
Abstract
Introduction/Objectives:
Vaccination rates in the United States have seen a concerning decline in recent years. Primary care, as the front line of healthcare for most individuals, is critical in reversing this trend. This study investigates trends in vaccine delivery amongst healthcare providers before and after Coronavirus Disease 2019 (COVID-19).
Methods:
The delivery of vaccinations were enumerated by provider type using a combination of 2017 to 2021 Medicare Part B Fee-For-Service claims and the 2013 to 2021 Medical Expenditure Panel Survey (MEPS).
Results:
Our findings reveal a notable decline in primary care physician (PCP)-administered vaccinations, with mass immunizers and non-physician providers increasingly assuming this role. Medicare claims showed that the vaccine delivery by PCPs decreased over time, from 46.2% in 2017 to 32.3% in 2021, while the vaccine delivery by mass immunizers increased over time, from 45.2% in 2017 to 60.5% in 2021. Similarly, MEPS data showed that PCPs accounted for 53.6% of vaccination visits in the pre-pandemic period but only 22.9% during the pandemic.
Conclusions:
The COVID-19 pandemic profoundly disrupted vaccine delivery, reshaping the roles of PCPs and other providers. This study highlights the need to better integrate primary care into future vaccine distribution frameworks to ensure broad and equitable access in the post-pandemic era.
Introduction
Vaccination has been an important public health strategy to prevent serious infectious diseases and save human lives from vaccine-preventable diseases. Historically, primary care has been crucial for reliable, equitable vaccine delivery, as continuous trusting relationships with a patient’s own doctor or health care provider mitigates vaccine hesitancy and distrust in healthcare.1,2 Recent studies have shown that the number of primary care physicians (PCPs) per capita was associated with higher Coronavirus Disease 2019 (COVID-19) vaccination rates in the US and having a usual source of primary care contributed to lower COVID-19 vaccine hesitancy.3,4 Indeed, primary care is in a unique position to promote vaccine equity especially in resource-limited and vaccine hesitant communities disproportionately at risk for COVID-19 and other illness.
Prior to the COVID-19 pandemic, the majority of visits for vaccination among the US population were with PCPs. 5 Wilkinson et al 5 showed that most Medicare Part B Fee-For-Service (FFS) beneficiaries in 2017 received vaccinations from PCPs (46.2%) or mass immunizers (45.2%), followed by nurse practitioners/physician assistants/certified clinical nurse specialists (NPs/PAs/CCNSs; 4.6%). Their analysis of the general population using the Medical Expenditure Panel Survey (MEPS) again demonstrated that PCPs provided most clinical visits for vaccination (53.6% of all visits) between 2013 and 2017. 5
However, the rise of retail pharmacies and declining access to primary care threatened equitable vaccine delivery.6,7 The COVID-19 pandemic further disrupted healthcare delivery. In the early phases of COVID-19 vaccination – when speed, scale, safety, and security were the most urgent public priorities – vaccine administration was provided by public health departments, hospitals, mass vaccination sites, and pharmacies, reducing PCPs from early vaccination distribution efforts. Additionally, anti-vaccination messages were broadly amplified through social media and quickly shared online, exacerbating medical mistrust. Pharmacies and mass vaccination sites were prioritized and predominately used by the public, potentially leading to heightened mistrust especially from vulnerable communities.8,9 Additional politicization of the vaccine amplified hesitancy in vaccination among patients, especially in vulnerable communities with historic mistrust in healthcare. 10 Simultaneously, social distancing guidelines and patient’s hesitancy to visit clinical settings during lockdown required practices to shift to telemedicine, reducing their abilities to vaccinate. 11 An analysis of commercial claims and electronic health records (EHRs) data has shown that there were substantial reductions in well-child visits in 2020 and 2021 (−47.3%, the largest decrease in April 2020) as a result of COVID-19 compared with the same time period in the previous 2 years, thereby increasing rates of missed pediatric and adolescent vaccinations. 12
Post-pandemic vaccination efforts were slow despite ample vaccine availability. A 2023 analysis found up to 49% of Americans reported some level of hesitancy about immunization, highlighting the absence of trusted medical professionals for vaccination advice. 13 Physicians and nurses were the most trusted sources of health information during the pandemic, emphasizing the need for primary care in vaccine rollout. 14
This study builds on the Wilkinson et al 5 2021 publication by extending analysis to include COVID-19’s disruption of vaccine delivery and provides meaningful insights for post-pandemic vaccination strategies. Using publicly available Medicare claims and MEPS datasets, we analyzed vaccine distribution patterns amongst healthcare providers before and after COVID-19 to highlight the need to better integrate primary care in enhancing vaccine access and fostering trust in the post-pandemic era.
Methods
To investigate trends in vaccine delivery before and after COVID-19, this study enumerated the delivery of vaccinations by provider type using a combination of the 2 publicly available datasets. This is a descriptive observational study to provide the key features of vaccine delivery.
Data Sources
This study analyzed the 2 datasets. First, the 2017 to 2021 Medicare Provider Utilization and Payment Data: Physician and Other Practitioners Public Use File (hereafter referred to as Medicare Part B FFS) provides information on services and procedures provided to Medicare Part B FFS beneficiaries at the provider level. The data are available annually from the Centers for Medicare and Medicaid Services at https://data.cms.gov/provider-summary-by-type-of-service/medicare-physician-other-practitioners/medicare-physician-other-practitioners-by-provider-and-service/data. Second, MEPS is a set of population-level longitudinal surveys of nonmilitary and noninstitutionalized individuals and families across the United States. These data are collected through respondents’ reports for themselves and their family members. The data are enriched with follow-up verification with physician offices for diagnoses and events. MEPS provides nationally representative estimates of healthcare services and expenditures for all age groups. We merged medical conditions, office-based, outpatient, and consolidated files to enumerate services delivered in office-based and outpatient visits from 2013 to 2021. The Agency for Healthcare Research and Quality maintains an archive of these files at https://meps.ahrq.gov/mepsweb/data_stats/download_data_files.jsp.
Measures
Identification of Vaccination and Provider Using Medicare Part B FFS
We calculated vaccination services by 5 different types of healthcare providers: (1) PCPs, (2) NPs/PAs/CCNSs, (3) mass immunizers, (4) clinical laboratory, and (5) other. We categorized PCPs using the standard method that includes family practice, general practice, geriatric medicine, or internal medicine. The Medicare Part B FFS includes non-physician provider types of NPs/PA/CCNS but does not provide their specialty. Mass immunizers include drugstore and grocery chains as well as community pharmacies and were identified using the provider terms of centralized flu, mass immunizer roster biller, pharmacy, or public health or welfare agency. Clinical laboratory was identified using the provider term of clinical laboratory delivering medically necessary laboratory services and some screening tests ordered by a physician or a qualified non-physician provider. The one remaining or not included was categorized as other. We used Healthcare Common Procedure Coding System codes descriptions to identify vaccination services in Medicare Part B FFS (Supplemental Table A1). To be included as a vaccination service, the description must have contained “vaccine” or “vaccination” and not have contained “detection.” Since a COVID-19 vaccination has been given since December 2020, new codes for the COVID-19 vaccination were added in the 2021 data.
Identification of Vaccination and Provider Using MEPS
We categorized MEPS providers into 4 groups: (1) PCPs, (2) non-PCPs, (3) nurses/NPs/PAs, and (4) other nonphysicians. We included physicians with specialties of family medicine, internal medicine, pediatrics, and geriatrics in the PCP category. Examples of other nonphysicians included dentists, psychologists, social workers, and technicians. We used questions related to reasons for visit from the office-based and outpatient files to identify visits for vaccination along with the ICD-9/ICD-10 codes for an immunization encounter (Supplemental Table A2). Instead of year-by-year comparison, we calculated the number and proportion of visits for vaccinations seen by provider type using survey weights averaged over the 5 years pooled from 2013 to 2017 (pre-pandemic) and the 2 years pooled from 2020 to 2021 (mid-pandemic), which result in a nationally representative sample for 1 year in each period.
Statistical Analysis
We first replicated the results in the pre-pandemic period from the Wilkinson et al. earlier study and updated vaccine distribution amongst common providers up to 2021. Then we created summary statistics and compared trends in vaccination delivery by provider type before and after the pandemic. The primary goal is simply presenting the data itself rather than drawing conclusions about relationships. This study doesn’t involve any statistical inference. All analyses were performed using Stata version 17 (StataCorp LLC, College Station, TX). This study was ruled exempt by the American Academy of Family Physicians Institutional Review Board.
Results
Vaccination Using Medicare Part B FFS
The number and proportion of vaccination services in Medicare Part B FFS were calculated from 2017 to 2021 (Supplemental Table A3). In 2017, there were 34.3 million vaccination services (1.4% of 2.4 billion total services). Overall PCPs provided the most vaccinations (46.2%), followed by mass immunizers (45.2%), then NPs/PAs/CCNSs (4.6%). In 2021, there were 28.0 million vaccination services (1.1% of 2.5 billion total services). Mass immunizers provided the most vaccinations (60.5%), followed by PCPs (32.3%), then NPs/PAs/CCNSs (4.6%). As shown in Figure 1, the vaccine delivery by PCPs decreased over time, from 46.2% in 2017 to 32.3% in 2021, while the vaccine delivery by mass immunizers increased over time, from 45.2% in 2017 to 60.5% in 2021.

Vaccination services by provider type in Medicare part B fee-for-service, 2017 to 2021.
Vaccination Using MEPS
Figure 2 shows the results using MEPS (see the number and proportion of vaccination visits by provider type in Supplemental Table A4). In the pre-pandemic period (2013-2017), there were an average 69.7 million vaccination visits in outpatient or office-based settings per year, and the majority of visits for vaccination were with PCPs (53.6%). During the 2 year of COVID-19 pandemic (2020-2021), there were an average 176.0 million vaccination visits per year, but the majority of visits for vaccination were with other nonphysicians (36.8%) or nurses/NPs/PAs (34.9%).
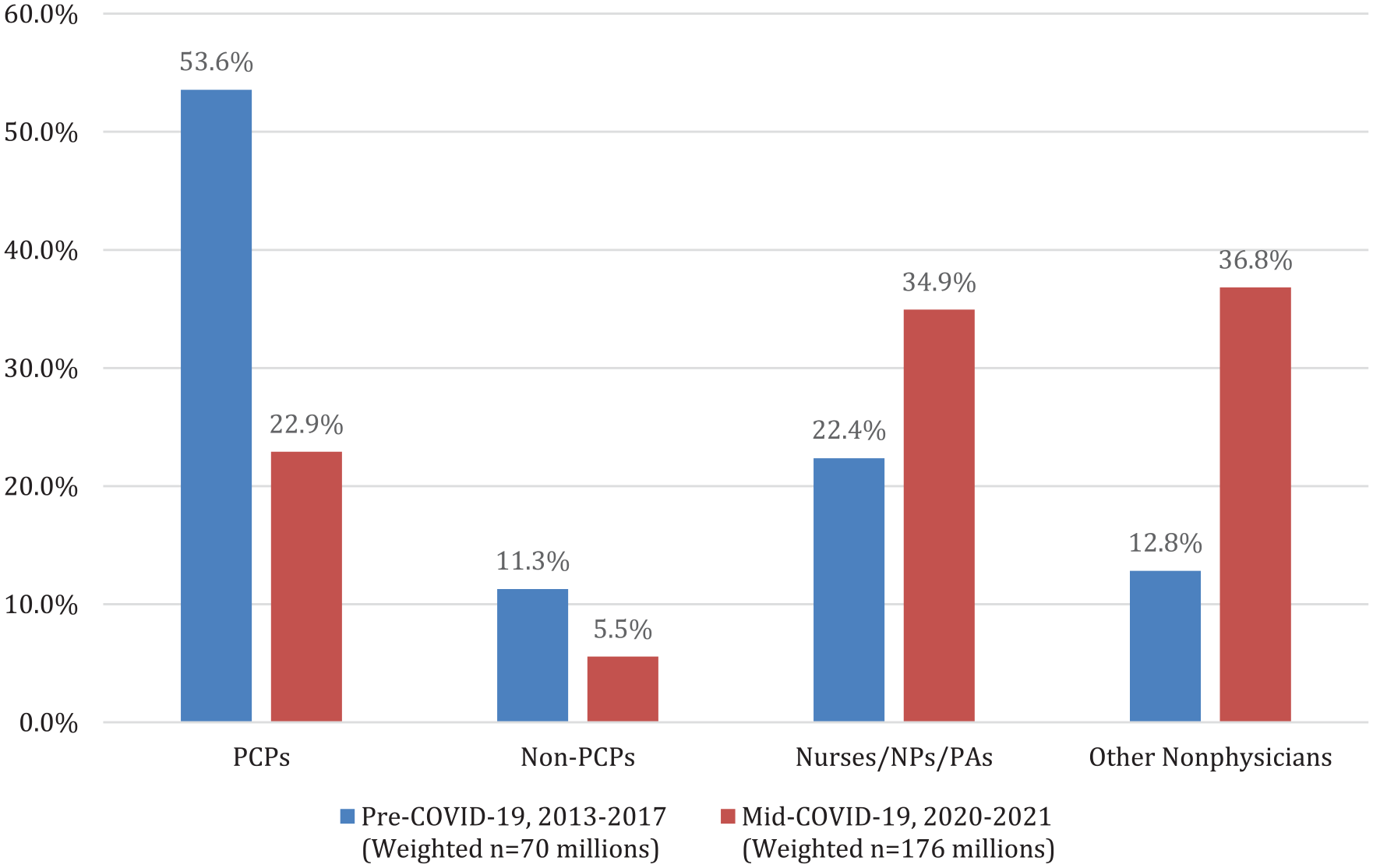
Vaccination visits by provider type in medical expenditure panel survey, 2013 to 2017 versus 2020 to 2021.
Discussion
The COVID-19 pandemic profoundly disrupted vaccine delivery, reshaping the roles of PCPs and other providers. Our findings reveal a notable decline in PCP-administered vaccinations, with mass immunizers and non-physician providers increasingly assuming this role.
The potential reasons for this shift in vaccine delivery dynamics are multifactorial. Mass immunizers were pivotal during the pandemic, ensuring rapid vaccine rollout at scale, particularly in the early days of the pandemic. This combined with the fact that traditional care in the continuity setting was disrupted with stay-at-home orders may have created an environment where, post pandemic, patients were accustomed to getting vaccines in their local pharmacy. Furthermore, regulatory changes during the pandemic expanded pharmacists’ scope of practice to administer a wider range of vaccines likely resulting in some of the growth in mass immunizers that we observed in the data. 15
While the convenience and habit of receiving vaccines from a local pharmacy has certainly changed patient behaviors, the implications of this shift are less clear. For multi-dose and childhood vaccines, in particular, it is essential to track delivery in a centralized system to ensure that a patient is fully vaccinated. 16 Although vaccine registries can serve as a centralized system, many are currently limited in their utility given incomplete data. Moreover, limited bidirectional interoperability between immunization registries and EHRs burdens PCPs with inefficient documentation processes, increasing administrative costs and time requirements. 17 Furthermore, the decline in vaccine administration within primary care settings may indicate a broader reduction in preventive care visits overall. 18 While pharmacies effectively expand access to vaccinations, visits to a primary care office often serve a dual purpose, offering opportunities to deliver other essential preventive services as well as to identify and manage chronic conditions. As such, shifting vaccination away from primary care may inadvertently reduce these valuable touchpoints for comprehensive care.
There are several limitations worth acknowledging. First, the analysis relies on administrative and survey data, which may not capture all vaccination events, both within and outside of traditional healthcare settings. Second, the categorization and definition of providers in both datasets risks a degree of classification bias, whether through misclassification or due to some providers performing multiple roles. Third, the focus on a limited set of years in the post-pandemic period (2020-2021) may not fully reflect long-term trends in vaccination delivery after the pandemic.
With vaccine hesitancy growing amidst the pandemic19,20 and a decline in the uptake of certain vaccines on the rise, fully understanding the implications of shifting vaccine delivery sites is essentials. While mass immunizers have expanded access, they may not offer the continuity of care or trusted relationships that help address hesitancy and misinformation. PCPs remain the most trusted healthcare providers, 14 a critical advantage in engaging hesitant patients and promoting vaccine confidence. Our findings highlight the need for ongoing analysis to inform policies that leverage primary care’s strengths while maintaining partnerships with mass immunizers and non-physician providers. These efforts are critical for rebuilding a robust, patient-centered vaccination system in the post-pandemic era.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251356376 – Supplemental material for Shifting Patterns of Vaccine DeliveryBefore and After COVID-19: The Declining Role of Primary Care
Supplemental material, sj-docx-1-jpc-10.1177_21501319251356376 for Shifting Patterns of Vaccine DeliveryBefore and After COVID-19: The Declining Role of Primary Care by Jeongyoung Park, Annie Didden, Andrew W. Bazemore, Yalda Jabbarpour and LaTasha Seliby-Perkins in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
None.
Ethical Considerations
This study was ruled exempt by the American Academy of Family Physicians Institutional Review Board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was developed independently by the ABFM Foundation, Inc. with partial funding provided from Sanofi. Sanofi was not involved in developing this manuscript and did not review it prior to publication. The opinions and view expressed are solely those of the authors and do not reflect Sanofi’s position.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Raw data underlying this article were generated from multiple publicly available datasets. Access to the analytic data will be made available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.