theme addressed financial barriers for older persons, who frequently pay for eye health beyond government support. Participants noted policy gaps and emphasized the need for careful planning and timely funding. Human resource issues, such as staff burnout and limited training of village health volunteers, were also identified as factors affecting service quality and screening accuracy. The third theme involved stakeholder engagement, where participants noted unclear roles limiting collaboration and emphasized the need for stronger social support. Despite these challenges, they highlighted the value of community engagement and proposed solutions such as eye health education for older persons, training village health volunteers in prevention and vision screening, and strengthening intersectoral collaboration. Finally, effective resource management was highlighted as essential to support the eye health promotion program, encompassing infrastructure, equipment, materials, and financial oversight.
Conclusion:
This study offers valuable insights into the factors influencing eye health behaviors among older persons in a Thai community, based on perspectives from key stakeholders. Guided by the PRECEDE model, it highlights the importance of health education, training, funding, service accessibility, and community collaboration. The findings underscore the need for community-based interventions that address both behavioral and environmental determinants. These insights can support the development of sustainable strategies to promote eye health and prevent avoidable blindness among community-dwelling older people. Future research should directly involve older persons and caregivers to enhance the depth and applicability of findings.
Introduction
Vision impairment poses a significant and escalating public health challenge globally, particularly among older persons. 1 The World Health Organization 2 estimates that at least 2.2 billion people worldwide experience vision impairment or blindness, nearly half of which are preventable or untreated. This burden is disproportionately high among aging populations, a trend particularly evident in Southeast Asia, where the prevalence of moderate to severe vision impairment among individuals aged 50 years and older exceeds 20%. 3 As populations continue to age, the rising incidence of conditions such as cataracts, glaucoma, diabetic retinopathy, and age-related macular degeneration further increases the risk of functional decline, reduced quality of life, and greater dependency among older persons.3-5
In many communities, older persons remain vulnerable due to limited access to eye care services, systemic healthcare constraints, and low engagement in preventive behaviors. 6 Practices such as regular eye examinations, effective management of chronic diseases like diabetes and hypertension, protection against harmful ultraviolet exposure,7,8 and adherence to prescribed treatments are essential for preventing, detecting, and managing vision-threatening conditions. However, the adoption of these vital practices is often hindered by factors such as a lack of awareness, limited health literacy, financial constraints, and prevailing cultural beliefs. Therefore, fostering sustainable eye health practices among older persons necessitates a comprehensive understanding of the social, environmental, and behavioral determinants that influence decision-making and healthcare access at the community level.
The PRECEDE model (Predisposing, Reinforcing, and Enabling Constructs in Educational Diagnosis and Evaluation) provides a systematic, theory-driven framework for assessing health-related needs and identifying the factors that influence health behaviors. It facilitates the design of tailored interventions by addressing behavioral determinants at both individual and community levels. 9 When applied in qualitative health research, the PRECEDE model enables a nuanced understanding of the real-world context of health service delivery and the perspectives of stakeholders, including service users and providers. Although the model is widely recognized in public health planning, its application in the context of eye care especially for older persons in community-based settings remains limited. This highlights an important gap in the literature and underscores the need for research that leverages the PRECEDE framework to guide the development of culturally appropriate, community-informed strategies for promoting eye health among aging populations.
Despite the escalating burden of vision impairment in older persons, there’s a notable gap in research that explores the perspectives of key stakeholders including community nurses, community leaders, village health volunteers (VHVs), and local authorities who are central to shaping and delivering eye care services. Understanding their experiences, challenges, and insights is fundamental for developing community-specific, culturally relevant strategies that can effectively address barriers to care and strengthen eye health promotion efforts.
This descriptive qualitative study aimed to explore the perspectives of key stakeholders involved in primary eye care services on enhancing eye care behaviors among older persons in a Thai community, using the PRECEDE model as the guiding framework. The findings are expected to generate critical insights into the contextual factors influencing eye health practices, thereby informing the design of targeted, culturally appropriate, and sustainable interventions. By aligning these strategies with the specific needs and realities of older persons in the community, this study seeks to support improved vision outcomes and overall quality of life for aging populations.
Methods
Study Design
This descriptive qualitative study aims to gain a comprehensive understanding of the experiences, perspectives, and insights of participants regarding eye care behaviors and primary eye care services among community-dwelling older persons in Thai.
Study Setting and Participants
Setting
This study was conducted in Muang Suphan Buri District, Suphan Buri Province, in the central region of Thailand, where eye disease ranks among the top 10 causes of illness among hospitalized patients.
Participants
Purposive sampling was employed to recruit 8 key stakeholders relevant to primary eye care services for older persons in the community. The participants included community nurses, village health volunteers (VHVs), community leaders, and a representative from the subdistrict administrative organization (SAO). The inclusion criteria were as follows (1) Community nurses with at least 1 year of experience in providing primary eye care services and willingness to share insights on eye health promotion. (2) Community leaders who were actively involved in eye health-related activities within the community and had experience collaborating with health services for older persons. (3)Village health volunteers (VHVs) with experience supporting eye health promotion activities among older persons, particularly in basic vision screening and eye care. (4) A representative from the SAO responsible for or knowledgeable about local public health policies, resource allocation, or community-based health initiatives for older persons. The exclusion criterion was any stakeholder who was unwilling to participate in the study and not able to understand Thai.
Research Process
The research process was conducted in accordance with ethical guidelines for qualitative research involving human participants. After receiving ethical approval from the institutional review board, purposive sampling was employed to identify and recruit 8 key stakeholders who were relevant to community-based eye health services for older persons. Recruitment began with the distribution of formal invitation letters sent to potential participants through their affiliated organizations. This was followed by an initial telephone contact made by the researcher to introduce the study, explain its objectives, and assess the stakeholders’ interest and eligibility based on the inclusion criteria. During the call, potential participants were provided with key information about the study, including its purpose, the type of data to be collected, the role of participants, confidentiality measures, and the voluntary nature of participation. If the stakeholder expressed interest, a detailed participant information sheet and consent form were sent via email or hand-delivered, depending on accessibility and preference. Prior to data collection, written informed consent was obtained from each participant. The consent form included information on the aim of the study, the expected duration approximately 90 to 120 min for the focus group discussion, the procedures involved, potential risks and benefits, the confidentiality of data, and the participant’s right to withdraw at any time without penalty.
Data Collection
Focus group discussions were conducted to gather rich qualitative data on awareness, barriers, needs, current policy, resources, and management related to eye care behaviors. The focus group questions were guided by the constructs of the PRECEDE model and continued until data saturation was reached, which occurred after 3 focus groups. The tool was assessed for content validity by 5 experts in ophthalmic nursing, gerontological nursing, ophthalmologist, and community health nursing. The contents, coverage, appropriate language, and organization were all considered. The reliability of this research instrument was tested by determining the Index of Item-Objective Congruence (IOC), which was found to have a value of 0.8 to 1. The instrument was then adjusted in accordance with the recommendations of all experts. Therefore, the questions used in the focus group were (1) What are the important of eye health behaviors that are associated with the prevention of blindness among older persons in the community? (2) What are the present community’s activities to prevent blindness among older persons in the community? (3) What are your thoughts on these activities: obstacles, needs, and opinions for improving those interventions? (4) What is the current policy, resources, and management in place for support activities of prevention of blindness among older persons in the community? (5) What is policy, resources, and management in place should be added to support the implementation of the prevention of blindness program among older persons in the community? A focus group discussion was then conducted with all 8 stakeholders in a neutral and accessible location within the community. The focus group discussion was led by the primary researcher who encouraged participants to express themselves openly. A trained assistant supported the process by taking field notes and managing audio recordings. Each focus group lasted 90 to 120 min. Importantly, the researchers are not staff members of the study community and have no special relationships or personal benefits connected to it.
Data Management
All focus group discussions were audio-recorded with participants’ consent and transcribed verbatim by the primary researcher to ensure the accuracy and richness of participants’ responses. To capture the full depth of the discussions, the recordings were listened to multiple times during and after transcription. Important elements such as tone, pauses, and non-verbal cues were noted where relevant. Before transcription, the researcher recorded contextual observations and personal reflections in a journal to support reflexivity. All identifying information was removed to protect participants’ confidentiality, and pseudonyms were used in all transcripts. The data were stored securely in password-protected files accessible only to the research team.
Data Analysis
The data were analyzed using thematic analysis, and organized using the PRECEDE model, which focuses on awareness, obstacles, needs and opinions, current policy, resources, and management related to eye health behaviors. First, the researcher immersed themselves in the data by reading transcripts repeatedly and making preliminary notes. Next, line-by-line coding was performed manually, assigning meaningful segments of text initial codes using both data-driven and theory-driven strategies. These codes were then grouped into broader categories and potential themes within the PRECEDE framework. The themes were reviewed and refined for clarity, coherence, and relevance to the overall dataset. Each theme was then clearly defined and named, and a thematic map was developed to illustrate the relationships among themes. Throughout the process the research team including qualitative and public health experts engaged in reflective discussions and peer debriefing to verify the themes and reach consensus. Finally, representative quotes were selected to support the findings, which were organized according to the PRECEDE model.
Trustworthiness
To ensure trustworthiness, the study focused on credibility, transferability, dependability, and confirmability. 10 Credibility was strengthened through prolonged engagement with the data and member checking by summarizing key points during focus groups to confirm participants’ meanings. Transferability was supported by providing clear descriptions of the study context and participants to help readers assess relevance. Dependability was addressed by maintaining an audit trail of key methodological decisions and analysis steps. Confirmability was ensured through reflexive journaling and peer discussions to minimize bias. These measures enhanced the rigor of the study and supported confidence in its findings for informing community-based eye health promotion.
Ethical Considerations
The proposal, questionnaires, and consent form were reviewed and approved by the Faculty of Public Health at Mahidol University (COA. No. MUPH 2023-084). Each participant was informed about the purpose, potential risks, confidentiality protection, and rights as a subject. Written consent was obtained before collecting the data. Participants’ privacy and confidentiality were rigorously protected throughout the study.
Results
Eight participants representing key stakeholders involved in eye health services for older persons in Muang Suphan Buri District were included in the study. The participants comprised 1 head nurse from the Subdistrict Health Promoting Hospital, 1 community nurse, 2 village health volunteers, 2 community leaders, and 2 representatives from the Subdistrict Administrative Organization. Participants were aged between 36 and 57 years and had between 2 and 15 years of experience related to primary eye care services and community eye health promotion for older people. In the community setting, nurses involved in primary eye care are not ophthalmic specialists but are registered nurses (RNs) trained in community health practice, which equips them with general skills to deliver basic eye health services and health education as part of their broader primary care responsibilities.
The results of the qualitative study, based on the identification of administrative and policy factors and intervention alignment using the PRECEDE model, revealed 4 themes, 10 main categories derived from 17 subcategories and their 26 corresponding codes, as presented in Table 1.
Themes, Main Categories, Subcategories, and Codes Identified from Stakeholder Perspectives Based on the PRECEDE Model.

Current Policy
Current policy refers to current policy implementation of primary eye care services that they provide to older persons. The participants revealed that they have been working on primary eye care services as the basic vision screening service for cataracts and glaucoma by ophthalmologists in cooperation with private hospitals. Including cataract surgery under the budget of National Health Security Office (NHSO) and those entitled to state welfare. Basic vision screening is conducted alongside a project that provides prescription eyeglasses for individuals aged 60 years and above. As a representative from the SAO said: “A private hospital provided local cataracts and glaucoma screenings with a team of ophthalmologists.” “In the community, eye screening will be conducted annually by village health volunteers, who will also provide relevant information.” “The Provincial Administrative Organization runs a project to provide prescription eyeglasses for individuals aged 60 and above.” “This community-based initiative coordinates with eyeglass shop staff to perform eye examinations and dispense glasses, although no ophthalmologist is involved in the vision assessment.” Community Nurse said: “This screening uses a standardized form completed once a year.”
Problems and Obstacles
Problems and obstacles involve problems and obstacles of the operation of primary eye care services in the community. These issues are linked to older people’s financial constraints. They try to minimize their expenses on eye care to save money, but often have to pay additional costs out of pocket beyond what government policies cover. Access barrier problems were concerns raised by the participants. Health villages volunteer said: “If we want to be able to get glasses that are outside of what the budget has prescribed for us, we will have to pay the cost ourselves, such as people with nearsightedness, farsightedness, and astigmatism.” “Because if you buy eyeglasses at the community market, they will be cheaper to go get glasses at the hospital because it will be expensive.”
Policy gaps were also highlighted by the participants. Proposing an eye care project requires thorough advance planning to ensure successful implementation. Policy guidelines should be established in advance, as budget allocations may be delayed unless there is an urgent need, highlighting the importance of timely financial planning. A representative from the SAO said: “To propose a project related to eye health, careful advance planning is essential. This serves as a foundation for policy development.” “Although funding may not always be fully received as initially promised to local governments, this situation provides an opportunity to adapt and explore alternative solution.” “Policies may evolve based on urgent needs, and while budgets are not always allocated in advance, there is flexibility to allocate resources as necessary to ensure the project progresses.”
Human Resources was also emphasized by participants. Participants revealed the significant important things deep within their heart as feeling low, disappointment and burned out that impair their work. A representative from the SAO said: “I feel deep sadness, disappointment, and burnout that really affect my work.” “Sometimes, we only have the manpower and authority to govern, but we lack the resources we need.”
In addition, service delivery was mentioned as eye health education is limited, vision screening lacks standardization, and uncertainty during performing basic vision screening by village health volunteers. Health education about preventing eye diseases is still not widely distributed in community. Older people, who often stay at home, have limited knowledge about conditions like glaucoma and cataracts. Many choose to buy eyeglasses for convenience and affordability, putting off hospital visits until their vision issues worsen significantly. A representative from the SAO said: “Preventing eye diseases is currently only a small part of health education and still haven’t gone into depth about preventing eye diseases.” Head of Subdistrict Health Promoting Hospital said: “In the case where older people are brought together or come to the Subdistrict Health Promotion Hospital and teach health education about eye diseases, in this case the Subdistrict Health Promotion Hospital has not yet taken action in this part.” Village Health Volunteers said: “Older people have very little knowledge about glaucoma and cataracts because they mostly stay at home.” “Most of older people, if they have eye problems, will go to the flea market and buy eyeglasses because they are comfortable and are more frugal and save money for other purpose.”
When village health volunteers conduct screenings, they often lack clear knowledge about whether individuals have cataracts or other eye diseases, which limits their ability to provide accurate advice to older people. Additionally, some village health volunteers may find it challenging to perform screenings. “As for the village health volunteers, when we go down to do the screening, we don’t know what the clear knowledge is about whether they will have cataracts or not.” “We don’t know the clear knowledge.” “We want the knowledge that we can give advice to older people” “For example, we measure that he can count on his fingers, but we don’t know if he has a disease or not. When he asks, we can’t answer.”
There were participants’ opinions concerning issues related to the standard of primary eye care services. In particular, the absence of an ophthalmologist during screenings was seen as a factor that may compromise quality. Coordination with eyeglass shops, which typically lack ophthalmologist oversight, usually involves simply assessing whether individuals are nearsighted or farsighted and providing glasses accordingly. This uncertainty regarding the presence and credibility of ophthalmologists discourages many older people from participating in projects that require eye examinations. Village health volunteer and Community leader said: “In screening, it may not be up to standard because there is no ophthalmologist to check.” “But it will be coordinating with the eyeglass shop, which may not be up to standard, knowing only if you are nearsighted or farsighted and tailoring the glasses accordingly without an ophthalmologist coming to check.” “Most of older people who do not come to be examined in the project because they do not have an ophthalmologist and do not know whether they can be trusted or not.” “We must do it for the people. Must do it together with other organizations of the country and work with local organization.”
Suggestions and Needs
Participants raised several key issues related to stakeholder involvement, program development, and the willingness of human resources. One major concern was role ambiguity among stakeholders, which affected collaboration. Community leaders said: “Sometimes, it’s unclear who is responsible for what.” “This confusion makes it hard for us to coordinate effectively and slows down the work.”
Regarding program development, participants suggested enhancing social support systems. They emphasized the importance of providing health education to older persons and offering training for village health volunteers and community nurses to improve service delivery. Teach preventing blindness in older people and teach the basic screening for eye diseases among village health volunteers were the important things that will be support the implementation of the program.
Village health volunteer said: “I want a way to prevent it so I can know whether it is or no.” “In prevention, to have knowledge about how to avoid eye disease, such as what to eat so as not to have eye diseases.” “I want to have clear knowledge in filtering whether what I do every day is right or not to make it clearer.” “I want to teach more” Community nurse said: “The nurses at the Subdistrict Health Promoting Hospital are typically graduates in general practice rather than specialized in eye care.” “Mostly in primary care and in the matter of referrals, for which we have LINE, a group of eye rooms where nurses at the hospital are in the group.” “ If there are problems, they can consult and send pictures for discussion via LINE.”
In addition, let relatives support to take care of older people’s eyes more effectively way to implementation of primary public health ophthalmology services in the community. SAO representative, community leader and village health volunteer said: “Sometimes, in addition to older people, we must have relatives come along because when we talk to older people about what disease they have, they don’t know much about them.” “And when older people come to participate in training, they usually must be accompanied by a caregiver.” “You will come to know that right now your parents have problems like this and that.” “There will be improvement to continue treatment.”
Willingness was provided by participants. Willingness to assist in project implementation is very important, participants proposed this for the supporting the implementation of the eye health promotion program. Community leader said: “As for the village headman, as mentioned, there is only manpower will fully help possible, such as helping make appointments to pick up the elderly or coordinating.” “I will help you to the utmost because I already work in this field.” Community nurse said: “If there is a need to provide knowledge to older people.” “Nurses can be part of the team providing knowledge.”
Resource Management
Resource management to support the implementation of the eye health promotion program was highlight as infrastructure, equipment and materials, financial management. Participants think together and said: “And in the location, multi-purpose meeting rooms can be used in communities, such as in temples, because older people can join easily.” “As for the equipment, the Health Promoting Hospital has approximately two to three sets of eye measurement equipment and considers that it is sufficient in the event of an eye examination in the area.”
Therefore, The PRECEDE Model Framework offers a systematic approach to developing and evaluating eye health promotion programs, particularly for fostering enhanced eye care behaviors in older persons (Table 2). This comprehensive model considers a range of interconnected factors influencing behavior change. Initially, Predisposing Factors are identified as the underlying motivations for behavior. These include an individual’s knowledge and beliefs about eye health, their health literacy concerning vision issues and available services, and their perception of aging and vision, encompassing attitudes towards age-related visual changes. Key stakeholders in this phase are community nurses and village health volunteers (VHVs), who are vital in assessing and influencing these factors through education and direct engagement with the target population.
Stakeholder Perspectives and Suggested Strategies Mapped to the PRECEDE Model to Guide the Development of Eye Health Programs for Older Persons.
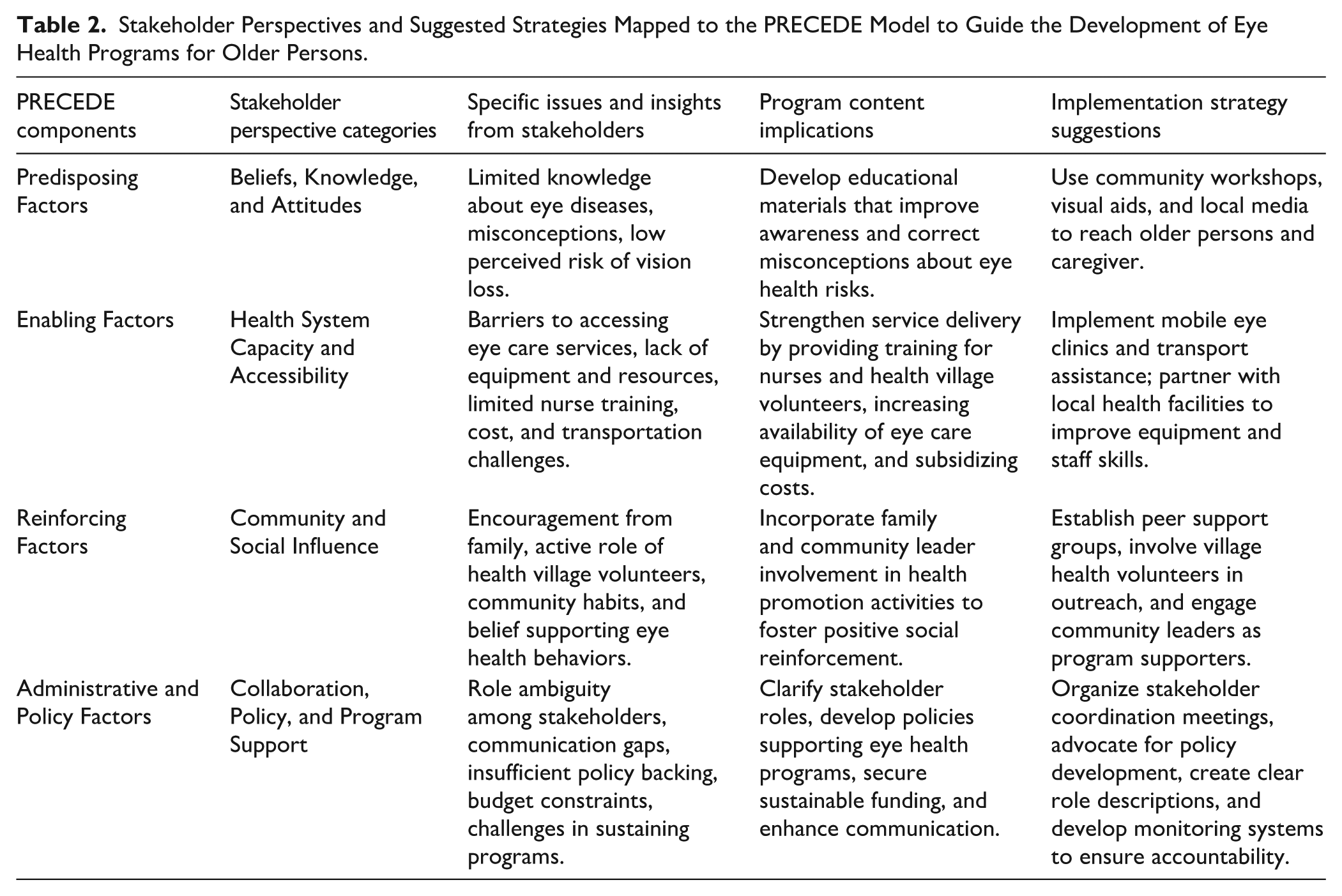
Next, Enabling Factors come into play, representing the environmental conditions that facilitate the desired behaviors and necessary skills. This involves ensuring accessibility to services, such as eye clinics and optometrists, and the availability of resources, including affordable glasses and transportation. It also emphasizes skill training for VHVs and community nurses to enable them to provide basic eye care support and referrals, along with the implementation of supportive policy and system supports that simplify access to and utilization of eye care. SAO representatives and health promoting hospital staff are crucial stakeholders in this stage, responsible for establishing and maintaining the infrastructure and policies that enable effective eye care access.
Finally, reinforcing factors are the results that happen after a behavior, which can make people want to do it again or stop doing it. These include the social support from families for seeking and maintaining eye health, active community involvement in eye health initiatives, and leader advocacy for eye care programs and awareness. community leaders, VHVs, and SAO representatives are key stakeholders in this aspect, as they foster a supportive environment and encourage the continuation of positive eye care behaviors.
The combination of these predisposing, enabling, and reinforcing factors leads to the stage where policies and interventions are planned and aligned. This strategic phase focuses on collaboration among all relevant stakeholders, the development of programs tailored to address specific needs, the mobilization of resources to ensure the sustainability of initiatives, and the creation of integrated local policies that formally support and embed behavior change. The overarching goal of this entire framework is to achieve sustainable improvements in eye care practices among older persons, ultimately leading to better vision outcomes and an enhanced quality of life for this demographic. This framework effectively illustrates how diverse individual, environmental, and social elements interact to influence eye health behaviors.
Discussion
This qualitative study explored stakeholder perspectives on the development and implementation of primary eye care services for older persons in the community, guided by the PRECEDE model. The findings revealed interconnected factors shaping eye health behaviors and service delivery, categorized into predisposing, enabling, and reinforcing components. Key themes included gaps in knowledge and awareness among older persons (predisposing factors), limited access to resources and trained personnel (enabling factors), and weak community and policy support (reinforcing factors). Role ambiguity, lack of ophthalmologist involvement, and financial constraints were also identified as significant barriers. Suggestions for future programs focused on strengthening collaboration, training, and community engagement.
The findings align with previous research highlighting the challenges older persons face in accessing appropriate eye care, particularly in low-resource or rural settings. Numerous studies have documented the compounded barriers faced by older persons, including limited awareness, lack of services, and social determinants such as income, education, and transportation.11-16 Similar to other research, participants in this study identified knowledge deficits, low perceived risk, and misconceptions as key barriers to service uptake.17-19 However, this study adds depth by capturing the lived experiences and perspectives of diverse community stakeholders including village health volunteers, nurses, and local leaders which are often overlooked in quantitative studies.
This qualitative approach provides a more nuanced understanding of how structural and operational challenges, such as unclear role responsibilities, inadequate funding, and the absence of professional oversight, impact the implementation of eye care services at the community level. These findings echo recent calls in the literature for greater attention to system-level and organizational factors in the delivery of primary eye care.20,21 By illuminating these issues, the study highlights the importance of embedding stakeholder voices into program development processes, ensuring that interventions are not only evidence-based but also contextually appropriate and sustainable.
While the PRECEDE model has been widely applied in various health promotion fields, its application to community-based eye care for older persons has been limited. This study contributes to closing that gap by using the model to structure a comprehensive understanding of the multi-level determinants influencing eye health behaviors and service uptake. The results reinforce previous findings that health behavior is shaped not only by individual knowledge and beliefs (predisposing factors) but also by enabling and reinforcing conditions such as availability of trained personnel, supportive social networks, and local policy frameworks.6,9,22,23
Importantly, this study deepens the theoretical application of the PRECEDE model by demonstrating the interdependence of its components. Stakeholders described how predisposing factors, like beliefs about older people and eye health, are inextricably linked to structural enabling conditions. Even when older persons are motivated to seek care, systemic limitations such as inadequate transportation, lack of equipment, or insufficient training among health workers may prevent action. This reflects the growing recognition that health behavior models must be interpreted through a systems-thinking lens. 24 As such, this study supports the use of the PRECEDE model as a flexible and iterative planning tool, rather than a rigidly linear framework, particularly when designing programs in complex community settings.
Moreover, the emphasis on collaborative engagement and policy-level considerations aligns with emerging global strategies for integrated people-centered eye care. For example, the WHO’s 21 World Report on Vision (2019) advocates for strengthening primary eye care within health systems by mobilizing community resources, supporting task-shifting, and promoting cross-sectoral collaboration. These priorities resonate with the study’s findings that emphasize the importance of training village health volunteers, improving communication between stakeholders, and integrating eye care services into existing community health platforms.
This study provides several practical insights that can inform the design and improvement of eye health interventions. First, tailored health education strategies should be developed to improve older persons’ understanding of the importance of regular eye screenings and available services. Using culturally sensitive materials and peer-led sessions can help increase acceptance and participation. Second, stakeholders emphasized the need to enhance access and resources by providing better training for village health volunteers and nurses, ensuring consistent funding, and offering mobile eye care services. Collaboration with eyeglass providers should also include professional oversight, such as involving optometrists or using tele-ophthalmology, to maintain quality standards. Finally, strategies to strengthen reinforcing factors should focus on building community norms that encourage regular eye care, for example by involving respected local figures as program supporters. Actively involving stakeholders in planning processes can further enhance program ownership and sustainability. The findings emphasize the importance of multi-level, context-sensitive interventions that consider the realities of local implementation, especially in resource-limited settings.
Strengths of the Study
A major strength of this study lies in its qualitative depth, which allowed for a real situation understanding of community-based eye health from multiple stakeholder perspectives. The use of the PRECEDE model provided a strong theoretical lens for organizing complex information across behavioral and environmental domains. This approach is particularly valuable for informing the development of targeted and contextually appropriate strategies to improve eye health behaviors. The study’s methodological rigor, including triangulation of informants and systematic coding, enhances its credibility and transferability.
Limitations
This study has several limitations. The sample size was relatively small, and participants were from a specific community context, which may limit generalizability. Additionally, as a descriptive qualitative study, it did not aim to test hypotheses or evaluate intervention outcomes. The findings are based on personal experiences, which may be different in other places or groups. Another limitation of this study is that it does not directly include the perspectives of older persons with eye problems or their caregivers. This was a deliberate decision, as the primary aim was to examine and synthesize strategies for promoting eye health at the community level, focusing on evaluating existing interventions and identifying broader approaches rather than exploring individual lived experiences. While some stakeholders included in this study may identify as older persons and thus partially reflect those experiences, the absence of dedicated perspectives from older persons and their caregivers may limit the comprehensiveness of our findings, particularly in understanding firsthand experiences and caregiving roles.
Future Research
Building on these findings, future research should focus on developing and piloting targeted interventions that directly address the identified barriers and facilitators, using the PRECEDE-PROCEED model as a guiding framework. The results of this study will inform the design of a structured eye health promotion program tailored for Thai community-dwelling older persons. This program will incorporate components identified through stakeholder input, such as educational materials, capacity-building for village health volunteers, and strategies to enhance community engagement and policy support. In addition, it is essential to evaluate the effectiveness of training programs for village health volunteers and assess their impact on improving service delivery. Comparative studies across different regions or countries would help determine which factors are universal and which are context-specific. Finally, further exploration of policy-level solutions is needed, including strategies to integrate primary eye care into broader community health systems with sustainable funding mechanisms and long-term support.
Conclusion
This qualitative study highlights the complex interplay of factors influencing primary eye care services for older persons in the community. Stakeholders including village health volunteers, community nurses, community governance representative and community leaders revealed key challenges such as unclear roles, inconsistent funding, and the absence of professional oversight. These factors collectively hinder effective service delivery. The findings emphasize the importance of strengthening education and improving access to trained personnel, and fostering supportive community norms to enhance eye health behaviors. By applying the PRECEDE model, this study provides a comprehensive framework that can guide the development of tailored and multi-level eye health interventions addressing both individual and systemic barriers. These insights offer valuable guidance for policymakers and health planners aiming to improve eye care programs and promote sustainable eye health outcomes among older populations dwelling in community.
Footnotes
Acknowledgements
The authors wish to express sincere gratitude to all participants and to everyone whose contributions were essential to the success of this research.
Ethical Considerations
This study was approved by the Ethical Review Committee for Human Research, Faculty of Public Health, Mahidol University (COA. No. MUPH 2023-084) on July 4, 2023. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent to Participate
All participants provided written informed consent prior to enrollment in the study.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Wasana, Plernpit, Sunee, and Chukiat. The first draft of the manuscript was written by Wasana, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was partially supported by Faculty of Graduate Studies, Mahidol University, Bangkok, Thailand.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.