
Abstract
Background:
Academic medical centers frequently recognize the importance of community engagement for advancing health equity. Yet, they often lack the infrastructure and skills needed for sustained collaboration. The 2025 Department of Medicine Research in Health Equity Symposium at the University of Rochester directly addressed this issue by focusing on community-engaged research.
Methods:
The 2025 symposium was designed to foster community engagement through 4 core strategies: (1) selecting a focused health equity topic; (2) issuing a call for community-engaged research abstracts; (3) featuring a panel of community experts; and (4) implementing targeted outreach and accessibility efforts to encourage diverse attendance. Evaluation data were collected via a post-event Continuing Medical Education survey.
Results:
The symposium drew 220 registrants across academic and community sectors. Survey results (n = 53) indicated an improved understanding of health disparities and increased knowledge of best practices for community engagement. Attendees reported greater motivation to foster community engagement in their work and identified best practices, such as centering lived experiences and reducing participation barriers. Qualitative comments indicated a desire for similar events to be hosted throughout the year.
Conclusions:
This symposium offers a replicable model for growing community-engaged research in an academic medical center. The event contributed to advancing long-term goals of health equity by building institutional capacity building and community connections. The organizing team is taking continued steps to advance community engagement, including conducting a community-engaged research landscape analysis and developing a longitudinal project to build capacity for community and clinician researchers.
Keywords
Background
Community engagement in medical research and education is widely recognized as essential for advancing health equity. 1 Studies have shown that academic initiatives developed in partnership with communities enhance the relevance of research, improve health outcomes, and build community trust in healthcare systems.1,2 However, many academic medical centers struggle to implement and sustain meaningful community partnerships.3,4 Common barriers include a lack of institutional infrastructure and incentives for researchers to support long-term collaboration, as well as misaligned goals between academic and community stakeholders.4,5 Faculty often feel under-resourced or insufficiently trained to conduct community-engaged research—especially when balancing other academic responsibilities—demonstrating a need for capacity building and support. 6 On the community side, partners may perceive engagement efforts as tokenistic or experience power imbalances in collaborations.4,7 Even when enthusiasm for engagement exists, these challenges can result in one-off events or conversations that fail to create lasting change.4,8
University of Rochester Medical Center (URMC) has experienced these precise barriers to expanding community engagement in clinical research. Specifically, many clinical researchers have expressed uncertainty over where to even begin with engaging community members. In response to these challenges, the Department of Medicine at University of Rochester developed a Research in Health Equity Symposium (hereafter “symposium”) as a means of showcasing health equity research conducted across the medical center and build sustainable partnerships. While the research symposium format is commonly used in academic medicine to disseminate research methods and results, there are few forums for sharing research and gathering with community members. Recognizing a paucity of spaces to engage around community-engaged research both locally and nationally, we made community engagement the theme for our 2025 annual symposium. The symposium is held annually with evolving themes that reflect community priorities, with community engagement serving as a foundational principle for 2025’s programming.
Rochester, NY, is a mid-sized city with a population of approximately 210 000, characterized by significant racial and socioeconomic disparities. 9 URMC, home to the Department of Medicine and the School of Medicine and Dentistry, serves as a major healthcare provider in the region. 10 Yet, Rochester also has a long history of community mistrust toward institutional systems, including healthcare, stemming from racialized policies, segregation, and uneven healthcare access. 11 These socioeconomic disparities lead to health disparities along racial lines. Compared to their White counterparts, Black populations in the Rochester area experience much higher rates of maternal mortality and complications, infant mortality, poor mental health, asthma, and hypertension. 12 The city’s health disparities make community-partnered health equity research an urgent priority.
This article describes the design, outcomes, and challenges of the symposium, demonstrating how such an event can both build capacity among healthcare professionals and trainees for community-engaged research while also enhancing rapport with community members. We discuss the symposium’s key components—including a community panel and keynote—their evaluation results, and the lessons learned for sustaining equity-focused collaborations in academic institutions. By evaluating the symposium’s impact through a post-event Continuing Medical Education (CME) survey, we sought to assess its effectiveness and glean best practices for continuing to promote health equity and community engagement within academic medicine.
Methods
This symposium represented the third iteration of the Department of Medicine’s Research in Health Equity Symposium. In previous years, while well-received, the event largely followed a traditional academic model centered on faculty research and external keynote speakers. Feedback from prior attendees and organizers highlighted the need for a more community-centered approach that aligned with institutional efforts to deepen community connections. Recognizing the limitations of earlier formats and the persistent disconnect between academic and community spaces, the 2025 symposium placed a deliberate emphasis on community-engaged research. 13 It showcased current health equity and community-engaged research projects and facilitated dialogue between healthcare professionals and community members to foster shared learning and potential collaborations. To provide a concrete example of engaging community members with lived experience, the symposium organizers selected sickle cell disease (SCD) as a connecting focus. 14 Improving care for patients with sickle cell disease has been a longtime priority for members of Rochester’s Black communities, but this patient population is often neglected in academic medical settings.
Our multi-pronged approach to addressing the problem included several deliberate strategies: (i) Selecting a focused topic to illustrate community-engaged health equity work; (ii) Soliciting broad participation through a call for community-engaged research abstracts; (iii) Incorporating a panel of community representatives to elevate patient and community voices; and (iv) Conducting outreach to encourage community member attendance. Below we outline these components in detail.
Focused Theme and Keynote Speaker Selection
The theme of community engagement was chosen to align with the Department of Medicine’s mission to improve health outcomes for marginalized members of the Rochester community. SCD was specifically selected because it is a priority research area for the community and a disease that exemplifies many areas of bias and inequity in patient care for marginalized communities.14,15 SCD Warriors and their caregivers have also expressed fatigue and burnout with regard to advocacy without support from URMC clinicians. By focusing on SCD, we aimed to ground the discussion in a concrete health equity challenge that required academic-community partnership, thus making the concept of community engagement more tangible for participants and hopefully building needed collaborations.
We invited Dr. Wally Smith, Director of the VCU Adult Sickle Cell Program and a renowned clinician, advocate, and researcher, as the keynote speaker.16 -18 This high-profile keynote was intended to set the stage and motivate attendees to “step out of [their] bubble” and reimagine our relationship to communities and to each other. His lecture emphasized the importance of engaging in open dialogue with those who see the word differently. As part of the symposium’s commitment to amplifying community voices, Dr. Smith was also invited and supported to bring a community partner to co-attend the symposium and participate in the community panel.
Call for Community-Engaged Research Abstracts
A call for abstracts was developed to encourage submissions on community-engaged research. We disseminated an open invitation for faculty, trainees, staff, and community partners to submit abstracts for projects with health equity research or programmatic initiatives, including medical education, mentorship programs, patient-centered care, and community health. The call for abstracts was disseminated through various channels including University listservs and newsletters. The Office of Health Equity Research and Center for Community Health and Prevention listservs were particularly helpful for reaching researchers engaging communities and community partners. This approach encouraged members of our academic community to share their community-engaged research efforts, and it broadened participation by attracting individuals who might not typically attend a research symposium, in part because community-engaged work is often underrepresented and not always prominently featured in traditional academic research settings.
Abstract submissions were reviewed by a committee from the Department of Medicine using a scoring rubric (Appendix 1). Engaging this committee in the review process lent a variety of perspectives, and thus credibility, to the selection. Additionally, we focused on building capacity among reviewers themselves, as they engaged deeply with the principles of authentic community-engaged research. The review panel prioritized projects demonstrating meaningful community involvement in their design, implementation, or evaluation—for example, studies that partnered with community advisory boards or incorporated patient input in shaping the research questions. Accepted abstracts were organized into thematic panels and plenary sessions at the symposium, reflecting a breadth of topics (e.g., innovations in SCD care, community-based interventions for chronic disease, patient-centered program evaluations). Presenters, whether they had a poster or oral presentation, were encouraged to invite and co-present with community partners.
Centering Community Voices
The previous year’s symposium introduced the idea of community panel where community leaders could discuss their priority areas for research, along with changes they would like to see implemented in patient care. For the 2025 symposium, we wanted to connect this panel to the central theme and demonstrate why community partners are needed for advancing health equity. We partnered with members of our medical center’s existing SCD clinical workgroup, which includes community SCD warriors, to identify and invite panelists. The organizers met with each potential panelist to share our intention for the panel and learn what would be most meaningful for them. The panel ultimately consisted of SCD warriors and advocates from Rochester and Buffalo, NY, as well as Smith’s SCD community partner from Richmond, VA. This panel was structured as an interactive discussion moderated by Dr. Smith; in doing so, it elevated the important, experiential knowledge often missing from discussions focused on research and clinical outcomes.
Outreach to Rochester Communities
Intentional outreach efforts were made to increase community attendance and engagement with marginalized community members, including but not limited to Black, Latino, LGBTQ+, low income, and refugee communities. We worked with local organizations—including regional health systems, community organizations, domestic violence shelters, urban leagues, and local nonprofit organizations—to promote the event. Personal invitations were additionally sent to community leaders, who could share the event through their local networks and organizational communication channels. These partners helped circulate invitations through their networks, extending outreach to key stakeholders for health equity research. Inside the institution, Department leadership encouraged faculty and trainees to attend, but we also distributed the event through the Office of Health Equity Research, Center for Community Health and Prevention, and other institutional listservs focused on community engagement and health disparities research.
Importantly, we took deliberate steps to remove barriers to participation for community members. With support from an institutional Office of Health Equity Research grant, we waived all registration fees for community attendees. We recognized that even a nominal fee could deter community participation, so eliminating cost was essential to ensuring community voices in the room. We also provided free parking vouchers for those attending in person, and offered a hybrid format (with both in-person and Zoom options) to accommodate individuals who might prefer to join remotely. Logistical considerations were crucial in building trust; by addressing practical barriers, we demonstrated respect for community members’ time and presence, making it clear their participation was central to the success of the symposium, not an afterthought.
A core goal of our outreach strategy was to build trust and rapport with community members. We sought to convey that people at URMC are genuinely invested in research addressing health disparities in partnership with the community. Oftentimes, community members are asked to share their wisdom with academic medical centers to improve research and care delivery. However, there is typically very little follow-up on how medical centers use that feedback, or if they implement any changes as a result. By highlighting that members of the institution are actively implementing change and eager for community perspectives, we began laying the groundwork for authentic engagement even before the symposium day. 19
Evaluation
In order to understand the success of the symposium, we invited attendees to complete a post-event CME (including Continuing Nursing Education and social work Continuing Education credits) survey designed to assess educational outcomes. Those who did not plan to claim CME credits, including community attendees, were still encouraged to complete the survey to share their valued feedback. The survey elicited both quantitative and qualitative data, providing insights into the symposium’s impact on knowledge, attitudes, and anticipated practice changes.
We used the survey to evaluate the following domains:
Symposium effectiveness: Impact of the event, including the relevance of the content, speaker engagement, and panel discussions.
Knowledge, competence, and practice change: Competence acquired, whether attendees intend to implement any changes in their practice, and whether it expanded their understanding of community engagement and health equity.
Sustained learning and further engagement: Plans for continued education, motivation for equity work, and intentions to connect more deeply with community perspectives.
Best practices: Insights from participants on how to improve future engagement and further organizational commitments to equity.
Results
Symposium Effectiveness
The Symposium drew 220 registrants—158 in-person and 62 virtual—representing faculty, staff, trainees, allied health professionals, and community members (Figure 1).
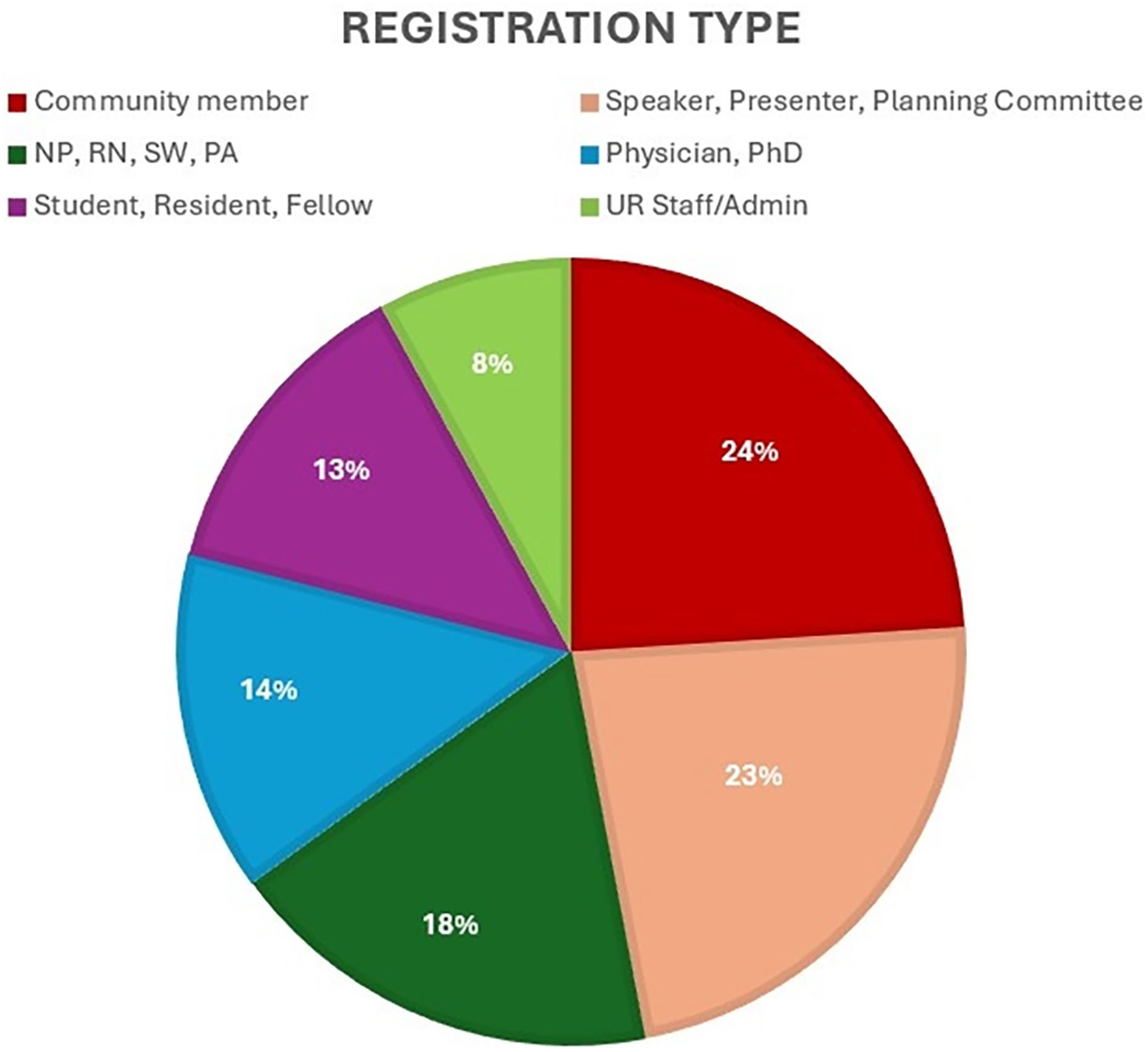
Research in Health Equity Symposium registration categories.
The CME survey was completed by 53 attendees. The results reflected strong satisfaction: 100% of respondents rated the event as Good or Excellent, with 81% selecting Excellent. Learning objectives were clearly met: 100% agreed they had an improved understanding of health disparities, and 98% agreed they could identify resources and best practices for engaging marginalized communities. Ninety-eight percent of participants said they could summarize the Department of Medicine’s equity-related scholarly work, suggesting the event met its intended educational goals. Overall comments reflected this satisfaction with respondents thanking the organizers for the opportunity to “educate myself [on] issues that matter” and noting that “everyone was well informed.” The overwhelming majority felt the symposium was free from bias and grounded in evidence, reinforcing its credibility.
Attendees consistently appreciated the keynote, community panel, and the session on innovations in SCD care (Table 1). Dr. Wally Smith’s keynote address, “Promoting Racial and Health Equity: Slogans Are Not Enough,” highlighted the challenges currently facing healthcare workers and inspired attendees to take action. The keynote was described as “phenomenal,” “inspiring,” and “powerful.” 20 Smith opened the keynote by urging attendees to “step outside of your bubble,” encouraging them to literally do so by standing up, moving around, and introducing themselves to attendees they had never met. This lecture allowed attendees to appreciate the “why” of community engagement, particularly in our current cultural climate.
Please Rate the Following Session/Speaker(s) on Their Knowledge/Content.
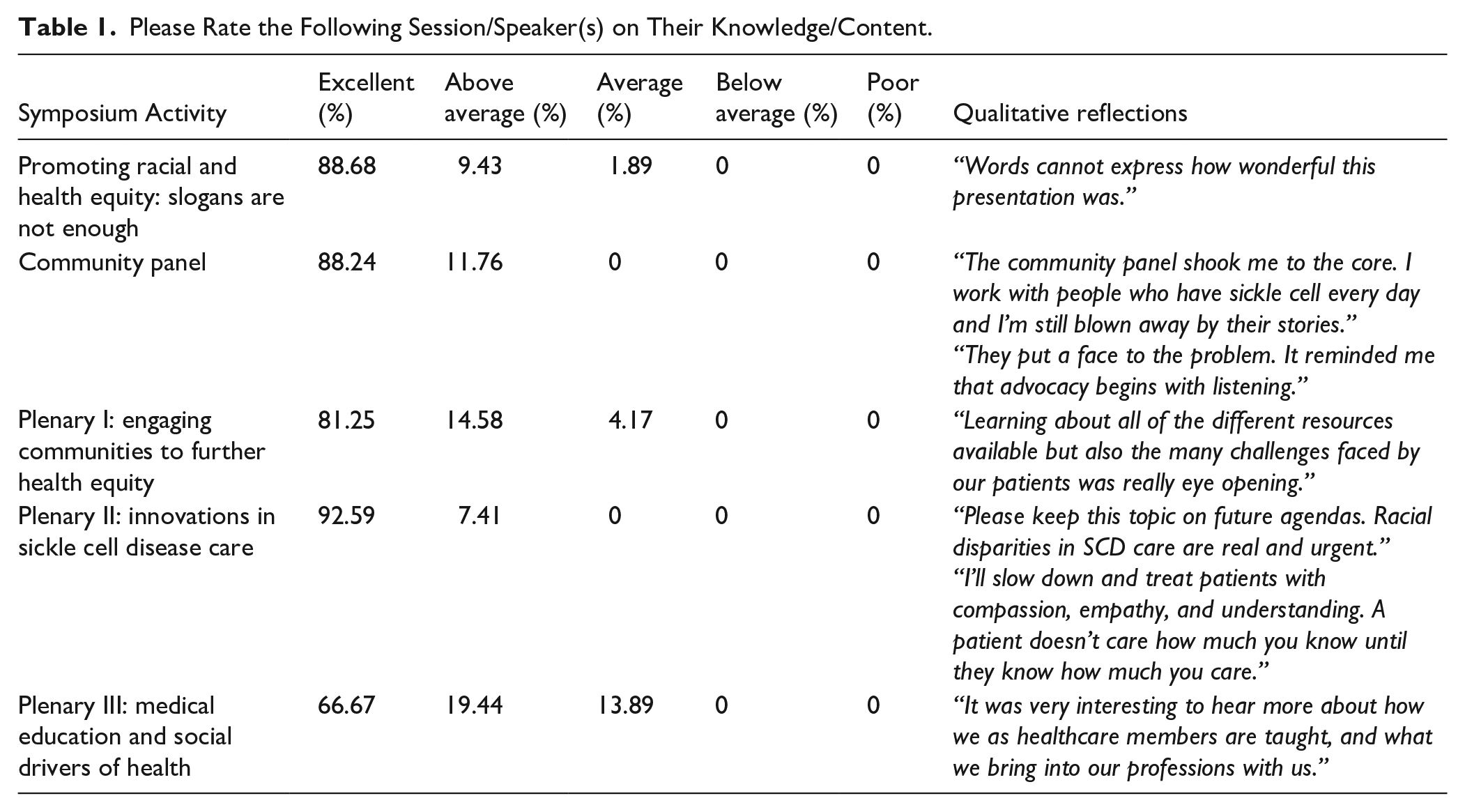
The community panel, moderated by Dr. Smith, was widely recognized for its emotional depth and authenticity; their personal narratives provided eye-opening context for faculty and trainees in the audience. Several participants requested more time for Q&A and deeper conversations with panelists. The session on innovations in SCD care further reinforced the symposium’s impact, prompting reflection on systemic inequities and encouraging a more compassionate, patient-centered approach among providers (Table 1). Throughout the event, attendees appreciated the emphasis on lived experience and the use of visual storytelling to contextualize health equity. Reflections highlighted how visual depictions of environmental health hazards—such as mushrooms, mold, and insects in children’s homes—were critical to understanding the impact of housing inequity and the importance of community-based interventions for early screening and prevention. Suggestions for future events included enhancing session flow with more thematic cohesion.
Knowledge, Competence, and Practice Change
The symposium demonstrated measurable impact across key CME domains (Tables 2 and 3). These results are summarized in the tables below:
Please Rate the Impact of the Following Course Objectives: As a Result of Attending This Activity, I Am Better Able To.

Please Rate the Project Impact of This Activity on Your Knowledge, Competence, Performance, and Patient Outcomes.

Many participants expressed learning about new resources, gaining practical insights, and cultivating a deeper appreciation for patient experiences. One noted: “This symposium increased my awareness of resources available to patients who are struggling.” Feedback also indicated that attendees left feeling inspired and ready to advocate for equity in their institutions. One wrote, “This symposium challenged me to think and step outside my bubble. I will take the lessons I learned and apply them to my daily interactions with others.” Another reflected, “I’ll slow down and treat patients with compassion, empathy, and understanding. A patient doesn’t care how much you know until they know how much you care.” Identified changes to practice included more person-centered care, earlier application of equity principles in quality improvement efforts, and increased use of community support resources.
Sustained Learning and Further Engagement with Rochester Communities
Respondents described plans to continue learning and apply new knowledge in their roles. Many expressed a renewed sense of purpose in addressing inequities. One stated, “This reminded me why I chose this field.” The evaluation demonstrated the symposium was more than a knowledge-sharing event—it was a catalyst for personal and professional growth. Overall, themes of community listening, deeper involvement, and the need for clear first steps emerged from the feedback, reflecting a willingness to move from intention to action.
Participants expressed a strong desire to deepen their involvement with local communities following the symposium. Several respondents indicated plans to stay involved by attending similar events, pursuing continued education, or engaging in proactive outreach. One attendee shared, “I’d love to have more panels and ability to hear directly from patients and families in a constructive forum,” reflecting a broader call for more spaces to learn from community voices. One attendee wrote, “This conference helped me realize we need to ask the questions and not assume what resources people need. Every community and every population deserve a chance to voice what would be beneficial for them.” At the same time, some participants expressed uncertainty—“I don’t even know where to start”—highlighting the need for structured opportunities like town halls or community-partnered programs.
Best Practices Identified
Evaluation feedback highlighted several best practices for community engagement. Comments included reinforcing the importance of centering community voices and interactive listening forums (e.g., world cafés or town halls) to engage community members directly. 21 Participants also stressed the importance of reducing barriers to participation, such as waiving fees and offering virtual options, and focusing on specific local priorities. These suggestions mirror many of the strategies we employed, and indeed, we had incorporated them based on community engagement principles from existing literature.
Discussion
The outcomes of the symposium demonstrate how a thoughtfully designed event can build capacity for academic healthcare professionals in community-engaged work and simultaneously foster trust and collaboration with the community. We found that by integrating patient voices and prioritizing community concerns, the symposium itself acted as an intervention—it not only studied a problem (lack of engagement), but also actively worked to change the situation by bringing stakeholders together in new ways. 22
Building Capacity among Healthcare Professionals
Importantly, the symposium helped address a gap in clinical professional development. Many healthcare professionals and researchers are eager to engage in community-partnered research, yet many lack formal training or support to do so. For example, a survey of faculty at one academic medical center found that 64% expressed interest in learning how to conduct community-engaged research, although less than half had prior experience in the past year. 6 Over half reported that targeted supports (e.g., career development opportunities, pilot grant funding) would increase their participation in community-engaged projects, and many junior faculty noted that academic promotion criteria seldom reward community engagement, posing a disincentive to pursue such research. 6 Their challenges reflect broader structural barriers within academic medical centers, where community engagement has traditionally been viewed as peripheral to research and clinical missions.3,6
By attending panels showcasing community engagement and hearing directly from patient advocates, participants were exposed to models for incorporating community perspectives into their own research and/or teaching. For example, presenters in the oral presentation sessions explained concrete methods, such as the formation of community advisory boards, implementation of community-led data collection, and shared decision-making in research design. In parallel, sessions on SCD care offered clinical strategies for engaging patients in developing care coordination plans, adjusting care workflows based on community feedback, and addressing social drivers of health, such as housing conditions and barriers to emergency department access. These examples, combined with the philosophical framing provided by the keynote and community panel, gave attendees a comprehensive understanding of both the why and how of community engagement.
Addressing these barriers requires intentional investment in education, training, and institutional infrastructure. Historically, medical and public health education have underemphasized key competencies for community collaboration, such as cultural humility, an understanding of social drivers of health, and the skills needed to collaborate with community partners. One promising approach is experiential learning: for example, a recent medical school course that paired students with public health organizations during the COVID-19 pandemic not only supported local communities but also enhanced students’ empathy, cultural awareness, and commitment to community-oriented careers. 23 As noted by experts, experiential learning requires infrastructure, such as community partnership offices and mentorship programs, protected time, funding for engagement, and formally recognized community-engaged scholarship in tenure and promotion decisions. 3
Furthering Engagement and Trust with Rochester Communities
As literature on community-engaged research demonstrates, trust is a cornerstone of authentic community-academic partnerships, and it must be built through consistent, genuine effort. 24 From the start, we recognized that hosting a one-day symposium would not by itself create deep trust, but it could lay crucial groundwork. The event was deliberately structured to demonstrate respect, humility, and a genuine desire to hear community voices. The community panel was perhaps the clearest manifestation, as it visibly placed community members at the center of the conversation. Feedback from community attendees, as relayed anecdotally and through survey comments, was positive; many were surprised and pleased to be “in the same room” as so many doctors and researchers discussing issues that matter to them.
Furthermore, by removing fees and providing a welcoming environment, the symposium conveyed that the institution is taking steps to lower historical barriers between academia and the public. This intention is critical, because trust is often broken when community members perceive that universities only engage when it benefits them (e.g., to recruit research participants) but are not truly invested in community priorities. 25 Our symposium attempted to change that perception by focusing on a community-identified issue—SCD disparities—and emphasizing mutual benefit through shared learning.
Best Practices
The symposium also illuminated several best practices that academic institutions can adopt to enhance community engagement. First, it is critical to center community voices and lived experiences through storytelling and patient narratives. Studies show that such narrative-based engagement fosters empathy, cultural humility, and deeper understanding among healthcare professionals. 26 Designing events and research structures where patients and community members can share their experiences in their own voices powerfully shifts medical narratives that typically center clinician perspectives. This shift aligns with the community-based participatory research model, which emphasizes power-sharing, co-learning, and mutual benefit. 27
Logistical accessibility and cultural relevance are key. Research shows that reducing barriers such as cost, location, and scheduling increases community participation and demonstrates institutional respect. 28 Institutions should align initiatives with community-identified priorities, a strategy proven to foster trust and sustainability. 29 Lastly, community engagement must be treated not as a one-off event, but as an ongoing commitment, complete with evaluation, iteration, and accountability. Institutions that adopt long-term engagement mechanisms—like advisory councils and shared governance structures—are better positioned to advance health equity and community trust. 30
Limitations
While the symposium achieved many of its goals, it was not without its limitations. Historically, one of the main mechanisms for incentivizing clinician participation in events like symposia is offering CME credit. To claim credit, attendees were required to complete an evaluation survey administered by the University’s CME office. This survey allowed us to evaluate the symposium’s impact, but it contained limitations. First, the survey is designed to measure medical education acquisition. While we could add some additional questions to the survey, the measure is not geared toward evaluating community capacity building. Second, while community members were encouraged to complete the survey to share their feedback, we were not able to differentiate between the different types of respondents. Third, measuring long-term impact (e.g., whether participants actually implemented changes or sustained community partnerships months later) was beyond the initial scope of our survey, but it is a question worth pursuing in future evaluations.
Next Steps
While we recognized a gap in opportunities for University and community members to engage in discussions of health equity research, we were not certain how enthusiastically the theme of community engagement would be received. However, the symposium’s success ultimately reinforced the importance of engaging community members at all levels of planning, and next year’s symposium will include community partners in the planning stages, review of abstracts, and judging of presentations. We have decided on a theme of building partnerships for the upcoming year and will invite abstracts for a plenary workshop session with researchers and community partners to share how they build and sustain equitable research partnerships.
The symposium was intended to fit within a wider Department of Medicine mission to enhance community engagement in clinical research. The Department is currently developing a community-engaged research landscape analysis to understand readiness to engage community members in research. This analysis will also assess barriers and facilitators to engaging communities, along with developing an inventory of Department community partners. Organizers Stamm and Shirin are developing a longitudinal capacity-building project with community partners to better prepare community co-researchers to co-develop and co-lead research centered on patient-centered priorities. Lastly, the symposium facilitated a meaningful connection with Jordan Health, one of the city’s Federally Qualified Health Centers that serves many marginalized communities. We are working to co-host a similar event focused on health equity research and advocacy located in the community.
Conclusion
While the symposium achieved its immediate aims, we acknowledge that a single event has limitations. Continued capacity building and trust building are long-term endeavors. Some feedback, such as the participant who felt uncertain about where to start, points to the need for continued support. Institutions looking to replicate this event should ensure that it is part of a larger continuum of engagement, rather than an isolated one-off. Despite limitations, the symposium offers a compelling example of how community engagement can be effectively integrated into an academic medical center to inspire clinicians to pursue community collaboration in their research and clinical practice. By treating the symposium itself as an intervention and carefully evaluating it, we have been able to learn and adjust our strategies for future iterations of the event.
Footnotes
Appendix
Abstract Scoring Rubric.

| Category | Possible points | Awarded points |
|---|---|---|
| Originality and creativity -Theoretical or clinical significance of research -Creativity and originality of logic -Timeliness and uniqueness of ideas |
5 | |
| Organization | Total of 10 | |
| Objectives/goals are clearly stated | 2 | |
| Methods are explained and appropriate for goals | 2 | |
| Results are clearly presented | 2 | |
| Thoughts and ideas flow in a logical manner | 2 | |
| Results accomplish the purposes of the project | 2 | |
| Impact of the research work |
5 | |
| Total points | 20 |
Acknowledgements
The authors would like to thank Dr. Wally Smith for his immense contributions to the success of the 2025 Department of Medicine Research in Health Equity Symposium.
Ethical Considerations
This project was undertaken as a QI initiative, and as per the University of Rochester’s Guideline for Determining Human Subject Research, did not meet the definition of research according to 45CFR46.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
Laura Stamm: Conceptualization, Data curation, Writing-original draft, Supervision.Ahona Shirin: Conceptualization, Data curation, Writing-original draft.Ashley Jenkins: Writing-review and editing.Chunkit Fung: Writing-review and editing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for the symposium described in this manuscript was provided in part by a grant from the University of Rochester Medical Center’s Office of Health Equity Research and the Center for Community Health & Prevention. The views expressed here do not necessarily reflect the views of the Office of Health Equity Research and the Center for Community Health and Prevention.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All relevant data is shared within the manuscript.