
Abstract
Background:
This study aimed to explore clinicians’ perspectives on the current practice of perinatal mood and anxiety disorder (PMAD) management and strategies to improve future implementation.
Methods:
This study had a cross-sectional, descriptive design. A 35-item electronic survey was sent to clinicians (N = 118) who treated perinatal women and practiced at several community clinics at an academic medical center in the United States.
Results:
Among clinicians who provided care for perinatal women, 34.7% reported never receiving PMAD management training and 66.3% had less than 10 years of experience. Out of 10 patients who reported psychiatric symptoms, 47.8% of clinicians on average reported providing PMAD management to 1 to 3 patients and 40.7% noted that they conducted screening only when patient expresses PMAD symptoms. Suggested future improvements were providing training, developing a referral list, and establishing integrated behavioral health services.
Conclusions:
Results from this study indicated that while PMAD screening and management was implemented, improvements are warranted to meet established guidelines. Additionally, clinicians endorsed providing PMAD management to a small percentage of perinatal patients. Suggested strategies to increase adoption and implementation of PMAD management should be explored to improve access to behavioral health services for perinatal women.
Introduction
Depression is prevalent in 10% to 20% of women during the perinatal period. 1 Depressive symptoms have been shown to emerge prior to pregnancy (26.5%), during pregnancy (33.4%), and 4 to 6 weeks after birth (40.1%). 2 Anxiety is also highly comorbid with depression in this population3,4 with estimates of prevalence ranging widely from 2.6% to 39% of women reporting anxiety symptoms during5,6 and after pregnancy.7,8
Dire consequences of untreated Perinatal Mood and Anxiety Disorders (PMAD) have been described; for example, maternal suicide remains a leading cause of death in the postpartum period.9,10 Maternal psychiatric illness has been shown to increase risk for placental pathology, fetal growth issues, preterm delivery, disordered attachment, and adverse developmental outcomes.11-13 Additional negative childhood outcomes associated with maternal mental illness include emotional and behavioral difficulties, low levels of cognitive development, and poor physical and growth development. 14
PMAD management is defined as the provision of behavioral health assessment and intervention (eg, pharmacotherapy and psychotherapy) to perinatal women. Current recommendations for PMAD management include screening for symptoms at least once during the perinatal period, using validated screening measures, increasing frequency of visits when elevated symptoms are identified, and referring patients to appropriate pharmacotherapy and psychotherapy resources.15-17 These recommendations align with existing guidelines from the United Kingdom National Institute for Health and Care Excellence (NICE) on antenatal and postnatal mental health 18 as well as American College of Obstetricians and Gynecologists. 19
Despite PMAD management guidelines, there is a gap between these recommendations and the practice of caring for women living with PMAD. 20 A systematic review found that only 55% of physicians routinely screen for PMAD. 21 Appropriate, timely screening is necessary to capture all patients with PMAD symptoms. 22 When PMAD symptoms are elevated, clinicians reported feeling ill-equipped to initiate further intervention, provided referrals, or both. 23 Although pharmacotherapy and psychotherapy have been shown to be beneficial for women with PMAD,24,25 less than 25% of affected women receive behavioral health services tailored to PMAD.26,27 Moreover, while the majority of women preferred psychotherapy over pharmacotherapy, 28 current estimates show that 75% of pregnant women with depression are referred for pharmacotherapy only. 29
Barriers to providing PMAD management occur at different levels. Women have reported difficulty disclosing emotional distress, a desire to handle PMAD on their own, and limited knowledge of PMAD as factors that reduce their willingness to participate in treatment.30,31 Limited insurance coverage is an additional barrier to perinatal women’s participation in behavioral health services. 32 Moreover, many clinicians perceive PMAD screening as difficult to carry out in everyday practice and question whether screening improves outcomes. 33 One study found that only 15% of positively screened mothers had evidence of mental health treatment in their medical record during pregnancy, with equally low rates of referral to behavioral health or social services. In the postpartum period, 25% of positively screened mothers received treatment, and only 2.5% were referred. 34
The aims of this study were to characterize clinicians’ PMAD management training, experiences, current practices, and suggested strategies for PMAD management implementation. The present study was part of a larger quality improvement project seeking to advance the delivery of PMAD management across multicenter community practices.
Methods
This study utilized a cross-sectional, descriptive design, using an online questionnaire. This study was conducted at a not-for-profit academic medical center in the United States with multiple sites across four states. Practices across the state of Minnesota, Wisconsin, Arizona, and Florida, where branches of the medical center were located, were included in the study. Clinicians practiced in diverse settings including Family Medicine, Obstetrics and Gynecology, and Social Work.
The purpose of the questionnaire was to characterize clinicians’ PMAD management training, past experiences, current practices, and perceived strategies that might improve the adoption and implementation of improved PMAD management. Initial questions were generated and reviewed by the research team. We went through three iterations of the questionnaire. Suggested changes included adding and removing certain questions and improving grammatical errors and wordings. Our research team members took the survey draft to assure readability after each iteration. Thirty five questions were included in the questionnaire. Main sections of the questionnaire included: (1) demographics and current field of practice; (2) past training and clinical experiences in PMAD management; (3) perceived comfort to manage psychiatric diagnoses for perinatal women; and (4) recommended strategies to support future PMAD management implementation.
Clinicians practicing in the institution, who reported providing care to pregnant and/or post-partum (ie, 1 year after delivery) women, were recruited via email and provided a link to the electronic survey. Two weeks after the first invitation, a second invitation email was sent to clinicians who had not completed the survey. Clinicians completed the 10-minute questionnaire via REDcap, an online portal approved by the institution to distribute survey research.
The study protocol was approved by the institution Institutional Review Board (IRB #18-011824). Participation was voluntary and clinicians indicated their consent to participate on the virtual survey. Once the questionnaire was submitted, data was automatically encrypted and transmitted to a secure database on a server hosted within the Department of Psychiatry and Psychology. All data were treated as private and confidential. No participants indicated a wish to withdraw from the study. Descriptive statistics were generated to identify the most commonly endorsed items. Content analysis was used on the open-ended questions to identify themes in the data.
Results
The email invitation was sent to 443 clinicians. A total of 201 providers responded to the survey (45% participation rate). Fifty nine clinicians identified that they did not provide care to perinatal women and 24 clinicians opened the questionnaire but did not complete it. Thus, data from 118 clinicians were included in the final analysis (27% participation rate for completed response).
The final sample included clinicians from Minnesota and Wisconsin sites. None of the clinicians from Florida and Arizona sites responded to the survey. Clinicians came from several disciplines: Family Medicine (N = 42), Obstetrics and Gynecology (N = 35), Pediatrics (N = 1), and Social Work (N = 40). The majority (N = 92; 78%) of clinicians were women with mean age of 42.8 (SD = 9.99). Table 1 presents further demographic variables.
Demographics.

PMAD Management Training, Experiences, and Perceived Comfort
Table 1 describes clinicians’ past training and experience providing PMAD management. The majority of clinicians reported that they had received formal training, attended a workshop, or received supervision on PMAD management. A portion of the clinicians (34.7%) noted that they had never received any PMAD management training in the past. Clinicians reported that they were somewhat knowledgeable (49.2%) or moderately knowledgeable (33.9%) on PMAD management. A smaller percentage indicated that they were very knowledgeable (11%) or not at all knowledgeable (5.9%). In terms of past experiences in providing PMAD management, 66.3% reported having less than 10 years of experience.
With regard to perceived comfort, clinicians reported being somewhat comfortable (39%) or moderately comfortable (35.6%) providing PMAD management while a smaller percentage reported being very comfortable (13.6%) or not at all comfortable (5.9%). Figure 1 summarizes perceived comfort to assess and treat different psychiatric conditions. Clinicians reported feeling most comfortable treating generalized anxiety disorder, major depressive disorder, and pregnancy loss. Respondents felt least comfortable treating eating disorders, psychosis, and schizophrenia among the perinatal population.
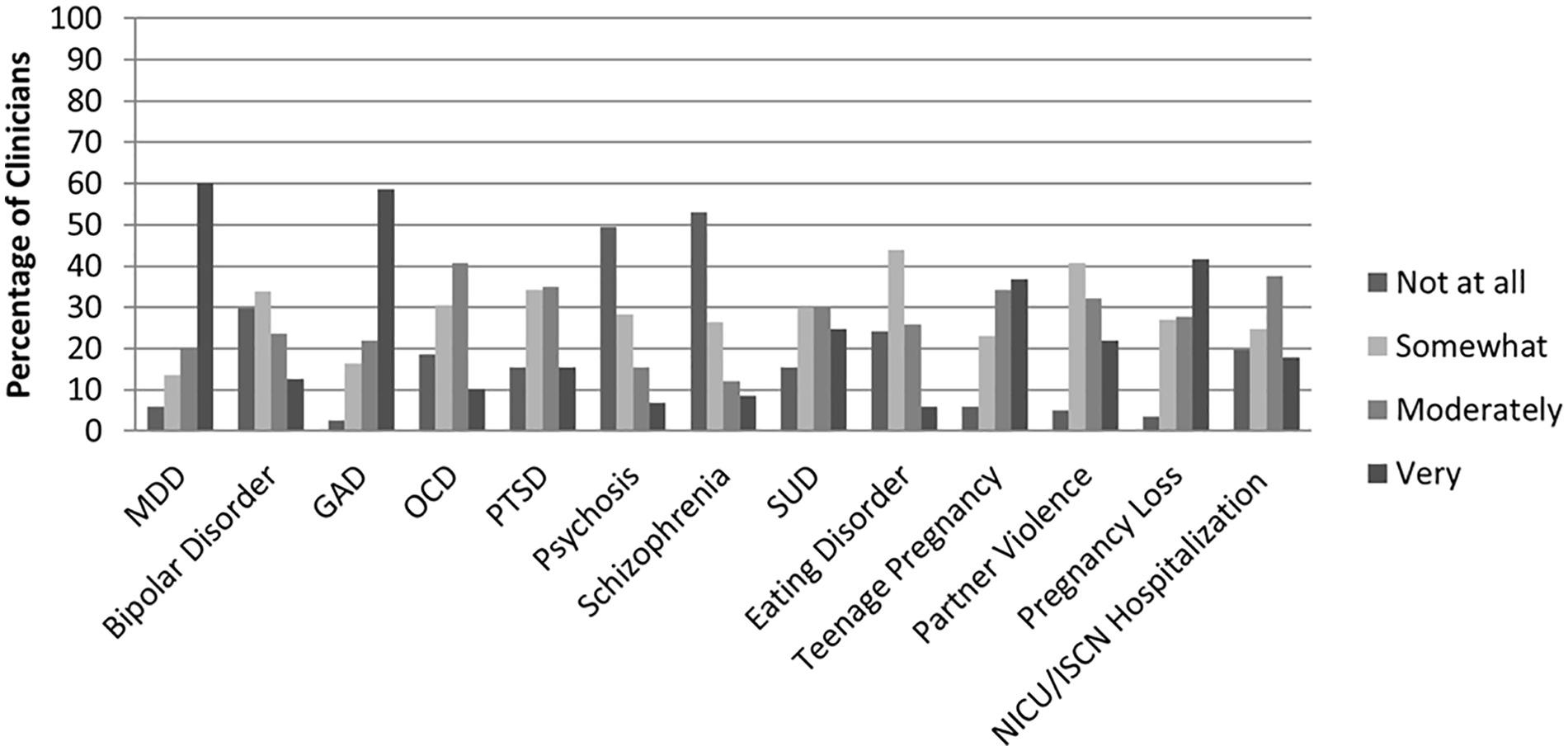
Perceived comfort to treat psychiatric and other conditions.
Current Practice of PMAD Management
Table 2 describes current PMAD management practices. We asked, “Out of 10 patients with PMAD, to how many women do you provide PMAD management?” Among respondents, 47.8% reported that they provided PMAD management to 1 to 3 patients, 20% to 4 to 6 patients, 21.7% to 7 to 9 patients, and 10.4% to all 10 patients. When asked, “to what extent do you manage PMAD in your clinical practice?” most clinicians provided some PMAD management with 7.6% noted that they did not provide any PMAD management.
Current Practice of PMAD Management.

We assessed the degree to which clinicians conduct mental health screening in their practice. We asked, “How often do you administer standardized self-report measures?” The top three selected time points were when patient expresses PMAD symptoms (40.7%), other (26.3%), and postpartum only (23.7%). The three least selected time points were all prenatal visits (5.1%), all prenatal and postnatal visits (5.9%), and intend to screen but it is not always completed (7.6%). The top three most commonly used patient reported outcome (PRO) measures were Patient Health Questionnaire 9-items 35 (PHQ-9; 75.4%), Generalized Anxiety Disorder 7-items 36 (GAD-7; 63.6%), and Edinburgh Postnatal Depression Scale 37 (EPDS; 41.5%).
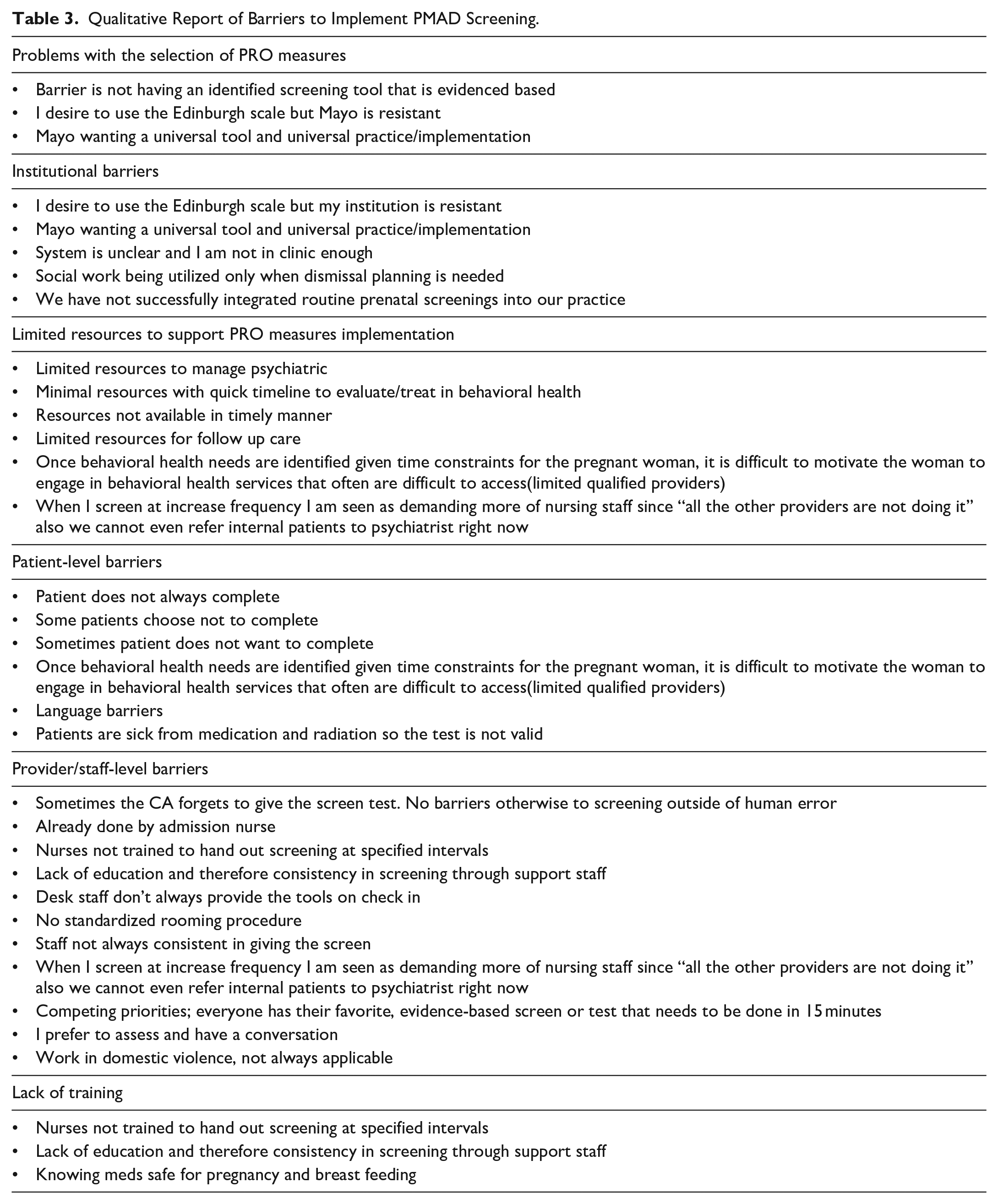
Barriers to screening for psychiatric symptoms were assessed and the top three reported barriers were unspecified barriers (24.6%), lack of time (22.9%), and no resources to refer patients with psychiatric concerns (16.9%). Since “other” was the most commonly endorsed, qualitative response was further analyzed. Table 3 presents other barriers reported by providers, which include problems with the selection of PRO measures, institutional barriers, limited resources to support PRO measures implementation and PMAD management, patient-level barriers, provider/staff level barriers, and lack of training.
Qualitative Report of Barriers to Implement PMAD Screening.
We further assessed the next steps that clinicians took when patients reported elevated psychiatric or psychological symptoms. The top three selected options were, “I provide further evaluation” (80.5%), “refer to mental health clinic/agency” (66.9%), and “I provide further treatment” (66.1%).
Suggested Strategies to Improve Future PMAD Management
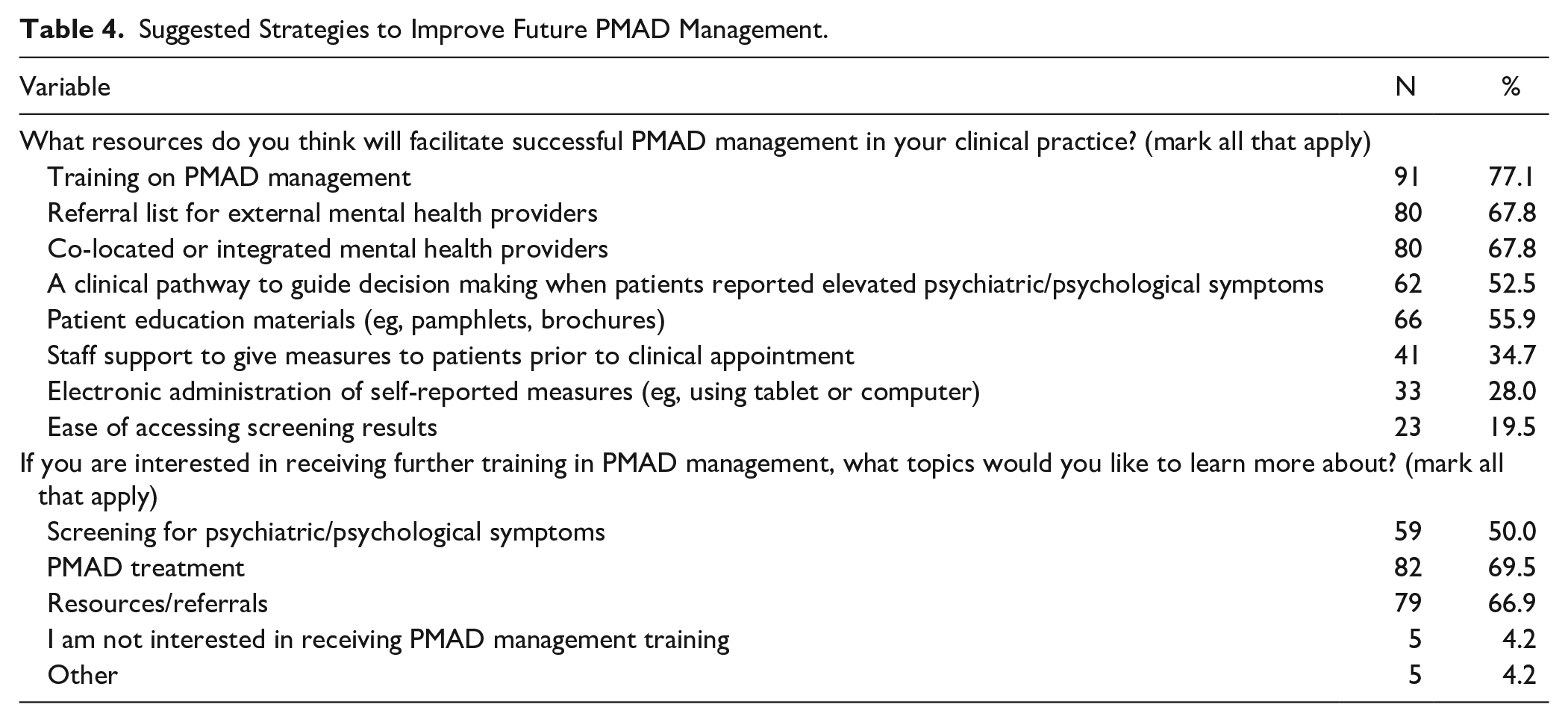
Clinicians rated factors that may promote successful implementation of PMAD management in their clinical practice (Table 4). The top three facilitators were receiving PMAD management training (77.1%), receiving referral list of behavioral health services in the area (67.8%), and having co-located behavioral health clinicians in their clinic (67.8%). Furthermore, clinicians were asked to rate topics to include in future PMAD management training that would be relevant to their practice. The top three training topics of interest were PMAD treatment (69.5%), resources and referrals (66.9%), and screening for psychiatric diagnosis (50%).
Suggested Strategies to Improve Future PMAD Management.
Discussion
The present study explored clinician perspectives on PMAD training, assessment, and management and suggests strategies to improve future practice. We support and extend research on PMAD management by integrating clinician perspectives across clinical practices where perinatal women receive health services (eg, family medicine, obstetrics and gynecology, pediatrics, and social work). Findings from this study demonstrate deficiencies in PMAD training and experience among clinicians involved in perinatal care. While some clinicians reported receiving a formal training on PMAD management (41.5%) and had PMAD management supervision (26.2%), the rest indicated that they never received training on PMAD management (34.7%) or only attended one workshop in the past (21.2%). This suggests that more than half of clinicians who provide perinatal care may benefit from receiving further training and supervision on the management of PMAD.
These findings echo previous reports that clinicians lack access to training and resources specific to the management of perinatal mental health concerns.38-40 The importance of providing training and supervision specific to the management of PMAD is beginning to receive more attention and has been identified as a critical step toward improving access to comprehensive care for this patient population. 41 Past studies have noted that many women perceived their clinicians to be inadequate in this area,42,43 highlighting the importance of implementing routine training in the assessment and treatment of PMAD for improving clinical outcomes. 44
A notable subset of clinicians (40.7%) reported utilizing standardized PRO measures only when patients expressed PMAD symptoms. This finding is consistent with previous studies describing heterogeneous, and in some cases nonexistent, screening for PMAD symptoms. 21 These trends suggest that many women in need of behavioral health services are not assessed and possibly do not receive adequate treatment. Additionally, only a small percentage of providers reported administering PRO measures at all prenatal visits (5.1%) which departs from current guidelines recommending that perinatal women with elevated psychiatric and psychological symptoms be assessed more frequently. 19
Our findings support the argument for the increased use of validated measures given that, in the absence of systematic screening, most women with elevated depression and anxiety symptoms are not adequately detected by clinicians. 45 An essential next step in the management of PMAD will be to implement systematic screening practices to ensure that perinatal women living with PMAD are identified and connected to adequate care. Moreover, out of 10 perinatal women who expressed PMAD symptoms, about half of the clinicians (47.8%) reported only providing PMAD management to 1-3 women. This could yield several interpretations. First, these clinicians might provide referrals to external behavioral health services for the majority of their patients with PMAD symptoms since 66.9% of them noted that they “refer patients to mental health clinic/agency.” Though, it is also possible that most women do not receive adequate treatment or referral, given that current evidence indicates that less than 25% of women with PMAD receive behavioral health services.26,27 Future studies should explore the extent to which women with PMAD symptoms receive behavioral health services and the barriers to adequate treatment or referral to external services.
Clinicians across specialties reported a desire to receive additional training in the assessment, diagnosis, and treatment of PMAD. They also expressed interest in improving coordination and follow-up of PMAD care through the use of referral lists detailing multidisciplinary services and local providers with PMAD treatment experience. Integrated behavioral health service were also highlighted as a key systems-level change that would meaningfully reduce barriers to PMAD treatment.
There are a number of limitations that may restrict generalizability of this study. First, the sample was comprised of clinicians from one academic health center. Furthermore, no clinicians from the health system’s Arizona and Florida sites responded to the survey invitation. This limits the generalizability of findings to institutions with differing organizational structures, climates, and resources. Furthermore, our response rate was lower than average at 45% for those who started the survey and 27% for those who completed the survey. 46 Strategies to improve survey completion should be considered, which may include engaging leadership and institutional support to encourage research participation, providing incentive for completing the questionnaire, and extending data collection time frame to allow for additional reminders for survey completion.
Conclusion
This study sheds light on the current state of PMAD training, assessment, and management. While many clinicians reported having adequate training, experiences, and endorsed providing some PMAD management to perinatal women, half of the participating clinicians could benefit from receiving further training and resources to support perinatal women with PMAD. Findings indicate the need to provide adequate resources such as referral lists and co-located behavioral health clinicians in practices where women with PMAD seek care. Our study sets the stage for additional research on the implementation strategies needed to effectively advance current PMAD management practices.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors whose names are listed in this manuscript certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval Statement
This research was approved by the Mayo Clinic Institutional Review Board and written consent was exempt and not obtained from participants.