
Abstract
Introduction:
The U.S. has the highest number of incarcerated persons per capita, and individuals who experience parental incarceration (PI) in childhood are at increased risk for internalizing and externalizing behavioral health conditions across the life course. This study explored the relationship between PI and mental health outcomes, including diagnoses of Attention Deficit/Hyperactivity Disorder (ADHD), Post-Traumatic Stress Disorder (PTSD), and depression by mid-life.
Methods:
Using data from Waves IV and V of the National Longitudinal Study of Adolescence to Adult Health, we assessed whether individuals who experienced PI before age 18 had higher rates of ADHD, PTSD, and depression diagnoses in mid-life and if the gender of the parent and child moderated these outcomes. We used a cross-sectional design which included chi-square tests of independence and logistic regression.
Results:
Participants who experienced PI had approximately twice the odds of depression (OR = 1.64; 95% CI: 1.30-2.09) or PTSD (OR = 1.70; 95% CI: 1.19-2.42). Parental incarceration was not a significant predictor of ADHD. There was no evidence for a differential impact of PI based on the parent or participant’s gender.
Conclusion:
PI is associated with negative effects, including higher rates of depression and PTSD, through mid-life. This same relationship did not exist for ADHD and gender did not moderate the relationship between PI and mental health outcomes. These findings extend knowledge on the possible long-term harms of criminal justice involvement, and are especially important for communities disproportionately affected by incarceration in the United States.
Introduction
The United States has the highest incarceration rate in the world with a rate of 639 per 100,000 adults. 1 This rate has increased by around 500% over the past 30 years, following the rise in mandatory sentencing, with penal severity increasing despite a decrease in crime.2,3 There are around 143,950 inmates housed in federal prisons for a wide variety of crimes; drug offenses (43.4%), weapons/explosions/arson use (22%), sex offenses (13.5%), and burglary/larceny/property offenses (5%) are the 4 most common crimes. 4 More than 5 million children in the U.S. have had a parent incarcerated at some point in their lives 5 contributing to a substantial social, economic, and public burden.
Parental incarceration (PI) is one of the now well-researched “adverse childhood experiences” (ACEs), which are traumatic events that occur in childhood and strongly predict physical and mental health outcomes across the life course. 6 In this study, “child” is defined as any individual under the age of 18. ACEs not only are associated with poor physical and mental health outcomes in adulthood but demonstrate a dose-response relationship between the extent of childhood trauma exposure and subsequent adult risk behaviors and health concerns. Incarceration of a parent can be sudden and traumatic, as is the chronic stress of separation, and limited communication regarding cause of a parent’s departure. Previous research also suggests that individuals experiencing PI are also at increased risk for other ACEs, potentially because many ACEs (e.g., substance use, violence in household) may directly lead to the parent’s arrest. 7 While a substantial body of research has demonstrated the impact of current PI on child emotional and physical wellbeing, research on the long-term effects of PI beyond childhood is needed.
Consistent with previous literature on ACEs, children experiencing PI show increased internalizing (e.g., anxiety) and externalizing (e.g., aggression) behavioral health symptoms, as well as increased risk for depression or post-traumatic stress disorder (PTSD) diagnoses.5,8 In an early study, 20% of mothers reported an increase in behavioral issues for their children during their father’s imprisonment, including impulsivity, delinquency, and academic difficulties. 9 These same behaviors are also correlated with an attention deficit/hyperactivity disorder (ADHD) diagnosis, which suggests a possible relationship between PI and ADHD. 10 In addition to the emotional stress of losing a parent, there are social factors that may exacerbate the impact of PI on children. Families with PI are often burdened with financial hardships due to the loss of income, social stigma, and housing insecurity. 8
Beyond the individual impact of PI on mental health, previous research suggests the gender of the parent and child may also predict the severity of psychological and behavioral problems associated with experiencing PI during childhood. Previous research suggests that incarceration of the mother is particularly harmful to child health, potentially because mothers provide a substantial amount of caregiving activities in the U.S. Children of incarcerated mothers are more likely to be rehomed.11,12 Additionally, previous research has found children experiencing maternal incarceration to score lower in math and literacy, with adolescent girls at a higher risk for substance-exposed pregnancies, sexually transmitted infections, and Human Immunodeficiency Virus.13,14 Alternatively, paternal incarceration has been found to predict future rule breaking behaviors more than any other type of father loss.15,16 While there seem to be extant findings on the impact of maternal and paternal incarceration, research comparing the 2 is extremely limited.
In addition to potential differences in health outcomes by parent gender, research has also pointed to the possibility of distinct responses to PI based on child gender. Gabel 17 also found gendered behavioral issues; boys more often displayed aggression, hostility, and drug use, while girls more often displayed regression, fearfulness, and nightmares after experiencing PI. Gendered differences may be a reflection of each group’s social norms rather than biological mechanisms shaping behavioral outcomes secondary to PI. Similar to research on parental gender, there has been no research comparing the long-term impact of PI for male and female children.
PI is a known adverse childhood experience, but there are important gaps in understanding its full impact across the life course. Research is specifically needed on specific mental health diagnoses, rather than symptoms, and the role of both parental and child gender in shaping long term outcomes. Most existing studies have only examined how PI affects mental health and behavior during the period of incarceration, rather than into mid-life. Stability in childhood is crucial for healthy development, and we seek to understand how incarceration through the age of 18 can predict mental health outcomes up to the fourth decade of life.
This study aims to explore how PI negatively impacts mental health and, specifically, diagnoses of ADHD, PTSD, and depression. Among children who have experienced PI, we explore the gender of the parent and child as moderators of 3 primary mental health outcomes. Using data from a single wave of the US National Longitudinal Survey of Adolescent to Adult Health, we hypothesized that (1) individuals who experienced PI would have higher rates of ADHD, PTSD, and depression, and (2) the gender of the parent and child would differentially relate to future mental health outcomes.
Methods
Participants and Data Sources
We analyzed free, public-use data from the National Longitudinal Study of Adolescence to Adult Health, a 5-wave study that utilized in-home interviews to collect demographics, economic, social, psychological, and health survey data. The portion of this dataset that is public use is representative of the larger dataset. As a result, no weights were applied as we employed a simple, cross-sectional design. This study used data primarily from Wave V, collected between 2016 and 2018, with the exception of data on ADHD/Attention Deficit Disorder (ADD) diagnoses data which were only measured in the Wave IV dataset collected in 2008. Due to Wave IV data collection on attention deficit/hyperactivity disorder taking place in 2008, before the term was updated from “ADD” to solely “ADHD” in 2013 with the release of the DSM-V, the diagnosis is referred to as “ADD” in the dataset. 18 To avoid confusion while remaining consistent with the dataset, we will refer to the diagnosis as “ADHD/ADD.” Participants who experienced PI after childhood (after age 18) were removed from the dataset. Participants who received a diagnosis of depression or PTSD prior to experiencing PI were also removed. Due to limitations in the dataset, diagnoses of ADHD/ADD that occurred before the period of PI could not be dropped. We excluded any participants who responded to the ADHD/ADD diagnosis question in Wave IV but did not continue to Wave V. The initial dataset had n = 5114 participants, and after exclusions and employing listwise deletion to address missing data, we analyzed data from 3875 adults.
Measures
Dependent Variables: Diagnoses
Participants were asked about previous mental health diagnoses and all variables were measured dichotomously based on whether the participant had received a professional diagnosis from a healthcare provider or not (1 = YES, 0 = NO). The questionnaire measured participants’ diagnostic history of ADHD/ADD (“Has a doctor, nurse or other health care provider ever told you that you have or had: attention problems or ADD or ADHD?”), PTSD (“Has a doctor, nurse or other health care provider ever told you that you have or had post-traumatic stress disorder or PTSD?”), and depression (“Has a doctor, nurse or other health care provider ever told you that you have or had depression?”).
Parental Incarceration
Our focal independent variable was whether participants had experienced the incarceration of a parent or parent figure before age 18. The questions “(Has/did) your biological father ever (spent/spend) time in jail or prison?” and “(Has/did) your (father figure) ever (spent/spend) time in jail or prison?” were combined into a single variable which measured paternal incarceration. Similarly, the survey asked “(Has/did) your biological mother ever (spent/spend) time in jail or prison?” and “(Has/did) your (mother figure) ever (spent/spend) time in jail or prison?” However, while n = 99 participants reported having their biological mother spend time in jail/prison, no participants had a mother figure (non-biological parental figure) incarcerated while under the age of 18 and as a result, we did not combine the maternal variables in the same way, opting to only use the data regarding biological mothers. Therefore, the variable “Paternal Incarceration” refers to the incarceration of a biological father or father figure while under the age of 18, and the variable “Maternal Incarceration” refers to the incarceration of only a biological mother while under the age of 18.
The final parental incarceration variable was defined as those who experienced the incarceration of a parent or parent figure when under the age of 18 and was constructed by limiting the participants in the PI group to those who indicated in a separate question (“How old were you when your biological father/father figure/biological mother went to jail or prison (the first time)? [years]”) that their parent was incarcerated for the first time while they were under the age of 18. Individuals who experienced PI, but indicated that they were over the age of 18 when their parent was first incarcerated, were not included in the sample.
Control Variables
Six control variables were utilized: sex assigned at birth, educational attainment, race, alcohol use, marijuana use, and history of sexual abuse. All variables were coded dichotomously. Educational attainment measured socioeconomic status, with those who had completed an Associate’s degree or higher coded as “1” and those who had not coded as “0.” For alcohol use, those who self-reported drinking more than once a week were coded as “1” and those who self-reported less once a week were coded as “0.” For marijuana use, those who self-reported using more than once a week were coded as “1” and those who self-reported less than once a week were coded as “0.”
Race and ethnicity were measured via self-identification. Participants were able to mark one or more boxes. For this study, the racial variables were coded as “Black” or “Not Black,” with “Black” including individuals who identified as Black among their responses and “Not Black” including individuals who did not, regardless of all other races identified. For example, if someone selected Black, White, and Hispanic, they would be coded as “Black.” If someone identified as “White, Hispanic, and Asian,” they would be coded as “Not Black.” We constructed race as a binary variable due to the disproportionate number of Black people incarcerated in the United States. 19
Procedure
A chi-square test of independence was run with every combination of PI (parental incarceration, paternal incarceration, maternal incarceration, and no parental incarceration) and adult ADHD, PTSD, or depression diagnoses, and then tested again with different combinations of parent and participant gender (girls with fathers incarcerated, girls with mothers incarcerated, boys with fathers incarcerated, and boys with mothers incarcerated). No test including the variable of ADHD diagnosis produced statistically significant results, and thus the variable was removed from further analyses. The dependent variables that yielded significant results, participant PTSD and depression diagnoses, were then tested with binary logistic regression, with the aforementioned control variables implemented. We also explored the relationship between participant gender, parental gender, and PI using interaction terms in a separate logistic regression model. We used the variance inflation factor to test for multicollinearity among our independent variables in all regression variables and all models were in the acceptable range. Statistical tests were run with Stata 15.1.
Results
Descriptive Statistics of Sample
Age was measured in the National Longitudinal Study of Adolescence to Adult Health dataset at the time of the Wave V data collection, with Mage = 37.32. Of the 3875 participants, 21.1% identified as Black and 78.9% did not. Additionally, 448 (11.4%) participants had a father or father figure incarcerated in jail or prison while they were under the age of 18. Ninety-two participants (2.3%) had a mother incarcerated in jail or prison while they were under the age of 18 (Table 1).
Descriptive Statistics (n = 4196).

Frequency of Parental Incarceration by Race and Sex
Cross-tabulation analysis was used to determine the frequency of participants experiencing PI by population. Of the Black participants, 28.63% (n = 144) experienced PI when under the age of 18, compared to 11.62% (n = 359) of non-Black participants. Of the male participants, 12.43% (n = 210) experienced PI when under the age of 18, compared to 13.09% (n = 293) of female participants.
Chi-Square Test of Independence
Statistically significant results were found for PI and participant depression diagnosis (X2 (1, N = 3917) = 41.76, P < .001) and PI and participant PTSD diagnosis (X2 (1, N = 3915) = 27.35, P < .001) (Table 2). PI and participant ADHD diagnosis did not yield statistically significant results (X2 (1, N = 3482) = 0.81, p = .367). Notably, no statistically significant differences were found when assessing different combinations of parent and participation gender (Table 2).
Chi-Square Test of Independence of Diagnosis Outcomes (n = 4196).
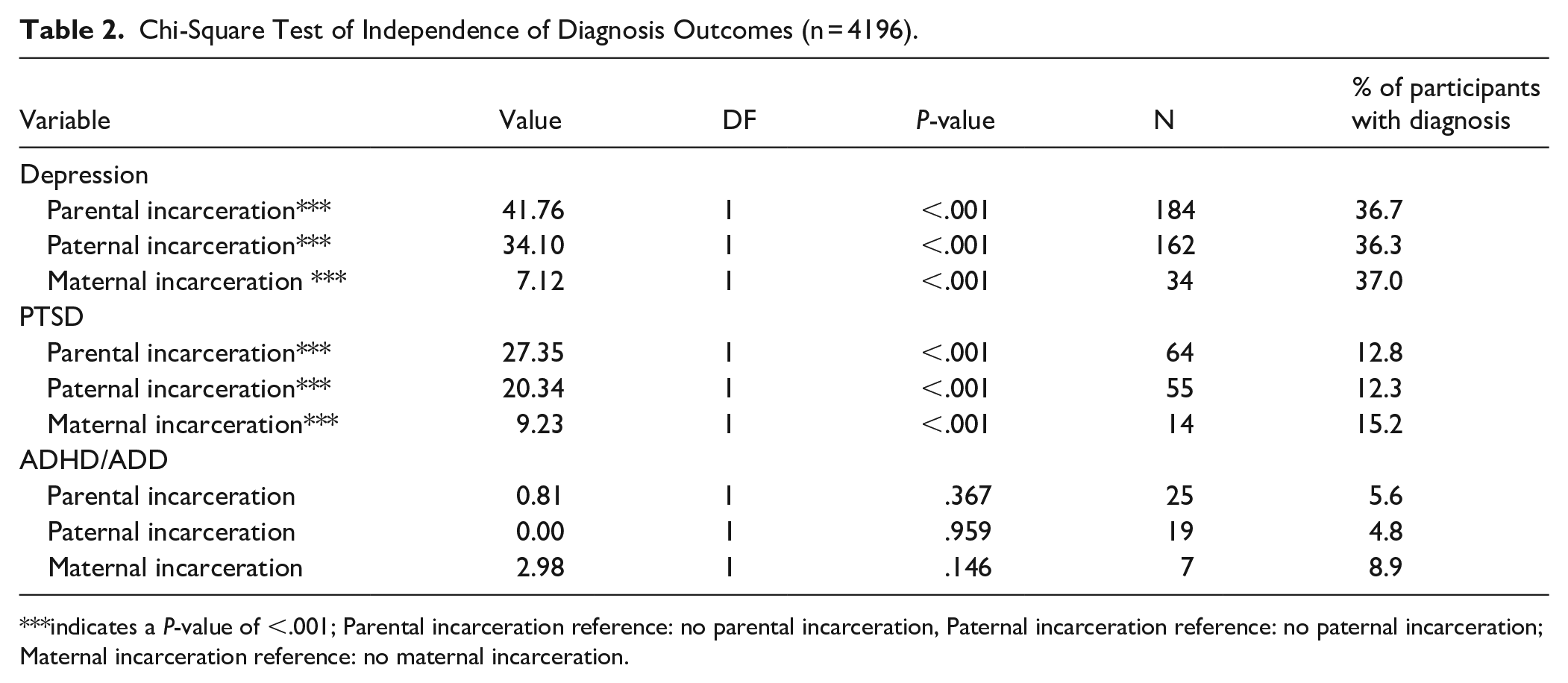
indicates a P-value of <.001; Parental incarceration reference: no parental incarceration, Paternal incarceration reference: no paternal incarceration; Maternal incarceration reference: no maternal incarceration.
Binary Logistic Regression
We fitted 2 binary logistic regression models with participant depression (Model 1) and PTSD (Model 2) diagnoses as the respective dependent variables and PI as the focal independent variable (Table 3). In Model 1, participants who had a parent incarcerated during childhood had 1.83 times higher odds of depression, independent of covariates. Female participants also had higher odds of depression (OR: 1.78, P < .001) as did participants with a history of sexual abuse (OR: 2.77, P < .001) and individuals who endorsed using marijuana (OR: 1.66, P < .001). Individuals who identified as Black (OR: .54, P < .001) and individuals who endorsed alcohol use (OR: .81, P = .011) had lower odds of having a depression diagnosis. In Model 2, parental incarceration during childhood was associated with 1.94 times higher odds of PTSD (P < .001). Participants with a history of sexual abuse (OR: 3.89, P < .001) and those who endorsed marijuana use (OR: 2.44, P < .001) also had higher odds of PTSD. Participants who endorsed alcohol use, by contrast, had lower odds of PTSD (OR: .53, P < .001). A third and fourth model were run to assess the interaction between child and parent gender on depression and PTSD diagnoses, but no statistically significant differences were found (Table 4).
Multivariable Logistic Regression of Diagnosis Outcomes (n = 4196).

Abbreviations: OR, odds ratio; SE, standard error; VIF, variance inflation factor.
Indicates a P-value of <.05. ***indicates a P-value of <.001.
Multivariable Logistic Regression of Diagnosis Outcomes by Gender (n = 4196).

Abbreviations: OR, odds ratio; SE, standard error; VIF, variance inflation factor.
indicates a P-value of <.05. **indicates a P-value of <.01. ***indicates a P-value of <.001.
Discussion
This study aimed to assess the relationship between parental incarceration during childhood and adult mental health diagnoses. Our results suggest that experiencing PI as a child is associated with approximately twice the odds of later being diagnosed with PTSD and depression, independent of race and known predictors of these mental health diagnoses. PI was not associated with later diagnoses of ADHD. We also did not find support for differential impacts of parental incarceration by gender of the parent or child, suggesting that this event is traumatic regardless of an individual’s gender or the familial role played by the separated parent.
Previous research has demonstrated that PI is a known adverse childhood experience. The traumatic nature of PI likely results from child separation from the parent and is often compounded by a lack of clear communication explaining the separation.12,20 Children who witness an arrest may also be at increased risk, as police are often not trained in child welfare. 21 Children whose parents are incarcerated are also often displaced resulting in increased instability during childhood. 11
It is important to note that after adjusting for childhood parental incarceration, Black participants had lower odds of depression which mirrors other studies in the literature. Although Black Americans had lower odds of being diagnosed with depression, this does not accurately reflect the real burden of depression given racial disparities in treatment access and diagnosis. Existing research suggests that Black Americans may actually have higher rates of chronic and debilitating depression despite less frequent depression diagnoses. 2 Given the disproportionate incarceration of Black Americans, a rate that is 6 times higher than their white counterparts, these disparities suggest that Black Americans may be at increased risk of mental health consequences from childhood parental incarceration, even later in life. 22 Future research should focus on measuring depression symptoms rather than diagnoses to accurately compare the impact of PI across racial/ethnic groups.
Children of color are overrepresented in the criminal justice system, as they make up 72% of children with incarcerated parents despite only making up 48% of children as a whole. 23 National statistics on race and incarceration rates suggest that associated mental health impacts may also disproportionately affect Americans of color. Although the true impact of this early life experience may be concealed by lower diagnosis and treatment access, childhood parental incarceration should be understood as another manifestation of structural racism that contributes to racial/ethnic health disparities into mid-life.
Limitations and Future Directions
This study contains several limitations, the majority of which are due to the limited scope of the National Longitudinal Study of Adolescence to Adult Health dataset. For the variables PTSD and depression, we were able to limit participants to those who received the diagnosis after experiencing PI. However, the variable of ADHD/ADD was not measured in Wave V, and when measured in Wave IV the participants were not asked about the age of diagnosis. Due to this, there are most likely participants in the sample who were diagnosed with ADHD/ADD before ever experiencing parental incarceration. Due to limitations with the variable of ADHD/ADD, we excluded it from most statistical analyses.
The dataset also does not differentiate between incarceration in prison versus jail, which would have allowed for more in-depth analysis and comparison between different types and lengths of incarceration. When asking whether a participant had a parent incarcerated, the dataset does not measure the length of incarceration. This means that a participant who had a parent incarcerated for 3 days and a participant who had a parent incarcerated for 3 years were treated equally. Future research should assess the incarceration setting as well as the length of incarceration as predictors of future mental health.
The use of PTSD and depression diagnoses as variables, compared to symptoms, also presents limitations. Individuals who could not access professional treatment are overlooked in this sample. Given that experiencing PI is often correlated with financial hardship, this likely resulted in an underrepresentation of depression and PTSD in our sample. There are also documented racial biases in the diagnosis of mental health conditions, including depression, and PTSD which could further limit the validity of these measures. 24
The accessibility of ADHD diagnoses may explain the lack of a statistically significant relationship between ADHD diagnosis and PI. People of color are disproportionately represented in the criminal justice system and among children with incarcerated parents. A racial bias has been found between ADHD and oppositional defiant disorder (ODD) diagnosis, suggesting that Black children are overdiagnosed with ODD and underdiagnosed with ADHD, which leads to worse life outcomes. 25 Future studies should measure symptoms in addition to diagnoses to allow for better measurement of this relationship.
A final shortcoming of this research and currently available studies in the field is the focus on incarceration. There is a corresponding lack of research on individuals with parents on probation or parole, or those whose parents have had encounters with the police that have not resulted in a sentence. Comparing the disparate impacts of different types of involvement with the criminal justice system on the long-term health of children affected should be a priority of future research. This research could be used to develop screening measures for children currently experiencing parental incarceration or other times of criminal justice involvement and develop early interventions to prevent mental health impacts across the life course.
Conclusion
This study found no significant relationship between PI and either child or parent gender and mental health outcomes in mid-life. These results are interesting and warrant additional research to understand the experience of PI within children and families. In particular, more research should be done on potential protective measures between genders and if they function as moderating variables. Qualitative research could be conducted to compare the different ways mothers and fathers cope and serve as caregivers in the context of their partner’s incarceration, and how these strategies impact their children’s mental health outcomes. Given the scope of PI in the U.S. and its documented relationship with mental health diagnoses, addressing the health of children experiencing PI is a critical public health priority.
Footnotes
Ethics Statement
Ethical approval was not required.
Consent to Participate
Not applicable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Research Experience for Undergraduates program from the National Science Foundation (#2050706).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.