
Abstract
Introduction:
Screening for unhealthy alcohol and drug use is recommended in primary care, and effective implementation requires understanding patients’ perspectives. Failure to identify and address potential differences in attitudes toward screening across demographic groups may result in care gaps, but research examining this is limited.
Methods:
We surveyed 977 adult patients in 9 primary care clinics that participated in a screening implementation study. The survey collected demographics and attitudes toward screening/discussion of alcohol/drug use in primary care. We described responses overall and compared across age, gender, race, and ethnicity using Chi-square/Fisher’s exact tests.
Results:
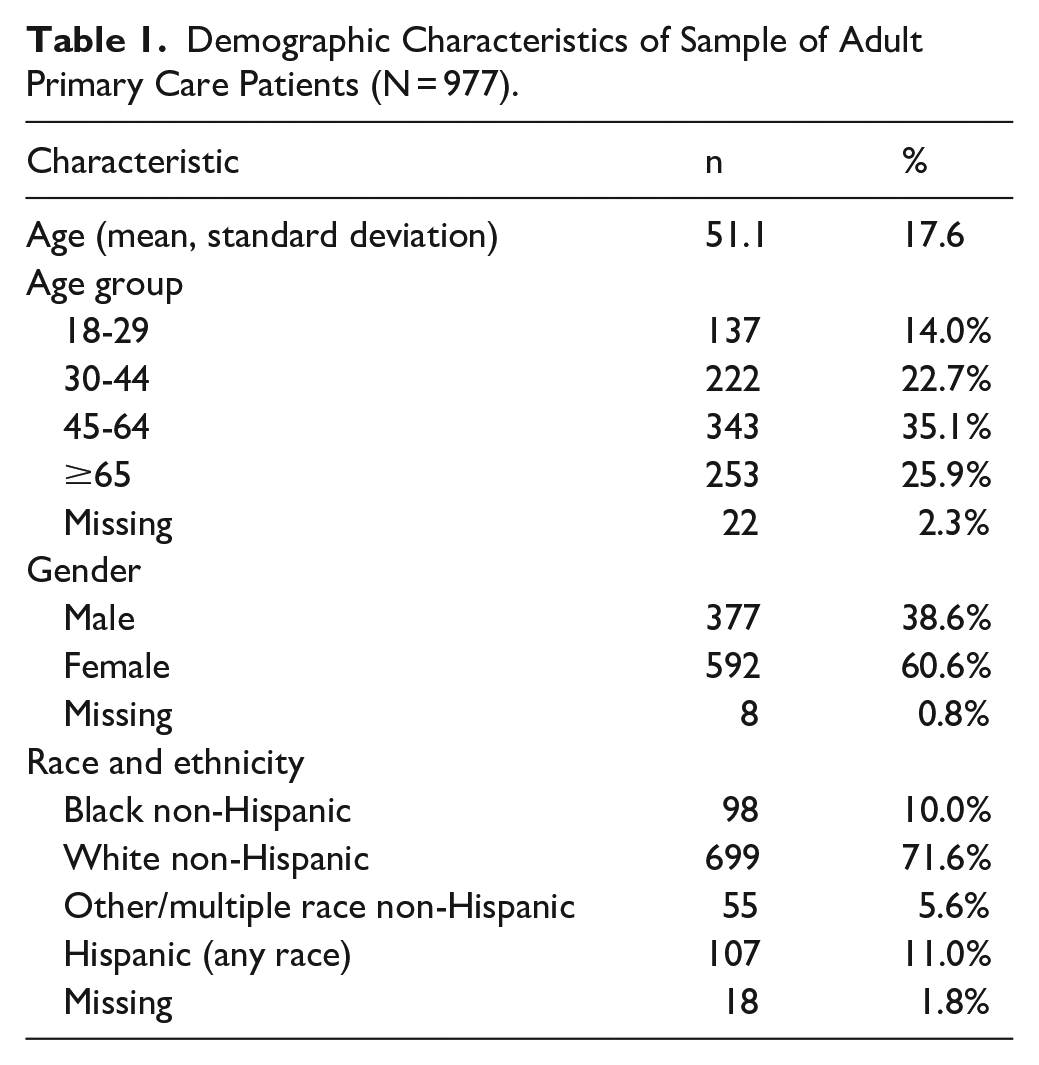
Mean age was 51.1 years, and the sample was 39% male, 61% female, 72% White non-Hispanic, 11% Hispanic, 10% Black non-Hispanic, and 6% other/unknown race non-Hispanic. Most participants across all demographic groups reported supportive attitudes. Comfort reporting drug use was lower among young, male, Black non-Hispanic, and Hispanic patients, and comfort with screening overall was lower among middle-aged, Black non-Hispanic, and Hispanic patients.
Conclusions:
Results suggest that screening/discussion of alcohol/drug use in primary care is generally highly acceptable to patients across demographic groups. Strategies are needed to increase comfort and alleviate concerns about how medical information will be used, particularly among middle-aged, Black, and Hispanic patients.
Introduction
Alcohol and drug use are common causes of preventable illness and death, and have contributed substantially to decreases in life expectancy in the U.S.1,2 Substance use increases risk for many harmful outcomes, including liver conditions, cancers, mental health conditions, overdose, and suicide.3-5 Unhealthy substance use, defined as any drug use or alcohol use above guideline-recommended levels, may not present with severe symptoms or be identified by patients as a health problem.6,7 As such, it often goes undetected in medical settings. Population-based screening is the first step to ensuring patients with unhealthy use receive appropriate care, which may include brief advice to reduce/stop use and/or providing/referring to substance use disorder (SUD) treatment.8,9 There are multiple brief, evidence-based screening tools available,10,11 and screening in primary care is recommended for adult patients by the U.S. Preventive Services Task Force.12,13
For substance use screening to be effectively implemented in primary care, it is essential to consider the perspectives of patients in this setting. Substance use is a stigmatized condition, particularly in medical settings, and this can impact patients’ comfort with screening. 14 Further, it is important to examine whether there are differences in attitudes across demographic groups. Patients may have differing attitudes toward disclosing health information informed by their experiences, which are impacted by demographic characteristics. 15 Addressing patients’ concerns during implementation of screening may increase comfort disclosing and discussing substance use in primary care, and understanding potential differences across groups may help improve care.
Prior studies examining patient perspectives have found high levels of acceptability for screening and receiving brief advice for substance use in primary care, though patients have reported concerns about confidentiality and stigma.14,16-24 There has been variation in preferences regarding screening format (eg, electronic, paper, and interviewer-administered).18,23,25 Fewer studies have examined differences in attitudes across demographic characteristics. These suggest that women may prefer electronic screening, patients with lower education may prefer interviewer-administered screening, preferences regarding advice/information about unhealthy alcohol use may not differ across characteristics, and Black and older patients may be more open to alcohol blood tests.23-26
Most prior studies examining differences in patient attitudes toward screening/discussion of substance use in primary care across demographic characteristics were conducted ≥10 years ago and/or focus only on alcohol. Therefore, updated research comparing attitudes for both alcohol and drug use is needed. This exploratory study aimed to address these questions using survey data from adult patients in primary care clinics that had recently implemented universal substance use screening.
Methods
Setting
This survey was conducted as part of an implementation feasibility study of alcohol/drug use screening in 9 primary care clinics. Participating clinics were from 2 urban academic healthcare systems in New York City and Boston, and 1 rural federally qualified health center (FQHC) in Maine.27,28 In the implementation study, validated screening questions and a brief counseling script were integrated into the electronic health record (EHR). Clinics varied in their approach (eg, screening at annual preventive care visits vs any primary care visit; patient-administered vs staff-administered) but all aimed for universal annual screening and used the same screening tools.27,28 This study was approved by the institutional review boards of the New York University Grossman School of Medicine, the Icahn School of Medicine at Mount Sinai, and Partners Healthcare System.
Participants and Data Collection
Patients were eligible for the survey if they were 18+ years old, English-speaking, received care in a participating clinic during the implementation study, and could provide informed consent. Surveys were collected 3/2018 to 6/2020. Research staff recruited participants in-person in clinic waiting rooms, and aimed to approach all patients present during recruitment periods. Participants received a study information sheet and provided verbal consent, completed the survey independently on electronic tablets, and received $5. Surveys were anonymous.
The survey collected self-reported demographic information and contained 19 Likert-scale items assessing attitudes toward screening/discussion of alcohol/drug use in primary care, including comfort discussing alcohol/drug use in primary care, biologic tests to assess alcohol/drug use, concerns about this information appearing in their medical chart, and openness to receiving advice about alcohol/drug use from their primary care provider (instrument in Supplemental Appendix A). These items were adapted from a prior survey assessing patient attitudes toward primary care alcohol screening. 24 Specifically, items were adapted to address drug screening in addition to alcohol, and new items were developed based on findings from focus groups conducted in implementation study clinics with patients, providers, and staff (comfort with drug vs alcohol screening, medical record concerns, face-to-face vs paper, and doctor vs nurse/medical assistant). 14
Data Analysis
Likert-scale items had 5 response options; to conserve statistical power, responses were collapsed into 3 categories (disagree/strongly disagree, neither disagree nor agree, and agree/strongly agree). We described the proportion in each category overall and across age groups (18-29, 30-44, 45-64, and ≥65 years), gender (male, female), and race and ethnicity (White non-Hispanic, Black non-Hispanic, other/multiple race non-Hispanic, and Hispanic any race). Statistical comparisons across groups were made using Chi-square tests, or Fisher’s exact test when an expected cell count was <5. 29 Analyses were conducted in Stata 18 software. 30
Results
Demographic characteristics of the study sample (N = 977) are described in Table 1. Mean age was 51.1 years, and over 60% of participants were 45+ years old (2% missing). Thirty-nine percent were male, and 61% were female (1% missing). Most participants (72%) were White non-Hispanic, 11% were Hispanic, 10% were Black non-Hispanic, and 6% were other/multiple race non-Hispanic (2% missing). Demographic characteristics of survey respondents appeared similar to the overall patient population of the study clinics (mean age = 53.5 years, 40.5% male, 59.5% female).27,28 EHR data used in the broader implementation study did not collect race and ethnicity in a manner consistent with this survey, therefore we could not directly compare race/ethnicity categories.
Demographic Characteristics of Sample of Adult Primary Care Patients (N = 977).
Overall Sample
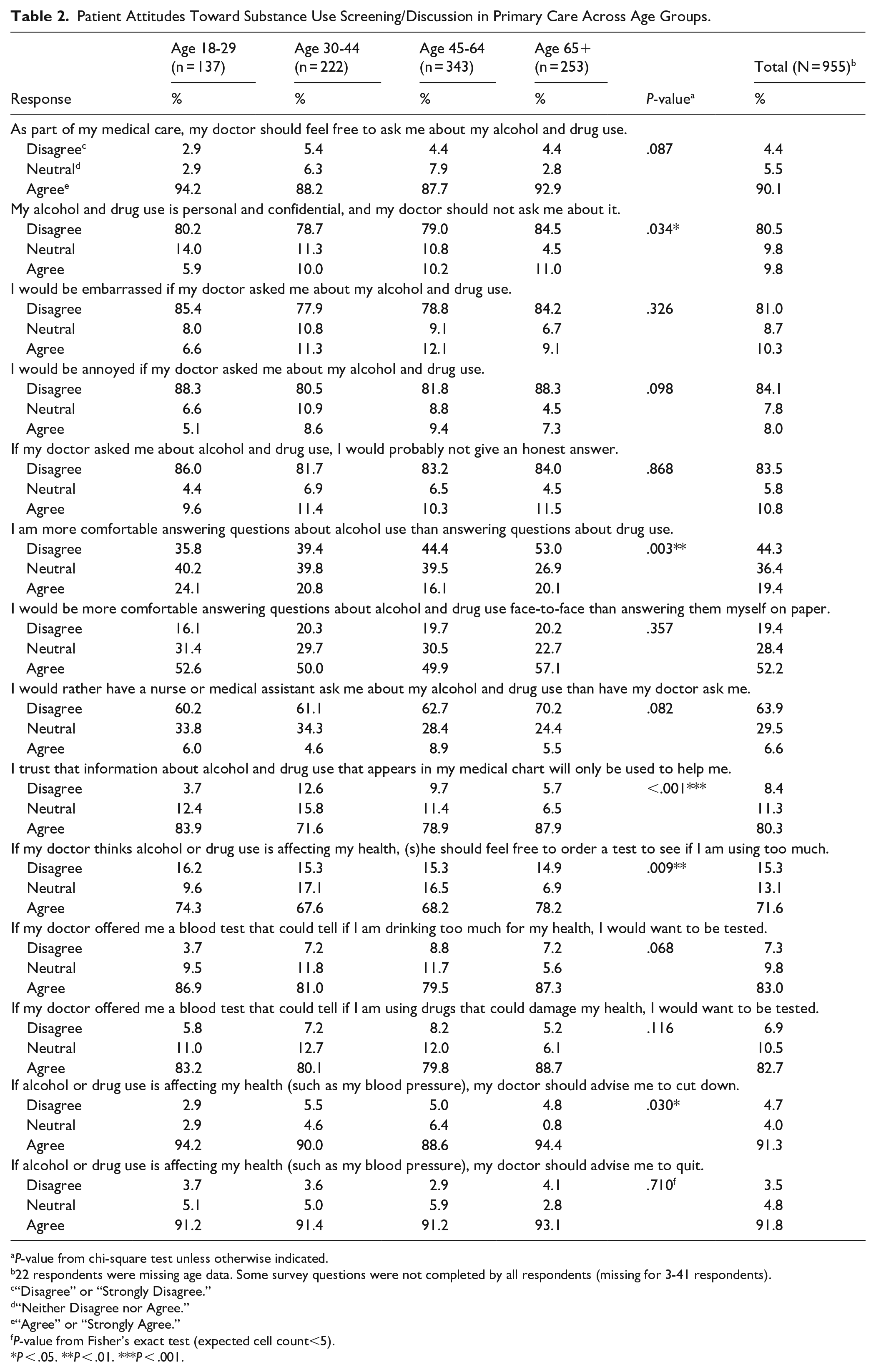
Participant attitudes are described in Tables 2 to 4. Five survey items had reverse-coded versions to check for response bias, only 1 version of each of these items is included in the tables (reverse-coded versions are reported in Supplemental Appendix B). In the overall sample, most participants agreed with statements supportive of screening (eg, 90% agreed with “my doctor should feel free to ask me about my alcohol/drug use”), ordering tests (eg, 71% agreed with “if my doctor thinks alcohol or drug use is affecting my health, (s)he should feel free to order a test to see if I am using too much”), and receiving advice (eg, 91% agreed with “if alcohol or drug use is affecting my health . . . my doctor should advise me to cut down”), and most disagreed with unsupportive statements (eg, 80% disagreed with “my alcohol/drug use is personal and confidential, and my doctor should not ask me about it”). Most (92%) agreed they would give an honest answer if asked about alcohol/drug use, 80% trusted that information about alcohol/drug use in their medical chart would be used to help them, and 88% were equally comfortable answering questions about drug use compared to alcohol. Over half (58%) preferred to have their doctor ask about alcohol/drug use rather than a nurse or medical assistant, and over half (52%) preferred face-to-face over paper screening.
Patient Attitudes Toward Substance Use Screening/Discussion in Primary Care Across Age Groups.
P-value from chi-square test unless otherwise indicated.
22 respondents were missing age data. Some survey questions were not completed by all respondents (missing for 3-41 respondents).
“Disagree” or “Strongly Disagree.”
“Neither Disagree nor Agree.”
“Agree” or “Strongly Agree.”
P-value from Fisher’s exact test (expected cell count<5).
P < .05. **P < .01. ***P < .001.
Patient Attitudes Toward Substance Use Screening/Discussion in Primary Care Across Gender.

P-value from chi-square test unless otherwise indicated.
8 respondents were missing gender data. Some survey questions were not completed by all respondents (missing for 3-43 respondents).
“Disagree” or “Strongly Disagree.”
“Neither Disagree nor Agree.”
“Agree” or “Strongly Agree.”
P < .05. **P < .01. ***P < .001.
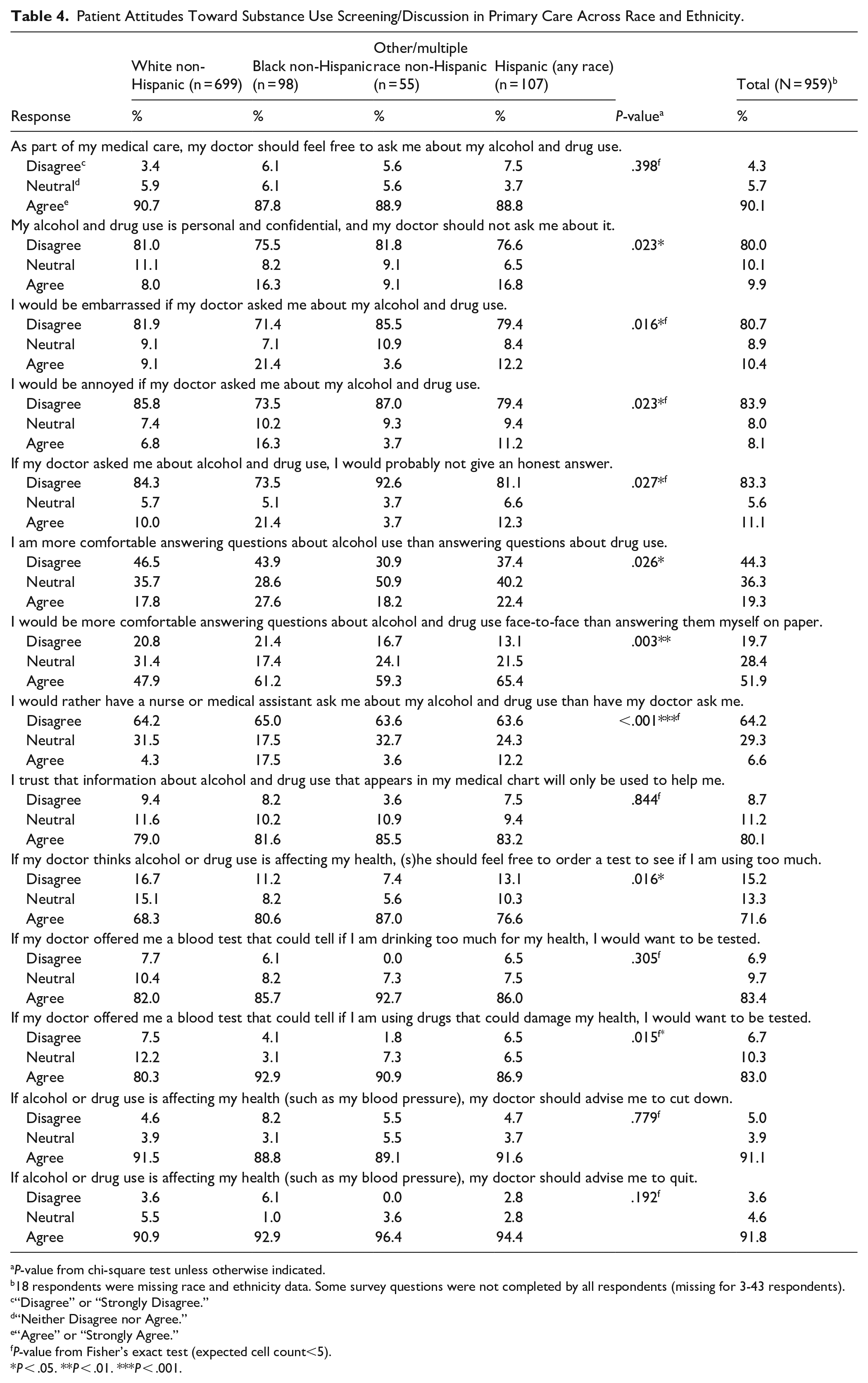
Patient Attitudes Toward Substance Use Screening/Discussion in Primary Care Across Race and Ethnicity.
P-value from chi-square test unless otherwise indicated.
18 respondents were missing race and ethnicity data. Some survey questions were not completed by all respondents (missing for 3-43 respondents).
“Disagree” or “Strongly Disagree.”
“Neither Disagree nor Agree.”
“Agree” or “Strongly Agree.”
P-value from Fisher’s exact test (expected cell count<5).
P < .05. **P < .01. ***P < .001.
Differences Across Age Groups
Age differences are described in Table 2. Participants aged 18 to 29 years were most likely to agree they were “more comfortable answering questions about alcohol use than answering questions about drug use,” while age 45 to 64 years were least likely to agree with this statement. However, there were not significant differences for “I am just as comfortable answering questions about drug use as I am answering questions about alcohol use” (Supplemental Appendix B). Participants aged 18 to 29 and 65+ years were more likely than middle-aged groups to agree with “I trust that information about alcohol/drug use that appears in my medical chart will only be used to help me,” and, “if my doctor thinks alcohol or drug use is affecting my health, (s)he should feel free to order a test to see if I am using too much.” Participants aged 18 to 29 and 65+ years were also slightly more likely than middle-aged groups to disagree with “my alcohol/drug use is personal and confidential, and my doctor should not ask me about it.” Participants aged 45 to 64 years were slightly less likely than other groups to agree with “if alcohol or drug use is affecting my health (such as my blood pressure), my doctor should advise me to cut down.”
Differences Across Gender
Gender differences are described in Table 3. While there were not significant differences for most statements, male patients were more likely than female to agree with “I am more comfortable answering questions about alcohol use than answering questions about drug use.” However, there were not significant differences for “I am just as comfortable answering questions about drug use as I am answering questions about alcohol use” (Supplemental Appendix B).
Differences Across Race and Ethnicity
Race and ethnicity differences are described in Table 4. Black and Hispanic participants were more likely to agree with, “I would rather have a nurse or medical assistant ask me about my alcohol/drug use than have my doctor ask me.” However, there were not significant differences for “I would rather have my doctor ask me about my alcohol/drug use than have a nurse or medical assistant ask me” (Supplemental Appendix B). White participants were less likely to prefer face-to-face over paper screening, and slightly less likely to agree they would want their doctor to order a test for unhealthy substance use or a blood test for drug use. Black and Hispanic participants were slightly more likely to agree with some statements indicating discomfort with discussing alcohol/drug use in primary care, including “my alcohol/drug use is personal and confidential, and my doctor should not ask me about it,” “I would be embarrassed if my doctor asked me about my alcohol/drug use,” “I would be annoyed if my doctor asked me about my alcohol/drug use,” and “If my doctor asked me about alcohol/drug use, I would probably not give an honest answer.” However, there were not significant differences for “If my doctor asked me about my alcohol/drug use, I would give an honest answer” (Supplemental Appendix B). Black and Hispanic participants were also slightly more likely to agree with, “I am more comfortable answering questions about alcohol use than answering questions about drug use.” However, there were not significant differences for “I am just as comfortable answering questions about drug use as I am answering questions about alcohol use” (Supplemental Appendix B).
Discussion
In this exploratory analysis of survey data from adult primary care patients, most participants across all demographic groups were supportive of screening/discussion of substance use in primary care, in alignment with prior studies,14,16-24 suggesting this strategy is highly acceptable across groups. Just over half preferred face-to-face over paper screening, and more preferred to have their doctor ask about alcohol/drug use than a nurse/medical assistant. There were some differences across demographic groups, most of which, to our knowledge, have not been reported in prior studies examining these differences.23-26 These findings may have implications for implementation.
While mechanisms underlying differences in patient attitudes cannot be determined from this study, several possible explanations exist. Younger people and men more commonly use cannabis and illicit drugs than older people and women, 31 which may make younger and male patients less comfortable answering questions about drug use than alcohol use. More research is needed to understand why middle-aged patients may be less open to doctors ordering tests and more concerned about substance use information in their medical record. Patients in this age range may be more concerned about negative impacts on employment or insurance.
Many of the significant differences across race and ethnicity had larger P-values (P > .01) and these differences should be confirmed in future research. However, mechanisms underlying these potential differences also deserve further study. For example, though most participants in all groups preferred to be asked about alcohol/drug use by their doctor, more research is needed to understand why some Black and Hispanic patients may prefer to be asked by a nurse or medical assistant – for example, these staff may be perceived as more trustworthy, or they may be more likely to share the patient’s racial or ethnic identity.32,33 Attitudes toward screening might change depending on whether administering providers/staff share demographic characteristics with patients; this should be examined in future research.
These findings have implications for future implementation of substance use screening in primary care. While high acceptability among patients may support successful implementation, patients’ potential concerns should be addressed to promote patient-centered care. Strategies are needed to increase comfort and alleviate concerns about how information will be used – particularly among middle-aged, Black, and Hispanic patients. Qualitative research could provide insight into how to increase comfort among these groups.
Just over half of study participants preferred face-to-face over paper screening. However, research suggests patient-administered screening (paper or electronic) is a better approach – staff-administered screening has been found to result in deviation from validated questions,34,35 and in substantially lower detection of unhealthy substance use. 27 Patients surveyed about this topic may have perceived self-administered screening as more burdensome, however in studies that have administered both types of screening, most participants have reported no preference for self- versus interviewer-administered screening.25,36 Participants also tended to prefer to have doctors conduct screening rather than nurses or medical assistants, consistent with prior studies.14,16 However, this approach may not be feasible given limitations on doctors’ time, and its acceptability likely depends on the quality of the individual doctor-patient relationship. Strategies to increase patient comfort with self-administered screening, such as providing patients with adequate information about the purpose of screening and ensuring non-stigmatizing communication and follow-up with medical providers as needed, may be beneficial.
This study has limitations. This analysis did not test a priori specified hypotheses, therefore results should be interpreted as exploratory. While research staff aimed to recruit all patients in waiting rooms, this was not always feasible. Patients who participated may have differed from those who did not in their attitudes. Future patient survey studies might collect non-respondents’ characteristics or ask why they are declining. The sample was majority female and White, and future research with more male and non-White patients may be better able to detect differences across groups. Future research is also needed to understand the perspectives of groups not represented in this study (eg, other specific racial groups and patients who do not speak English) and to examine differences across urban/rural residence. It is unclear what specific drugs participants may have been considering when completing the survey; future research should examine whether attitudes differ across drug types. Additionally, the survey did not track whether participants had already completed screening in the clinic, or what modality they experienced (patient- vs staff-administered). Finally, generalizability may be limited outside of academic and FQHC primary care settings.
Conclusions
In this survey of adult primary care patients, most participants across all demographic groups expressed supportive attitudes toward screening/discussion of alcohol/drug use in primary care. Comparisons across demographic groups suggest comfort answering questions about drug use may be lower among young, male, Black, and Hispanic patients, and comfort with substance use screening overall may be lower among middle-aged, Black, and Hispanic patients. While results suggest substance use screening in primary care is generally highly acceptable to patients across groups, strategies are needed to increase comfort, particularly among middle-aged, Black, and Hispanic patients.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251364034 – Supplemental material for Patient Attitudes Toward Substance Use Screening and Discussion in Primary Care: Comparison Across Demographic Characteristics
Supplemental material, sj-docx-1-jpc-10.1177_21501319251364034 for Patient Attitudes Toward Substance Use Screening and Discussion in Primary Care: Comparison Across Demographic Characteristics by Madeline C. Frost, Jennifer McNeely, Noa Appleton, Sarah Farkas, Sarah E. Wakeman, Timothy E. Wilens, Joseph Kannry, Bethany McLeman, Noah Nesin, Richard N. Rosenthal, Carmen Rosa, Aimee Wahle, Seth Pitts, Emily C. Williams and Leah Hamilton in Journal of Primary Care & Community Health
Footnotes
Author Note
Preliminary findings from this study were presented at the College of Problems on Drug Dependence 2020 Annual Scientific Meeting (virtual).
Ethical Considerations
This study was approved by the institutional review boards of the New York University Grossman School of Medicine, the Icahn School of Medicine at Mount Sinai, and Partners Healthcare System.
Consent to Participate
Participants received an IRB-approved study information sheet and provided verbal informed consent to participate.
Consent for Publication
Not applicable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants UG1DA013035, UG1DA015831, and HHSN271201400028C (The Emmes Company) from the National Institute on Drug Abuse, National Institutes of Health. This material is based upon work done as part of the VA Advanced Fellowship Program in HSR supported by the Office of Academic Affiliations, US Department of Veterans Affairs. Carmen Rosa, MS, Scientific Officer at the National Institute on Drug Abuse Center for the Clinical Trials Network (retired), contributed to study conception and participated in the writing of the manuscript, and was substantially involved in the study consistent with her role as Scientific Officer (UG1DA013035). She had no substantial involvement in the other cited grants. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Drug Abuse or the National Institutes of Health, the Department of Veterans Affairs, or the United States Government.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Wilens receives royalties from Ironshore, Guilford Press, and Cambridge University Press, and consults for Gavin Foundation, Bay Cove Human Services, US National Football League (ERM Associates), US Minor/Major League Baseball, and White Rhino/3D. No other authors have declarations of interest.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.