
Abstract
Background
In South Africa, rates of HIV and alcohol use are among the highest globally, with a detrimental synergistic relationship. Screening, Brief Intervention, and Referral to Treatment (SBIRT) is an evidence-based, cost-effective approach to identifying people at risk of alcohol-related problems to deliver early intervention. We developed and deployed a cascading train-the-trainer model to promote SBIRT implementation in a large nongovernmental organization offering HIV services across South Africa.
Method
Between 2021 and 2022, we completed preparatory activities including designing scalable training resources prior to rolling out the train-the-trainer model across two South African provinces. We conducted a comprehensive assessment of outcomes at the trainer- (knowledge, fidelity), provider- (attitudes, confidence, perceived implementation potential, adoption), and client-encounter (reach) levels over approximately one year.
Results
We trained 12 novice trainers who then trained 206 providers to implement SBIRT. Trainer SBIRT knowledge increased pre- to posttraining, and fidelity of training delivery was high (99.0% of elements covered across sessions). Provider attitudes, confidence, and perceived implementation potential increased over time, and 64% of providers adopted SBIRT. Reach of the model varied by component, with 41,793 clients screened by trained providers. Of those screening positive for risky alcohol use, 86% received brief intervention (BI) and 53% received referral to treatment (RT). Additionally, 15,353 clients who did not screen as having risky alcohol use received BI and 1,122 received RT.
Conclusion
Results indicated that the cascading training model was delivered with high fidelity, associated with improvements in all provider outcomes, and reached high numbers of clients for the screening component of the model. Rates of BI and RT delivery were moderate to high, though data suggested over-application of these elements with some clients, highlighting the tension between reach and fidelity. Lessons learned will inform future scale-out of this model in HIV service settings in low- and middle-income countries.
Plain Language Summary
In South Africa, rates of HIV and alcohol use are high, and they negatively impact one another. An approach known as SBIRT—Screening, Brief Intervention, and Referral to Treatment—is an evidence-based and effective way to identify individuals with risky alcohol use and provide them with interventions to reduce alcohol-related risks. The purpose of this research is to test whether a cascading train-the-trainer model can mobilize a large workforce to use SBIRT in HIV service settings. Our research team partnered with a large nongovernmental organization serving populations at high-risk for HIV in South Africa to test this training model. A small group of expert trainers from our team trained 12 novice trainers from the partner organization in how to instruct providers to use SBIRT with their clients. These novice trainers then trained 206 providers within the partner organization covering almost all (99.0%) training elements. Almost two-thirds of these providers used SBIRT, screening 41,793 clients over approximately one year. The reach of brief intervention was very high; 86% of indicated clients who were seen by trained providers received a brief intervention. Reach of referral to treatment was moderate, with 53% of indicated clients seen by trained providers receiving a referral to treatment. We also found that many clients received either a brief intervention or a referral to treatment when they did not screen positive for risky alcohol use. Our results are encouraging with respect to the feasibility of the cascading training model and its ability to mobilize a large workforce to reach clients with SBIRT, yet the fidelity of the application of brief intervention and referral to treatment warrants further research. This work highlights the tension between reaching large numbers of clients and maintaining fidelity.
Keywords
Introduction
Global alcohol consumption has increased over the past 20 years, primarily in low- and middle-income countries (LMICs) (Huang et al., 2023; Manthey et al., 2019). The World Health Organization has recommended screening and brief intervention for risky drinking in LMICs to reduce alcohol-related harms globally (Dua et al., 2011; World Health Organization, 2008). Screening, brief intervention, and referral to treatment (SBIRT) is clinically effective and cost-effective in reducing alcohol-related problems (Babor et al., 2008) and has been recommended in HIV service settings to reduce the negative impact of alcohol on HIV prevention and care (Ghosh et al., 2023; Harris et al., 2024). Yet, one recent review noted “limited literature reporting on the implementation and evaluation of substance use screening practices within HIV care settings” (Hitch et al., 2019) and another revealed the lack of availability of SBIRT for substance use in HIV care settings in LMICs (Lancaster et al., 2024).
In South Africa, rates of HIV and alcohol-use are among the highest globally, with a detrimental synergistic relationship (Llamosas-Falcón et al., 2023; Morojele et al., 2021; Rehm et al., 2017; Scott-Sheldon et al., 2013; Williams et al., 2016), yet clinical care for HIV and alcohol are siloed (Lancaster et al., 2024). To promote integrated care, the South African National Department of Health encouraged efforts to implement SBIRT in HIV prevention and treatment settings (National Department of Health, 2023). Citing studies establishing the effectiveness of SBIRT in South Africa (Myers & Sorsdahl, 2014; Pengpid et al., 2013; van der Westhuizen et al., 2021), the South African Medical Research Council advised that “individual screening for harmful/hazardous alcohol use, brief intervention and referral to treatment (SBIRT) of patients/clients should be performed routinely by trained health care workers using standardized treatment protocols and screening tools” (Morojele et al., 2013).
Promoting SBIRT and other evidence-based alcohol interventions requires contending with the severe shortage of specialized behavioral health practitioners in South Africa. Recent estimates of healthcare workers in the government-supported health system indicated there are only 0.97 psychologists and 0.31 psychiatrists for every 100,000 individuals (Sorsdahl et al., 2023). Task shifting—a strategy in which treatment tasks are distributed to nonspecialists with less training and experience (Kakuma et al., 2011; Okoroafor & Christmals, 2023; Yankam et al., 2023) – offers an opportunity to promote access to SBIRT. Train-the-trainer models are a specialized case of task shifting in which “expert” trainers train a group of health professionals to become novice trainers who in turn train larger groups of lay health providers in a new skill, thereby cascading skills to others and mobilizing a larger and more skilled workforce.
While the effectiveness of task shifting of HIV interventions is established (Fulton et al., 2011; Okoroafor & Christmals, 2023; Spedding et al., 2014), there are few studies focused on alcohol interventions, limiting the ability to scale integrated alcohol-HIV care in LMICs. There is also little known about the potential of train-the-trainer models to increase novice trainers’ capacity to deliver training content with fidelity, and in turn, the ability of such models to increase provider attitudes, confidence, and adoption of SBIRT, ultimately enhancing client reach.
Study Objectives and Specific Aims
This report describes an implementation initiative that employed a cascading train-the-trainer model to promote the uptake of SBIRT in HIV service settings in South Africa [Protocol paper citation]. Figure 1 presents a conceptual overview of the implementation initiative including the focal SBIRT intervention, the train-the-trainer strategy, and outcomes measured at the novice trainer-, provider-, and client encounter-levels.

Conceptual Overview of the Implementation Initiative and Evaluation Plan.
Method
This implementation initiative was embedded within the Alcohol Research Center on HIV (ARCH), a Center of Excellence at Brown University, and led by a multidisciplinary team that also included researchers from University of Cape Town, Northwestern University, and American University. This report describes the two-phased approach we took with our first partner. In Phase 1, we conducted preparatory work including specification of our SBIRT protocol, development of a scalable train-the-trainer curriculum, and creation of a suite of tools and protocol for fidelity monitoring. In Phase 2, we rolled out and evaluated the train-the-trainer model. Evaluation activities were reviewed and approved by the University of Cape Town Human Research Ethics Committee (HREC Reference Number 381-2020). The ethics committee determined that informed consent was required from providers, but not from clients, since SBIRT was fully integrated into clients’ usual care.
Setting and Partner
South Africa has a population of 64 million people and is divided into nine provinces. The partner organization for this implementation initiative is one of the largest HIV service nongovernmental organizations in South Africa. It provides integrated care for HIV, tuberculosis, hepatitis and other major diseases. The partner's chose to roll out the cascading training model predominantly in KwaZulu-Natal and Eastern Cape provinces and among programs targeting adolescent girls and young women given their enhanced risk for HIV. Within the programs serving these clients, activities were partially supported via grants from entities including the President's Emergency Plan for AIDS Relief and the Centers for Disease Control within the DREAMS program (Cooperative Agreement GH2188). As is true across much of South Africa, most staff were multilingual with English fluency; we therefore piloted this implementation initiative in English.
Phase I Preparatory Procedures
Specification of the SBIRT Protocol
The first preparatory step was selecting a validated alcohol use screener. We selected the 10-item Alcohol Use Disorders Identification Test (AUDIT), because it was developed using data from a World Health Organization multicountry study, is publicly available in over 20 languages, and has demonstrated strong psychometric properties in South African settings (Morojele et al., 2017). The AUDIT performs well across age groups: while the multinational study to develop AUDIT was conducted in individuals ages 15–65 (Babor et al., 2001), subsequent studies demonstrated psychometric validity in individuals ages 12 to over 85 years (Knight et al., 2003; Liskola et al., 2018; Powell & McInness, 1994). AUDIT scoring ranges from 0 to 40, and an SBIRT risk algorithm assigned clients to one of four Zones. As shown in Figure 2, clients in Zone 1: Low Risk should receive screening and alcohol education, clients in Zone 2: Hazardous Risk and Zone 3: Harmful Risk should receive screening plus brief intervention (BI), and clients in Zone 4: Possible Dependence should receive screening, BI and referral to treatment (RT) (Babor et al., 2001).
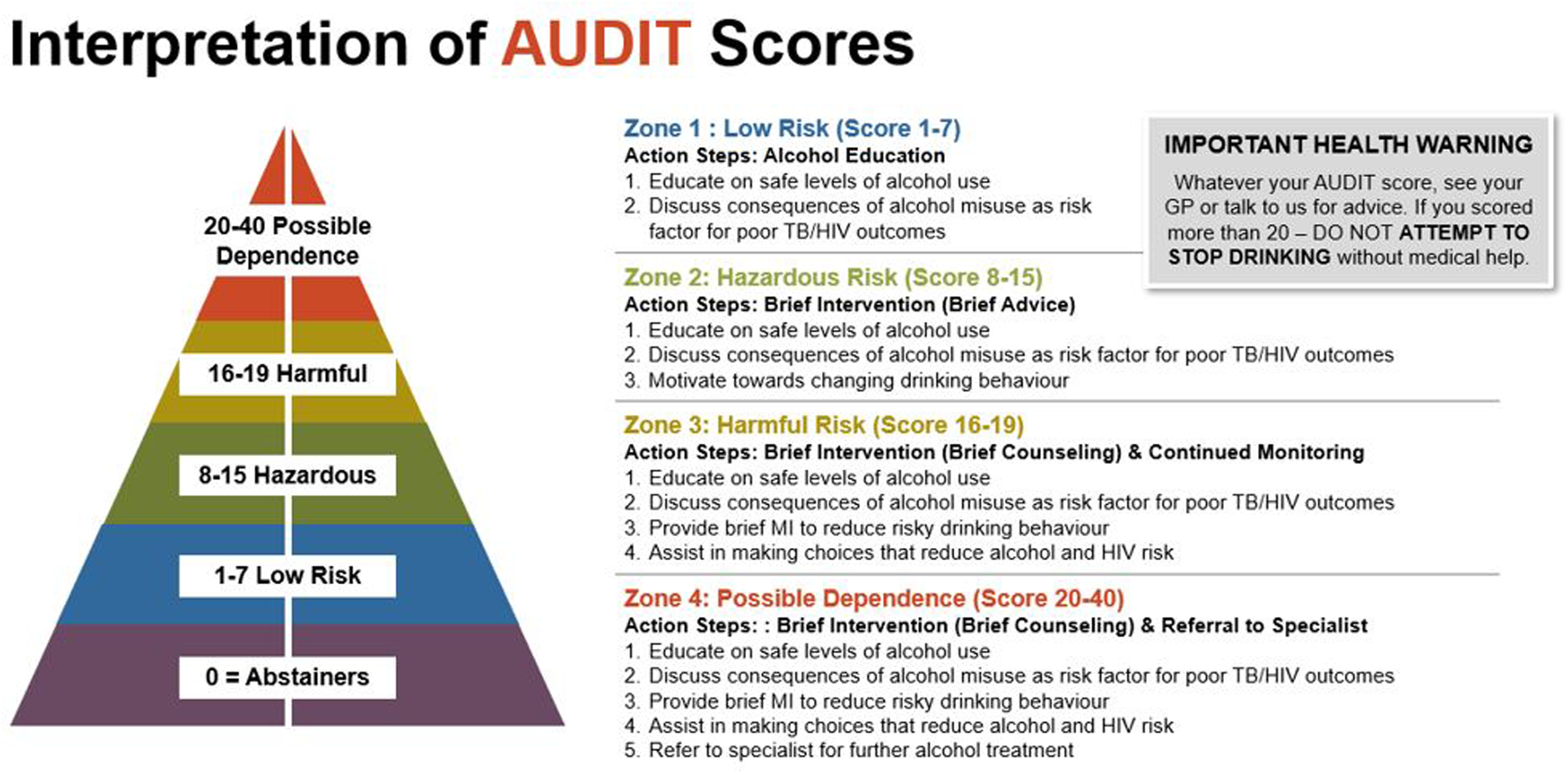
Interpretation of AUDIT Scores, as Presented in the SBIRT Training Resource Suite.
A second critical preparatory decision was where SBIRT would reside within the partner's usual workflow. The partner was already preparing to initiate a new digital platform, CommCare, to administer a comprehensive risk assessment to clients upon intake to HIV prevention services. The research team and partner organization jointly agreed to program AUDIT into the new CommCare system such that the screening questions and provision of appropriate action steps would follow immediately after questions about sexual risk and prior to a gender-based violence screener, mental health screener, and risk reduction planning template. The rollout of CommCare and SBIRT were therefore aligned. Notably, programming ensured that all providers, including those who were not part of this research project, saw the AUDIT tool as an expected part of their workflow.
Train-the-Trainer Curriculum Development
Once the SBIRT protocol was finalized, the team developed a train-the-trainer curriculum consisting of a suite of resources (Figure 3): an SBIRT Trainer's Guide, a Participant's Resource for Providers, a Technology User Manual for Providers, fidelity coding tools, and a set of agendas to guide monthly external facilitation calls. To ensure scalability and accessibility, each resource relied heavily on graphics, engaging visuals, checklists, and off-the-shelf tools, all of which were available both electronically and on paper.

Snapshots of User-Friendly Resources for Novice Trainers and Providers. The Trainer's Guide Was Developed for Novice Trainers. The Trainer Fidelity Coding Tool was Developed for an Observer to Rate Trainer Fidelity. The Participant Resource, Technology User Manual, and Provider Self-Reflection Tool Were Resources Developed for Providers.
The Trainer's Guide was a user-friendly, comprehensive set of materials to support the rigorous delivery of SBIRT training by novice trainers to health professionals and lay workers. Though we expected novice trainers to be health professionals with at least several years of experience delivering health services, materials were drafted at a secondary school literacy level to promote engagement. The Trainer's Guide started with training slides, accompanied by detailed trainer notes. These slides provided the latest evidence around effective SBIRT delivery and demonstrated how to apply the AUDIT risk algorithm to guide the selection of an appropriate BI and/or RT. The Trainer's Guide also contained instructions for each clinic location to create a list of local referrals with the capacity to address high-risk substance use and to create a site-specific protocol to oversee the RT component.
Next, a substantial portion of the Trainer's Guide focused on specific educational strategies to deliver training effectively. Educational strategies in the manual included: (1) use of role-play to develop skills of lay workers; (2) actively listening to draw out discussion from providers and promote engagement; (3) solicitation and problem solving around barriers to SBIRT implementation in specific contexts; (4) interactive learning activities and team-building exercises (i.e., ice breaker activities, vignettes); (5) time management strategies; and (6) evaluation techniques to gauge how well trainees are taking on skills (i.e., formal use of knowledge tests, informal use of guided questions). The Trainer's Guide also included guidance to address local contextual factors, such as strategies for delivering the training with limited bandwidth or electricity (i.e., using printed handouts rather than electronic slides). Finally, the Trainer's Guide included a comprehensive list of materials and checklists to be used during provider training, including full-day agendas, handouts, didactic slides, mock-ups of images and text for flipcharts, case vignettes to guide role-plays, training video vignettes, and ice-breaker activities.
The Trainer's Guide was augmented by the Participant's Resource, which was given to providers receiving the SBIRT training. The Participant's Resource consisted of step-by-step instructions for delivering SBIRT and graphics depicting the typical SBIRT workflow. Instructions emphasized that the AUDIT and corresponding SBIRT workflow were intended for clients aged 12 years and older; providers were advised to skip AUDIT administration for youth under age 12. The Participant's Resource contained a set of text-based standardized case vignettes, which providers could use to role play SBIRT delivery during the live training. These were augmented by videos shared during training demonstrating effective AUDIT administration and scoring and how to conduct BI and RT using motivational interviewing techniques. Based on the instructions in the Provider's Resource, screening was expected to take 2–3 min and BI and RT were expected to take 3–7 min depending on participant severity.
A Technology User Manual for Providers was the third component of the train-the-trainer curriculum. It contained screenshots depicting how to administer the AUDIT and record client responses within CommCare. The Technology User Manual closely aligned with the Participant's Resource: it contained example wording that providers could use to ask each screening question along with detailed instructions about how to enter the client's response to each question using CommCare.
The final component of the train-the-trainer model was curriculum (agendas and didactic lessons) for the external facilitation sessions. Consistent with the growing recognition that didactic training is more effective when paired with external facilitation (Chaple et al., 2024; Kilbourne et al., 2023; Miller et al., 2004), all health professionals and lay workers that received SBIRT training were invited to join monthly videoconference facilitation sessions. Agendas were 60-min and consisted of: (1) didactic teaching about SBIRT delivery, (2) troubleshooting of emergent implementation challenges, and (3) interactive group discussion. Didactic teaching included topics such as AUDIT review and tips for skip patterns, motivational interviewing within BI, and the importance of a referral network.
Fidelity Monitoring Tools
A final preparatory activity was development of fidelity monitoring tools including: an observer-rated trainer fidelity coding system and two self-report fidelity reflection forms (Figure 3). These tools assessed the core ingredients needed for trainers to effectively deliver SBIRT training and for providers to deliver SBIRT.
Consistent with recommendations by Carroll and colleagues (2007), the observer-rated fidelity coding system assessed two complementary elements of SBIRT training: adherence (the extent to which training elements were delivered consistently) and competence (the extent to which the training was delivered with skill). For adherence, observers rated 20 distinct training activities on a scale from 1–3 to indicate whether the trainer fully, partially, or rarely/never covered the activity. Adherence rates were calculated as the percent of items fully covered from 0 to 100%. For competence, observers rated three trainer skills on a 3-point scale to indicate whether the trainer consistently, occasionally, or rarely/never demonstrated the skill. Competence was calculated as the average of the three skills items and ranged from 1 to 3, with 3 being stronger competence. To ensure reliability, two research team members jointly rated a set of practice training sessions until 100% agreement was obtained.
The other two tools were self-report fidelity reflection forms. A Trainer Self-Reflection Tool was designed for trainers to complete at the end of each SBIRT training. This contained the same 23 items (20 adherence and 3 competence) as the observer-rater form, all of which focused on the quality and consistency of training delivery. A parallel Provider SBIRT Self-Reflection Tool containing 14 items (11 adherence and 3 competence) was developed for providers to fill out after completing an SBIRT role play.
Phase 2 Train-the-Trainer Procedures
Participants
Together with the partner organization, we set a goal to train up to 12 novice trainers, each of which would train up to 25 health professionals and lay counselors over approximately one year. Novice trainers had to meet the following criteria: (1) be currently registered with a regulatory body relevant to HIV care (e.g., registered counselor, nurse, medical doctor, psychologist, social worker); (2) have been with the partner organization for at least 1 year; and (3) have experience providing training and/or supervision to front-line treatment providers.
Novice trainers were responsible for identifying providers to which they would provide SBIRT training. Providers had to be client-facing employees of the partner organization with the ability to integrate screening into their existing workflow. Novice trainers and providers had to provide written informed consent to complete evaluation measures. Providers who did not complete the informed consent process were still welcome to receive SBIRT training but were not invited to complete evaluation measures.
Training of Novice Trainers
A Master's-level staff member with expertise in SBIRT led the training of novice trainers. Novice trainer sessions were virtual using Zoom for four hours each day over three days and followed the curriculum developed in Phase 1. As described previously, the curriculum heavily emphasized experiential learning, practice delivering elements of the SBIRT training, and provider self-reflection on their delivery of SBIRT training elements with fidelity. At the end of the three days, novice trainers received a certificate of completion indicating they were ready to deliver SBIRT training, along with 12 Continuing Professional Development credits.
Training of Providers
Novice trainers were asked to lead their first training within three months of certification completion. Provider training sessions were 1-day in duration and used training materials developed in Phase 1. The 1-day training consisted of 6 hours of didactic instruction focused on SBIRT (guided by the Trainer's Guide and Participant's Resource) and two hours of practice using the CommCare system (guided by the Technology Manual). A single member of the research team conducted live observation of each trainer's first SBIRT training session, using the observer-rated fidelity system. Novice trainers were informed that if they did not receive an adherence rate of at least 80% or an average competence score of at least 2.5, they would receive corrective feedback.
Facilitation Calls
Monthly facilitation calls were offered throughout the 12-month implementation initiative using the agendas and didactic curriculum created in Phase 1. Both novice trainers and providers were invited to join as many of these calls as they found helpful and feasible. Calls were led by local research team members and designed to enhance the sustainability of the SBIRT training by reinforcing skills and troubleshooting barriers to implementation routinely.
Measures
Figure 4 depicts key implementation events and the timeline of data collection for evaluating the cascading train-the-trainer model at the novice trainer-, provider-, and client encounter-levels. Trainer-level measures included SBIRT knowledge and fidelity. Novice trainers completed measures of their SBIRT knowledge both prior to and after the 3-day training. The SBIRT knowledge measure was based on an SBIRT Knowledge test developed by Knopf-Amelung and colleagues (2018) and adapted for the South African context. It assessed the novice trainer's knowledge of SBIRT using a 20-item scale comprised of true/false and multiple-choice questions. Fidelity of training delivery was assessed at the novice trainer's first training using the observer-rated fidelity tool described in Phase 1.

Timeline of Key Implementation Events and Assessments.
Provider-level measures included attitudes, confidence, perceived implementation potential, and adoption. All provider measures other than adoption were assessed prior to the provider training and 3- and 6-months posttraining via provider surveys, whereas provider adoption was measured over the full 12-month initiative. Based on measures contained in the SBIRT Implementation Toolkit developed by the Emergency Nurses Association (Cameron et al., 2010), provider attitudes towards SBIRT were measured on a 10-item scale and provider confidence was measured on a seven-item scale. Item scores ranged from 1 (strongly disagree) to 5 (strongly agree). Perceived implementation potential was measured using three well-validated, brief scales that measure acceptability, feasibility, and appropriateness, respectively (Weiner et al., 2017). Each measure contained four items scored on a 5-point scale ranging from 1 (completely disagree) to 5 (completely agree); we averaged all acceptability, feasibility and appropriateness items to calculate a singular “leading indicator” of implementation potential (Proctor et al., 2011). Adoption measured the proportion of trained providers who delivered SBIRT to at least one client, based on extraction of CommCare data.
Client encounter-level data were tracked to examine the reach of each SBIRT component. For screening, reach was calculated as the proportion of client encounters over the implementation initiative that had documented evidence of screening with the AUDIT. For BI and RT, reach was calculated as the proportion of clients screening in the indicated Zones who received appropriate intervention. We calculated reach in two ways: first by dividing the total number of clients screened by the number of clients seen by the target program over the approximate 1-year tracking period, and second by dividing the total number of clients screened by the number of clients seen by the organization overall during that period.
In addition, novice trainers and providers provided basic socio-demographic data including their South African population group (e.g., the equivalent of race/ethnicity in the USA), biological sex, and years of experience in the field. Clients reported their age and biological sex as part of the AUDIT screening process.
Analysis Plan
SBIRT knowledge, adoption, and reach were examined via pre‒post tests and descriptive statistics. Change in novice trainers’ SBIRT knowledge was examined via paired-samples T-tests comparing scores before and after training. Provider adoption and reach were then examined via descriptive statistics.
To investigate change in provider outcomes (attitudes, confidence, and perceived implementation potential) over time, we performed latent growth curve modeling in a structural equation modeling framework. This type of model characterizes within-individual change as a function of a random intercept and random slope characterizing the functional form of an individual's scores over time. Between-person differences are characterized as between-subjects variance on this random intercept and slope. Intercept and slope were modeled such that a linear trend of time was examined (loadings for the slope coded 0, 1, and 2 for baseline, 3-month, and 6-month assessments, respectively). A mean value of the random slope significantly greater than zero was viewed as confirmation of a sample-wide significant increase in each outcome. Longitudinal models of all provider-level outcomes accounted for clustering at the trainer-level.
To accommodate missing data in provider outcomes, we used a maximum-likelihood estimator with robust standard errors that enabled full-information likelihood estimation under the assumption that the data were missing at random (MAR), meaning robust inferences minimizing bias can be drawn when known causes of missing data on the outcome variables are included as predictors in the model. This estimation method minimizes potential bias introduced from missing data patterns. Because all SBIRT questions were programmed with forced response, and any patient who received standard intake procedures received SBIRT, there was no missing item-level data on the AUDIT. Latent growth curve models were conducted in Mplus version 8 (Muthén & Muthén, 1998–2021).
Results
Training and Sample Characteristics
Two three-day trainings were conducted with 12 novice trainers in August 2021 (10 novice trainers) and January 2022 (two novice trainers). The novice trainers primarily identified as women (n = 8; 67%) and as Black African (n = 11, 92%). They had an average of 10.83 (SD = 7.83) years of experience in the field. Most identified as social workers and nurses, and 42% had prior familiarity with SBIRT (Table 1).
Demographic and Professional Characteristics of Novice Trainers (N = 12) and Trained Providers (N = 206).
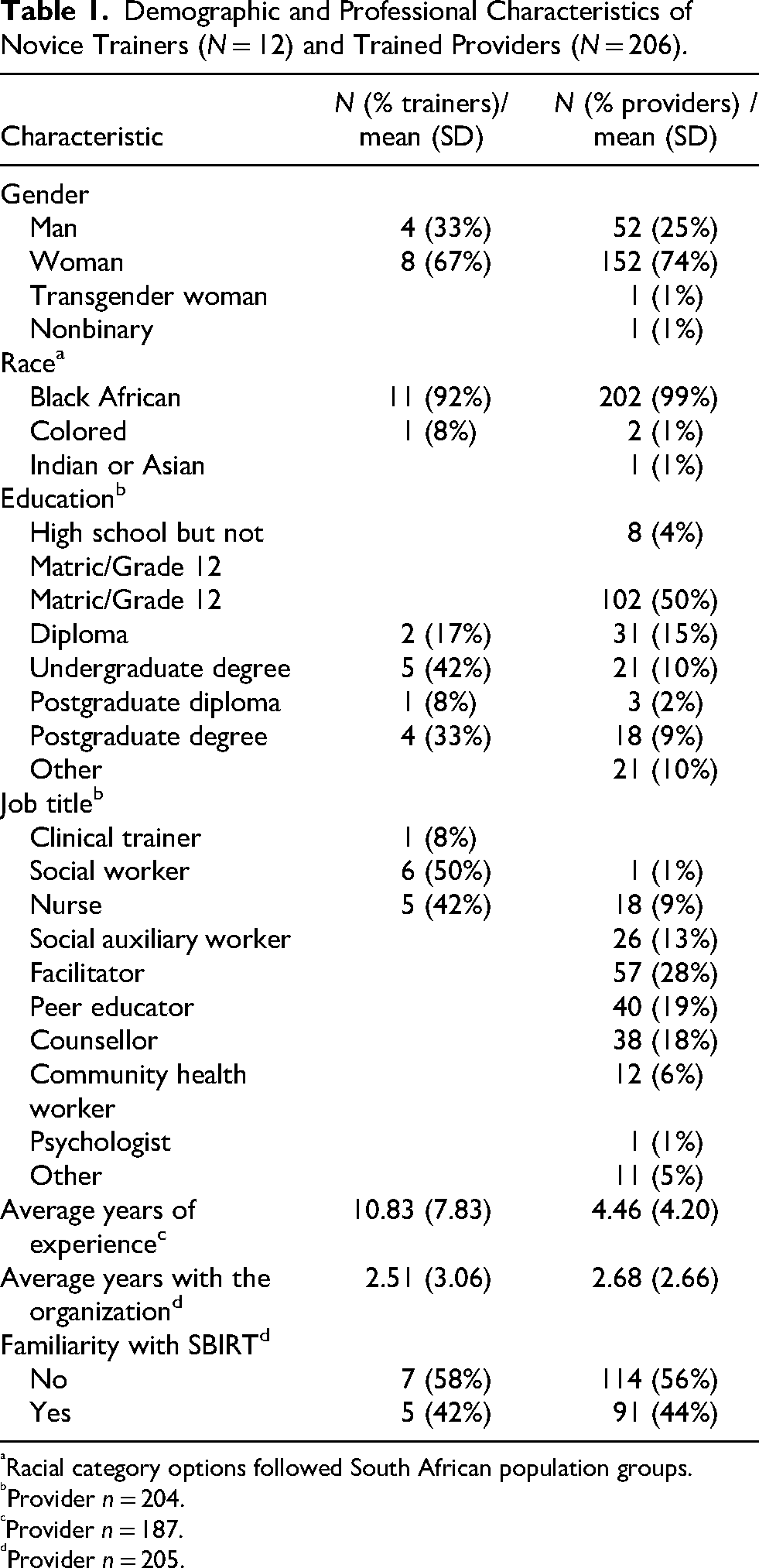
Racial category options followed South African population groups.
Provider n = 204.
Provider n = 187.
Provider n = 205.
Between October 2021 and March 2022, the novice trainers trained a total of 206 providers across 239 unique locations spanning five municipalities in South Africa (within KwaZulu-Natal and Eastern Cape provinces) including Oliver Tambo District, eThekwini Metropolitan, uMgungundlovu District, uThukela District, and Zululand District. Provider attendance per training session ranged from 9 to 25, with an average size of 14.71 (SD = 5.17) providers per training. Attendance at facilitation ranged from 1–25 (median = 8) participants per call. Seventy-four percent of providers identified as women, 99% were Black African, and 50% matriculated Grade 12 (Table 1). Providers described their job responsibilities as facilitators, peer educators, counselors, and social auxiliary workers. On average, providers had 4.46 (SD = 4.20) years of experience in their field. Just under half (44%) had familiarity with SBIRT prior to training.
Between November 2021 (the month following the first provider training) and November 2022, a total of 41,793 clients received SBIRT from trained providers. An additional 13,958 clients were screened by providers at the organization who did not participate in the cascade training model due to the integration of SBIRT into CommCare, resulting in 55,751 screens over a 12-month period. Reflecting the organization's focus on adolescent girls and young women, clients predominantly identified as female (84%) with an average age of 18.84 (SD = 5.01). Consistent with the multinational validation sample, 85% of clients were age 15‒65 years, with a moderate subset under the age of 15 (14%) and less than 1% over the age of 65. Client demographics did not differ between providers trained via the cascading model versus those untrained.
Trainer-Level Outcomes
Novice trainer SBIRT knowledge improved significantly following the training (pretraining M = 10.5, SD = 1.3; posttraining M = 15.0, SD = 3.0); t(df = 10) = 5.076, p < .001. Two of the 12 novice trainers did not go on to lead a provider training. The remaining trainers each led at least one, for a total of 14 provider training sessions. Fidelity of training sessions was high, with 99.0% of training elements covered in full with an average skill rating of 2.83 (SD = 0.18).
Provider-Level Outcomes
Table 2 presents the results of the repeated measure analyses examining change in provider attitudes, confidence, and perceived implementation potential over time. The retention rate among actively employed providers was 91.7% and 77.9% at the 3- and 6-month assessments, respectively. Provider confidence, attitudes, and perceived implementation potential of SBIRT all improved significantly (b values = 0.05–0.14, p < .039).
Provider Outcomes Over Time.

Of the 206 trained providers, 131 screened at least one client, indicating provider adoption rates of 64% among those trained. Records also revealed that four novice trainers and an additional 64 providers who did not attend the SBIRT training ultimately delivered SBIRT. Inclusion of these providers and novice trainers revealed an adjusted adoption rate of 73% when using those trained and those untrained in the denominator (199 individuals delivering SBIRT out of 274 individuals trained and/or administering SBIRT untrained) or an adjusted rate of 97% when using only those trained in the denominator (199 individuals delivering SBIRT out of 206 individuals trained). Notably, SBIRT accuracy did not differ between trained and untrained providers.
Client Encounter-Level Outcomes
We assessed reach overall both among the participating programs and across the entire organization. This calculation indicated that 57% of all clients seen by participating programs and 25% of all clients seen by the entire organization were screened via AUDIT during the approximate 1-year tracking period.
To assess reach of BI and RT for clients seen by trained providers, we calculated the proportion of clients who screened as indicated for BI and RT that received those components. In total, 86% of indicated clients received BI and 53% received RT. Trained providers delivered an additional 15,353 BIs and 1,122 RTs to clients who did not screen as indicated.
Discussion
This implementation practice report describes a novel cascading train-the-trainer initiative in HIV service settings in South Africa. The train-the-trainer initiative was associated with increased trainer knowledge, high trainer fidelity, and improvement in provider attitudes, confidence, and perceived implementation potential over time. Provider adoption was moderately high, with 64% of trained providers using SBIRT with clients. An unanticipated benefit of the model was that an additional 64 providers and 4 novice trainers delivered the SBIRT protocol, leading to an adjusted adoption rate of 73% or 97%, depending on the denominator. This pattern of results indicates that novice trainers led the training with high fidelity and providers in turn adopted SBIRT, with their attitudes, confidence, and perceptions of implementation potential increasing over time.
The encouraging results at the novice trainer- and provider-levels can be interpreted in the context of well-documented facilitators of the adoption of SBIRT and other evidence-based practices. Established facilitators of adoption include leadership support, organizational prioritization, alignment between the evidence-based practice and the organization's mission, and compatibility of the evidence-based practice with usual care (Bach-Mortensen et al., 2018; Cooke et al., 2019; Leonard et al., 2020), all of which were present in this implementation initiative. The partner organization had leadership buy-in to implement SBIRT, identified integration of HIV and alcohol care as a strategic priority, and had an organizational mission statement that explicitly valued prevention and early intervention. The SBIRT protocol was also highly compatible with usual care, particularly given the brevity of the AUDIT and the ease of integration into CommCare.
While outcomes at the novice trainer- and provider-levels were universally encouraging, data at the client encounter-level varied by SBIRT component. Reach of SBIRT was modest, with approximately 57% of clients receiving SBIRT. This rate was associated with a large absolute number of clients screened (55,751) yet indicates that over 40% of admitted clients were not screened, despite the partner's decision to make SBIRT screening compulsory. A review of organizational records suggests that SBIRT was virtually always conducted when the standard intake battery was completed and was skipped only when the battery was missed; therefore, the issue was not adherence to SBIRT but rather adherence to standard intake procedures. There are several possible explanations for providers’ lack of adherence to standard intake that are well documented, including limited time with clients, providers feeling overburdened, low provider retention, and difficulty transitioning from paper-based to digital systems (Bach-Mortensen et al., 2018; Evans et al., 2023; Leonard et al., 2020; van der Westhuizen et al., 2019; Zharima et al., 2023).
Among trained providers, reach of the BI component was excellent at 86% while reach of RT was moderate at 53%. The modest rate of RT was consistent with prior SBIRT implementation trials in the United States and globally, which found implementation rates were lowest for the RT component of the model (Evans et al., 2023; Mello et al., 2024). Two recent SBIRT implementation trials which implemented SBIRT across10 sites, found that the postimplementation RT rate was 25–26%, which are far lower than those attained in the current initiative (Evans et al., 2023; Mello et al., 2024). A well-documented implementation challenge for RT is provider concern about long wait times and limited referral options, particularly for clients with co-occurring physical or psychiatric concerns or childcare needs (Nunes et al., 2017). Improving RT uptake would likely require identification or creation of new referral pathways for clients at high risk of alcohol use disorder.
Notably, the cascading train-the-trainer model had high rates of unanticipated reach, both in terms of untrained providers delivering the model and unindicated clients receiving BI and RT. The reach to untrained providers and the lack of differences in SBIRT accuracy between trained and untrained providers was highly encouraging and speaks to the scalability and sustainability of the technology-based platform and the training resources. By contrast, the unanticipated reach to clients who did not screen as indicated for risky drinking was less desirable. In some cases, providers were screening clients that were too young, whereas in other cases, providers were delivering BI and RT to lower risk clients. Conversations with our partner have suggested two possible explanations. First, SBIRT was integrated into programs that served populations at extremely high risk of HIV, including adolescent girls. Providers may have delivered BI and RT to lower risk clients as an opportunity to prevent future risky substance use in a key population, an approach that would be consistent with youth substance prevention programs based on brief motivational interventions (Reyes-Rodríguez et al., 2020). Second, providers may have self-reported delivering BI and RT even though they did not due to demand characteristics or perceived pressure to document the tasks as completed. This interpretation would be consistent with data suggesting that providers often over-report delivery of evidence-based behavioral interventions (Hogue et al., 2013).
Limitations
There are several limitations to this work. First, our calculation of reach of BI and RT was based on self-report, which as noted previously may have been subject to over-reporting. Second, 14% of the sample was under 15 years old and prior work has suggested that adolescents might benefit from different cutoff scores (Knight et al., 2003; Liskola et al., 2018). Third, the data extracted from CommCare were limited, since the rest of the standard intake process was funded by a grant from the Centers for Disease Control and Prevention that was not available for analysis. We could not access data regarding where clients were within the HIV care cascade, which would offer critical insight into which populations were reached by this implementation initiative. That said, the programs where SBIRT was implemented predominantly served adolescent girls and young women, suggesting that most clients were in the earlier stages of the HIV care cascade. Fourth, each of the 239 unique clinical locations was responsible for generating its own referral process and the monitoring of these processes was beyond the scope of the current protocol. As a result, specific locations to which patients were referred, which services were available, wait times, and patient follow-through were not tracked systematically. We therefore cannot conclude whether the RT rates were affected by access issues. Finally, this implementation initiative focused on evaluating multilevel outcomes with limited attention to the assessment of contextual determinants.
Future Directions
Future work will address limitations and expand upon this initiative in several ways. First, we will shift away from dichotomous self-report of whether providers delivered BI or RT; instead, we will ask providers to review a list of therapeutic techniques and to indicate which, if any, they used. This list of techniques will be prefaced by language indicating that not all clients are expected to need all therapeutic techniques in hopes of prompting more honest self-reporting and to reduce the likelihood that the overapplication of BI and RT is the result of demand characteristics/over reporting rather than a true deviation from fidelity. Next, we will seek novel technology-assisted strategies, including the use of artificial intelligence, voice recognition software and refined workflow programming, to optimally balance the reach and fidelity of the SBIRT model. Such strategies will aim to ensure that the scoring algorithm is sensitive to developmental differences in clients and that the BI and RT components of the model are not over-applied so as to avoid placing greater than intended burden on providers. Third, we will include more questions on HIV status and/or treatment and expand our tracking of referral options to enhance our evaluation of SBIRT implementation across the HIV care cascade. Finally, we will conduct qualitative interviews with partner administrators, novice trainers, and providers guided by the Consolidated Framework for Implementation Research (Damschroder et al., 2022) to solicit perspectives on factors that enhanced and hindered the success of the initiative.
Conclusions
This implementation initiative occurred within the context of growing calls to implement SBIRT in LMICs (Kane et al., 2023; Suleman et al., 2021; van der Westhuizen et al., 2019), a critical need to address the dual HIV and alcohol use epidemics (Baliunas et al., 2010; Llamosas-Falcón et al., 2023; Morojele et al., 2021), and increasing recognition of the utility of task shifting (Spedding et al., 2014; Yankam et al., 2023). The cascading train-the-trainer model demonstrated evidence of high trainer fidelity, moderate provider adoption, and improved provider attitudes, confidence and perceptions of implementation potential. In addition, the model reached 55,751 clients, with far higher rates of reach for BI and RT than found in other large-scale implementation initiatives. Further, the model demonstrated high potential for sustainability given the off-the-shelf nature of training resources and the ease with which untrained provider delivered SBIRT. Overall, there is great promise for this highly scalable train-the-trainer implementation strategy to advance integrated alcohol-HIV care in settings with limited resources and high clinical needs.
Footnotes
Ethical Considerations
All study activities were reviewed and approved by the University of Cape Town Human Research Ethics Committee (HREC Reference Number 381-2020).
Informed Consent Statements
All study participants provided written informed consent as approved by the University of Cape Town Human Research Ethics Committee.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the National Institute on Alcohol Abuse and Alcoholism of the National Institutes of Health under award number P01AA019072. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or any other funder.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data may be made available upon request to the corresponding author.