
Abstract
Background:
The hypertriglyceridemic-waist phenotype (HTWP), defined by concurrent hypertriglyceridemia and increased waist circumference, is a recognized marker of metabolic and cardiovascular risk. While extensively studied across populations, data on Amerindian communities remain scarce. This study examines HTWP prevalence and its association with type 2 diabetes mellitus in middle-aged and older adults of Amerindian ancestry in rural Ecuador.
Methods:
This population-based cross-sectional study was conducted in 3 ethnically homogeneous villages. Participants aged ≥40 years underwent standardized assessments, including structured interviews and fasting blood tests. HTWP was defined using serum triglyceride levels ≥150 mg/dL together with increased waist circumference determined by 2 criteria: Amerindian-specific (men ≥ 89 cm, women ≥83 cm) and NCEP-ATP III (men ≥102 cm, women ≥88 cm). Logistic regression models assessed associations between HTWP and diabetes indicators, adjusting for demographics and cardiovascular risk factors.
Results:
Among 1354 participants, HTWP prevalence was 47% by Amerindian-specific, and 30% using NCEP-ATP III criteria. Hypertriglyceridemia was frequent (55%), particularly in men. In multivariate models, HTWP was associated with fasting glucose ≥126 mg/dL under both Amerindian-specific (OR 1.32, 95% CI 1.02-1.71) and NCEP-ATP III (OR 1.50, 95% CI 1.12-2.01) criteria. When HTWP components were separately included in the models, only hypertriglyceridemia remained significantly associated with diabetes risk. No significant association was observed between HTWP and HbA1c levels.
Conclusion:
HTWP prevalence is high in this population. Hypertriglyceridemia drives diabetes risk more than waist circumference. Findings underscore the need for ethnicity-specific cardiovascular risk assessments and targeted health interventions for indigenous communities.
Keywords
Introduction
The hypertriglyceridemic-waist phenotype (HTWP), defined by the concurrent presence of abdominal obesity and elevated triglyceride levels, has been widely studied as a marker of cardiovascular and metabolic risk.1 -5 While associations between this phenotype and various health outcomes have been documented across diverse races and ethnic groups, there is a gap in research focusing on Amerindian populations, where evidence is limited.6 -8 Genetic predispositions and other factors unique to this ethnic group may influence the prevalence and implications of HTWP, underscoring the need for population-specific studies.
In Ecuador, indigenous populations living in rural settings predominantly exhibit Amerindian ancestry, as evidenced by phenotypic characteristics and genomic studies.9,10 In addition, these communities maintain distinct lifestyles and environmental exposures, including traditional dietary patterns and limited healthcare access, which may also shape metabolic health. Given the known influence of genetic background on modeling the metabolic risk, examining HTWP within this ethnic group is essential for identifying potential differences in cardiovascular risk factors compared to other populations.
This study aims to assess the prevalence of HTWP among middle-aged and older adults of Amerindian ancestry in rural coastal Ecuador. In addition, it intends to evaluate its association with traditional cardiovascular risk factors, particularly type 2 diabetes mellitus, to better understand how ethnicity may influence these relationships. By addressing a critical gap in metabolic health research, these findings could contribute to more effective risk stratification by improving the classification of individuals based on metabolic risk profiles. This enhanced stratification may help identify high-risk subgroups more accurately, informing targeted prevention strategies and optimizing cardiovascular risk assessment for underserved Amerindian communities
Methods
Study Population
This study was conducted in community-dwelling older adults residing in 3 neighboring rural villages located in coastal Ecuador. The population is ethnically homogeneous, consisting of indigenous Ecuadorians, as evidenced by their phenotypic characteristics, including olive-moderate brown skin (Type IV in the Fitzpatrick scale), short stature, dark brown eyes and hair, and a predominantly elliptic hard palate. 9 Genome-wide analysis supports the ethnicity, indicating a predominantly Amerindian ancestry (94.1%). 10 Most of the study population has low levels of education and socio-economic status, sharing dietary habits characterized by a diet rich in oily fish, vegetables, and carbohydrates, but low in other meats, dairy products and processed foods. 11
Study Design
Following a population-based cross-sectional design, community-dwellers aged ≥40 years who were actively participating in a large population-based study cohort as of June 2024, were identified through a door-to-door survey and invited to participate. Eligible individuals underwent structured interviews and procedures to assess demographics, levels of education, cardiovascular risk factors, and blood tests for relevant biomarkers. Data was not imputed in any case, and individuals who did not complete all required interviews and tests were excluded. Research was conducted following the ethical principles of the Declaration of Helsinki. All individuals signed a comprehensive informed consent before enrollment. The study was approved by an international accredited Ethics Committee. Aggregated data will be available from the corresponding author upon reasonable request.
Independent Variable
The exposure variable was HTWP, defined by the concurrent presence of elevated serum triglyceride levels and increased waist circumference. Blood samples were collected in a fasting state to determine serum triglyceride levels. Samples were centrifuged on the field and transported on ice to the laboratory of our Institution for processing. Serum triglyceride levels were analyzed using the COBAS® c 501 Automatic Analyzer (Roche Diagnostics, Mannheim, Germany), with values of ≥150 mg/dL classified as elevated according to standardized guidelines.
Waist circumference was measured at the midpoint between the last rib and the iliac crest using a stretch-resistant tape. Measurements were taken in fasting state, with participants wearing only undergarments, in a standing position with weight evenly distributed. 12 Waist circumference was independently measured by 2 investigators and the average of these values were used by analysis.
Two distinct cutoffs were used to define increased waist circumference: one specific to Amerindian populations, which classifies increased waist circumference as ≥89 cm for men and ≥83 cm for women, 13 and one proposed by the National Cholesterol Education Program (NCEP) Adult Treatment Panel III (ATP III), which classifies increased waist circumference as ≥102 cm for men and ≥88 cm for women. 14 Elevated triglyceride levels were defined as ≥150 mg/dL across both constructs. As the most widely recognized framework for HTWP, NCEP-ATP III was included to facilitate data comparisons across both constructs. Additionally, we examined the association between waist circumference, used as a continuous variable, to minimize potential misclassifications caused by predetermined cutoffs selections.
Dependent Variable
Type 2 diabetes mellitus was selected as a cardiovascular risk indicator for assessing its association with HTWP. According to the American Diabetes Association, 15 the diagnosis was based on fasting serum glucose levels ≥126 mg/dL on 2 separate occasions (usually 2-3 days apart), or glycated hemoglobin (HbA1c) levels ≥6.5%. Blood samples for serum glucose and HbA1c determinations were sourced from the same collection used for triglyceride assessments, using the previously mentioned COBAS® c 501 analyzer. We did not use “random” glucose determinations since all samples were obtained after a fasting state of at least 8 h. Likewise, the oral glucose tolerance test was not used because of logistical challenges during the survey. Blood samples used for HbA1c and glucose determinations (in all cases) were sourced from the same collection used for triglyceride assessments, using the COBAS® c 501 analyzer.
Covariates
Demographics, levels of education (primary school education or higher), and traditional cardiovascular risk factors based on the Life’s Essential 8 construct of the American Heart Association, 16 were selected as covariables because of their relevance to the occurrence of type 2 diabetes mellitus. Demographics and levels of education were assessed by self-report. The Life’s Essential 8 construct evaluates 8 health metrics that include: diet (according to the Dietary Approaches to Stop Hypertension [DASH] score), physical activity, nicotine exposure, sleep health (nighttime sleep duration), body mass index (BMI), blood lipids (HDL and total cholesterol), blood glucose (fasting glucose + HbA1c), and blood pressure (systolic and diastolic). The “blood glucose” metric—included in Life’s Essential 8 construct—was excluded as a covariable for analysis since type 2 diabetes mellitus was the dependent variable.
Statistical Analysis
Data analysis was carried out using STATA version 18 (College Station, TX, USA). In unadjusted analyses, continuous variables were compared using linear models and categorical variables by using the chi-square or Fisher exact test, as appropriate. Several logistic regression models were fitted to assess the association between HTWP and type 2 diabetes mellitus, after adjusting for all confounders. Models separately evaluated the association of the 2 constructs of interest (Amerindian-specific construct and the NCEP-ATP III) as well as a third construct using continuous values of waist circumference as independent variables, and the 2 biomarkers for type 2 diabetes mellitus diagnosis (fasting serum glucose levels and HbA1c) as dependent variables.
Results
Selection of Participants
Of the 1838 individuals aged ≥40 years enrolled in this cohort, 1408 (77%) were actively participating as of June 2024 and signed the informed consent. The remaining 430 had died, emigrated, or declined consent before data collection. In addition, 54 eligible candidates were excluded due to a history or prior diagnosis of type 1 diabetes mellitus, uncontrolled metabolic disorders, advanced liver disease, chronic renal failure, or cancer. Following this selection process, 1354 participants remained in the study. Included individuals were younger, were less frequently women, and had higher levels of education compared to those excluded (all differences at the P < .01 level).
Characteristics of the Study Population
Table 1 depicts clinical and laboratory characteristics of the study population. The mean age of participants was 60.4 ± 12.6 years, 798 (59%) were women, and 724 (54%) had only primary school education. According to the Life’s Essential 8 criteria and proposed cutoffs (Supplemental File 1) for defining each of the health metrics in a low range. Participants with poor individual health metrics included those who: 1) had Dietary Approaches to Stop Hypertension (DASH) scores below the 25 percentile (n = 489; 36%), 2) reported ≤29 min of moderate to vigorous physical activity per week (n = 30; 2%), 3) were current smokers or had quit <1 year age or were currently using inhaled nicotine delivery systems (n = 83; 6%); 4) had a nighttime sleep duration <6 or >10 hours (n = 481; 36%), 5) had a body mass index (BMI) ≥30 kg/m2 (n = 417; 31%), 6) had non-HDL cholesterol levels ≥160 mg/dL (n = 513; 38%), and 7) had ≥140 mmHg systolic or ≥90 mmHg diastolic pressure (n = 420; 31%). As previously mentioned, the metric “blood glucose” was not considered among these covariables.
Clinical and Laboratory Characteristics of 1354 Participants of this Study.

Mean serum triglyceride levels were 187 ± 108 mg/dL, with 750 participants (55%) exhibiting ≥150 mg/dL, indicating high levels. Hypertriglyceridemia was more frequent in men (61%) than in women (52%). An increased waist circumference was observed in 1065 participants (79%) based on Amerindian-specific cutoffs and in 678 participants (50%) based on NCEP-ATP III criteria.
According to Amerindian-specific cutoffs, 630 participants (47%) exhibited HTWP, with similar distribution between sexes (46% of women and 48% of men). By contrast, using NCEP-ATP III cutoffs, only 410 participants (30%) were classified as having HTWP, with a marked disparity between men and women, with 316 out of 630 men (50%) 94 out of 724 (13%) women meeting criteria (P < .001). A total of 356 participants (26%) had fasting glucose levels ≥126 mg/dL while 304 participants (22%) had an HbA1c threshold ≥6.5%. Both criteria present in 220 (16%).
Table 2 presents the characteristics of study participants categorized by HTWP status in unadjusted analysis. Using Amerindian-specific criteria, participants with HTWP were younger, engage in higher levels of physical activity, were more frequently obese, and had higher non-HDL cholesterol and blood pressure compared to those without HTWP. Using the NCEP-ATP III criteria, most of these differences persisted across participants with and without HTWP, except that the former were more often women, and there were no differences in the prevalence of poor physical activity across groups.
Characteristics of 1354 Study Participants According to the Hypertriglyceridemic-waist Phenotype (HTWP) Using Two Distinct Constructs.

Statistically significant results.
Association Between HTWP and Type 2 Diabetes Mellitus
Using Amerindian-specific criteria, no significant association was found between HTWP and type 2 diabetes mellitus using HbA1c as the sole diagnostic criterion (22% vs 23%; P = .953). However, when fasting glucose levels were used for comparison, type 2 diabetes mellitus was significantly more prevalent among participants with HTWP compared to those without (29% vs 24%; P = .032). Similar results were observed when NCEP-ATP III criteria, with non-significant differences in the prevalence of normal or elevated HbA1c levels (25% vs 22%, P = .172), but a significant association when fasting glucose levels were used for diagnosis (32% vs 24%, P = .011).
Table 3 summarizes the results of all the unadjusted logistic regression models fitted to assess the associations between individual components, HTWP, and both biomarkers of type 2 diabetes mellitus, using Amerindian-specific and NCEP-ATP III criteria. Models showed significant direct associations between serum triglycerides and fasting glucose levels (OR: 1.36; 95% C.I.: 1.06-1.74), but not between serum triglycerides and HbA1c. Using Amerindian-specific cutoffs, increased waist circumference was not associated with fasting glucose nor with HbA1c levels. On the contrary, increased waist circumference was directly associated with fasting glucose (OR: 1.31; 95% C.I.: 1.03-1.67) but not with HbA1c, when NCEP-ATP III criteria were used.
Unadjusted Logistic Regression Models Showing the Associations Between Individual Components, The Hypertriglyceridemic Waist Phenotype (HTWP), and Both Biomarkers of Type 2 Diabetes Mellitus, Across Two Different Constructs of HTWP.

Abbreviations: HTWP, hypertriglyceridemic waist phenotype; NCEP-ATP III, National Cholesterol Education Program Adult Treatment Panel III.
Statistically significant results.
Also in unadjusted analysis, using the Amerindian-specific criteria, HTWP was associated with fasting glucose (OR: 1.30; 95% C.I.: 1.02-1.66). Same results were observed when NCEP ATP III criteria (OR: 1.53; 95% C.I.: 1.18-1.67) were used to compare the association between HTWP and fasting glucose. Associations between HTWP and HbA1c were non-significant in both cases.
When waist circumference was used as a continuous variable stratified in quintiles for presentation purposes, the association with fasting glucose was significant (OR: 1.14; 95% C.I.: 1.04-1.24) but not with HbA1c. Waist circumference had a normal distribution, and a significant association with fasting glucose after adjusting for sex (OR: 1.14; 95% C.I.: 1.05-1.24), which had a non-relevant effect in this association (Figure 1).

Predictive probabilities of elevated fasting glucose levels in men and women across waist circumference quintiles. The relationship shows an approximate linear trend, with quintiles 1 and 2 differing significantly from quintile 5.
Multivariate logistic regression models, adjusted for all the above-mentioned covariables, were fitted to evaluate the independent significance of the association between HTWP and fasting glucose. In a first model, using Amerindian-specific cutoffs for increased waist circumference, HTWP was significantly associated with higher fasting glucose levels (OR: 1.32; 95% C.I.: 1.02-1.71; P = .038). The second model, applying HTWP construct considering NCEP-ATP III criteria for increased waist circumference, also showed a significant association between HTWP and fasting glucose (OR: 1.50; 95% C.I.: 1.12-2.01; P = .006). None of the included covariables retained independent significance in either model. Interestingly, the strength of the association was greater when NCEP-ATP III criteria were used compared to Amerindian-specific cutoffs. There was no significant association between HTWP and HbA1c in multivariate models (data not shown).
When the two components of HTWP were separately included as exposures in the same multivariate model, only the association between hypertriglyceridemia and fasting glucose was significant in the model using Amerindian-specific cutoffs for waist circumference (Table 4). The same was observed in the model using NCEP-ATP III criteria, triglycerides were significantly associated with fasting glucose but waist circumference was not (Table 5).
Multivariate Logistic Regression Model Showing Associations Between the Two Components of the Triglyceridemic-waist Phenotype and Fasting Glucose Levels.

Increased waist circumference was based on Amerindian-specific cutoffs for men and women.
Statistically significant results.
Multivariate Logistic Regression Model Showing Associations Between the Two Components of the Triglyceridemic-waist Phenotype and Fasting Glucose Levels.
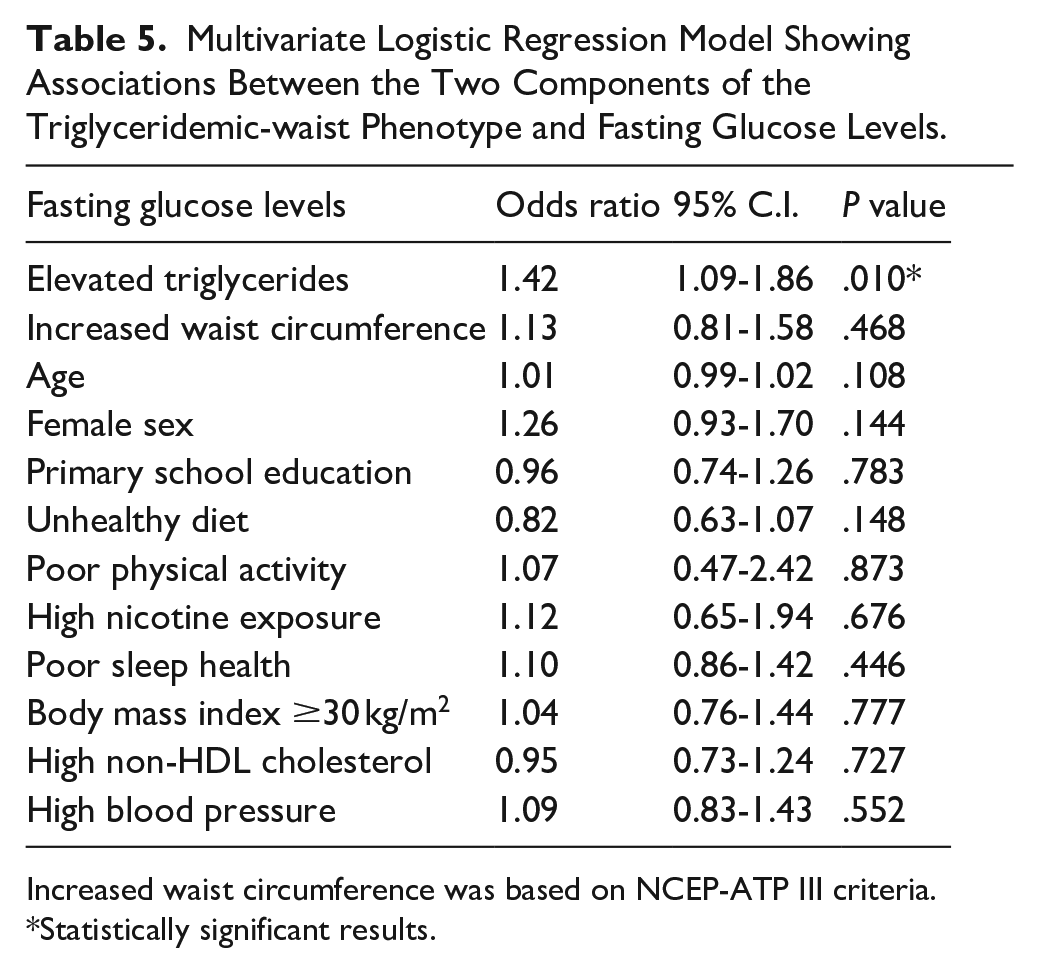
Increased waist circumference was based on NCEP-ATP III criteria.
Statistically significant results.
Regarding the associations between elevated triglycerides, increased waist circumference (using both Amerindian-specific cutoffs and NCEP-ATP III criteria), HTWP, and HbA1c, all multivariate models were non-significant in both men and women (data not shown).
Discussion
This study provides valuable insights into HTWP prevalence and association with type 2 diabetes mellitus among middle-aged and older adults of Amerindian ancestry living in rural villages of coastal Ecuador. In first place, it underscores the high prevalence of elevated serum triglyceride levels (55%), which exceeds that reported in most studies involving other races/ethnic groups. While hypertriglyceridemia prevalence varies widely across different studies and populations, it is generally accepted that African Americans and their ancestors have lower prevalence rates, whereas some Asian populations and American mestizos (an admixture of Indigenous Americans and Europeans) tend to exhibit higher rates of hypertriglyceridemia.17 -21
In population-based studies conducted among Canadian Inuit and other populations with predominant Amerindian ancestry, the prevalence of hypertriglyceridemia has been shown to be even higher than in other races/ethnic groups.6 -8 In this regard, Aymara natives from northern Chile have a prevalence of hypertriglyceridemia comparable to that reported in the present study. 22 It is noteworthy that indigenous Ecuadorians enrolled in our study and the Aymara (from Perú, Bolivia and Chile) represent the ethnic groups with the highest percentages of Amerindian ancestry in South America, based on population branch statistics analysis (94.1% and 96.8%, respectively).10,23
A second finding of interest in the present study is the high prevalence of increased waist circumference (79%), which exceeds that reported in many populations. 24 However, this extremely high prevalence was noted only when Amerindian-specific criteria were applied but decreased to 50% when NCEP-ATP III criteria were used. In any case, the significant rate of abdominal obesity does not align with the BMI status of participants, as only 31% had a BMI ≥30 kg/m2. The mismatch between central and visceral obesity is most likely related to the distinctive phenotypic characteristics of study participants. 25 These findings reinforces previous suggestions that BMI may not be the most suitable anthropometric measurement for assessing obesity in this and potentially in other races/ethnic groups. In this context, neck circumference has gained recognition as a strong marker of obesity in Amerindians and has been linked to adverse cardiovascular outcomes and increased mortality risk, even when accounting for other anthropometric measurements.26,27 Future studies should incorporate neck circumference as an essential metric in the construct of a phenotype that combines triglyceride levels and an anthropometric index.
As a consequence of the above-mentioned findings, it can be concluded that prevalence rates of hypertriglyceridemia, abdominal obesity, and HTWP are higher in people of predominantly Amerindian ancestry than in those from other races/ethnic groups. However, data comparison may be complicated because of the heterogeneity of study designs and the distinct criteria used to define components of HTWP. Even in the present study, there were important differences when Amerindian-specific and NCEP-ATP III criteria were used for diagnosis. The underlying causes of these differences have yet to be fully determined, but they likely result from a complex interplay of genetic, dietary, and environmental factors, which together account for a sizable proportion of these effects. 28
Another key observation of the present study is the differential association between HTWP and biomarkers of type 2 diabetes mellitus. While no significant differences were observed when assessing diabetes prevalence via elevated HbA1c levels, fasting serum glucose levels demonstrated a significant association. This suggests that relying solely on HbA1c for diagnosing diabetes in Amerindian populations may not fully capture the metabolic dysregulations associated with HTWP. This discrepancy warrants further investigation to determine which factors contribute to variations in glycemic markers. In this regard, it is possible that fasting glucose might be a more sensitive biomarker of metabolic disturbances related to HTWP than HbA1c, as some phenotypes may exhibit stronger associations with short-term glycemic markers rather than long-term markers. 29 HTPW is linked to insulin resistance, which can lead to episodic fasting hyperglycemia without necessarily causing increased HbA1c levels. Since HbA1c falls to capture transient glucose abnormalities, it may underestimate the risk of type 2 diabetes mellitus in individuals with HTWP.30,31
All these considerations may have important clinical implications for early diabetes screening in individuals with HTWP. Given our findings, waist circumference alone may not be the most relevant indicator of the association between HTWP and type 2 diabetes mellitus. If a single criterion is to be selected, the standard NCEP-ATP III cutoffs for waist circumference could be preferable for indigenous people living in the Americas. Otherwise, the association would primarily depend on hypertriglyceridemia. Despite its significance, the link between isolated hypertriglyceridemia and cardiovascular health outcomes has been largely overlooked. However, a growing evidence body of evidence highlights its adverse consequences.32,33 In populations with inconsistent waist circumference cutoffs, isolated triglyceride determinations could serve as a stand-alone marker of cardiovascular and metabolic risk. Alternatively, hypertriglyceridemia may be used together with other emerging biomarkers of cardiovascular risk to enhance its predictive ability. Potential candidates could include apolipoproteins, 34 or other traditional inflammatory biomarkers such as C-reactive protein, cortisol, and interleukins 1 and 6. 35
While previous research has highlighted the association between HTWP and metabolic risk across diverse racial and ethnic groups, this study addresses a critical gap by specifically examining an indigenous Ecuadorian population. The high prevalence of HTWP among study participants reinforces the importance of understanding ethnicity-related variations in metabolic risk factors. In the present study, participants with HTWP are more likely to exhibit other cardiovascular risk factors, such as obesity, high non-HDL cholesterol levels, and elevated blood pressure. These findings highlight the multifaceted nature of metabolic health in this population, emphasizing the necessity of a comprehensive approach to risk assessment beyond triglyceride levels and waist circumference alone. Given the lifestyle characteristics of this community—including low rates of sedentarism, a diet rich in oily fish and carbohydrates, but limited access to healthcare—the interaction between these factors and metabolic risk requires further exploration.
Strengths of this study include the population-based design with unbiased participant enrollment, the systematic assessment of the investigated variables using validated structured field instruments and the use of reliable laboratory equipment ensuring accurate measurements. In addition, the study benefits from the application of 2 distinct constructs to estimate HTWP prevalence, providing a more complete evaluation of metabolic risk.
This study has limitations that go beyond its cross-sectional design. The findings, though highly relevant to Amerindian populations, may not be entirely generalizable to other ethnic groups due to genetic and environmental differences. Additionally, waist circumference cutoffs remain a debated issue, and the lack of full standardization could affect the clinical applicability of the results. While fasting glucose was identified as a potentially more sensitive biomarker of metabolic disturbances than HbA1c, relying primarily on one measure may overlook aspects of long-term metabolic regulation. In addition, the 2-h post-prandial glucose testing (not used in this study) may have provided potentially useful information in participants with glucose intolerance. Furthermore, the study does not consider some potential confounding factors which might have influenced the reported associations.
Overall, this study underscores the need for tailored prevention strategies for indigenous populations in Ecuador and across Latin-American countries where over 40 million indigenous people reside. 36 Given that hypertriglyceridemia is a primary driver of diabetes risk, educational support programs should prioritize reducing refined carbohydrate intake and promoting aerobic physical activity. Addressing metabolic health disparities requires a comprehensive approach that incorporates ethnic-specific cutoff values, socio-environmental influences, and barriers to healthcare access. Future longitudinal studies should explore the progression of HTWP in Amerindian communities and identify targeted interventions to mitigate cardiovascular risk.
In conclusion, our findings contribute to a growing body of literature that recognizes the diversity in metabolic responses across ethnic groups and underscore the importance of population-specific studies. In addition, this study contributes to better stratification methods by incorporating novel metabolic markers and subgroup analyses. By addressing risk stratification strategies, these insights could inform targeted health policies aimed at improving metabolic outcomes in underserved communities.
Supplemental Material
sj-pdf-1-jpc-10.1177_21501319251362044 – Supplemental material for Prevalence of hypertriglyceridemic-waist phenotype and its association with type 2 diabetes mellitus among middle-aged and older adults of Amerindian ancestry
Supplemental material, sj-pdf-1-jpc-10.1177_21501319251362044 for Prevalence of hypertriglyceridemic-waist phenotype and its association with type 2 diabetes mellitus among middle-aged and older adults of Amerindian ancestry by Denisse A. Rumbea, Robertino M. Mera, Emilio E. Arias, Kleber Arriaga and Oscar H. Del Brutto in Journal of Primary Care & Community Health
Footnotes
Author Contributions
DAR: study design; data collection and analysis; RMM: statistical analysis, significant intellectual contribution to manuscript content; EEA: data collection; KA: interpretation of laboratory exams;. OHD: study design, manuscript drafting.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Universidad Espíritu Santo – Ecuador. The sponsor had no role in the design of the study, in the collection, analysis and interpretation of data, or in the decision to submit the manuscript for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.