
Abstract
Introduction and Objective:
Food insecurity (FI) is associated with adverse health outcomes across the lifespan. Primary care and prenatal practices can identify and address FI among patients through screening and interventions. It is unclear how practices and communities responded to FI during the COVID-19 pandemic, and how the pandemic may have impacted practices’ FI strategies. We aimed to understand how practices providing primary care or prenatal care in northern New England experienced changes in FI during the COVID-19 pandemic.
Methods:
We conducted a web-based survey of clinicians and staff from 43 unique practices providing primary care or prenatal care in northern New England.
Results:
Most practices (59.5%) reported at least 1 new food program in the practice or community since the pandemic began. Practices reporting new practice- or community-based food programs were more likely to be rural, federally qualified health centers, and have greater confidence in practice and community capacity to address FI (chi-square tests, P < .05).
Conclusion:
Results suggest that practices and surrounding communities in northern New England responded to FI during the pandemic by increasing food support programs. Future work is needed to examine the impact of food programs initiated during the pandemic and determine optimal strategies for practices to address FI among patients.
Introduction
Food insecurity (FI) is a critical public health issue in the U.S., affecting 1 in 10 households in 2019. 1 The U.S. Department of Agriculture (USDA) defines food security as “access by all people at all times to enough food for an active, healthy life.”1,2 Certain populations experience disproportionately high rates of FI, including rural and urban communities, households with incomes below the federal poverty level, households with children under age 18, unmarried women, and Black and Hispanic-headed households. 1 FI is associated with adverse health outcomes including chronic disease in adults, 3 negative behavioral and academic outcomes in children, 4 and gestational weight gain and diabetes in pregnant women. 5 Thus, addressing FI is crucial to decrease health inequities and improve the health of individuals and communities.
Beginning in early 2020, the coronavirus disease 2019 (COVID-19) pandemic caused widespread social and economic disruption, including increased poverty rates. 6 Early studies suggested that rates of household FI also increased during the pandemic. 7 Northern New England, comprised of the largely rural states of Maine, New Hampshire, and Vermont, experienced this early rise in FI; one survey in Vermont in March and April of 2020 demonstrated a 32% increase in FI. 8 However, the USDA ultimately found that 10.5% of U.S. households were food insecure during 2020, which was unchanged from the rate in 2019. 9 A variety of supports may have prevented an increase in overall FI rates despite social and economic challenges brought on by the pandemic. Additional funding was used to expand federal nutrition assistance programs 10 and use of programs such as the Supplemental Nutrition Assistance Program (SNAP), the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), and food pantries increased in early 2020. 11 Additional food initiatives implemented by health care organizations and communities also may have buffered changes in FI during the pandemic.
Health care organizations can address FI by conducting routine screening among patients, hosting practice-based food programs, and referring patients to community-based or public food assistance programs. 12 Practices providing primary care and prenatal care may be particularly well suited to identify and address FI given their longitudinal relationships with patients. Interventions at primary care practices can increase food resource referrals, food pantry use, and fruit and vegetable consumption.12,13 During the pandemic, some primary care practices addressed FI by initiating telephone calls to patients about their social needs14,15 and recommending safe options for accessing food such as food delivery. 15 Assessing the role and experience of primary care and prenatal practices in addressing FI during the pandemic can add to our understanding of how to engage health care providers and practices in reducing FI, particularly in rural areas such as northern New England. In this study, we surveyed staff and clinicians from practices providing primary care or prenatal care in northern New England to understand how they addressed FI during the COVID-19 pandemic.
Methods
Between September 2020 and March 2021, we conducted a 1-time web-based survey of a convenience sample of clinicians and staff from primary care and prenatal care practices as part of a larger mixed-methods study on how these practices addressed FI. The study setting included practices in the 3 northern New England states of Vermont, Maine, and New Hampshire, which have large rural populations estimated at 65%, 40%, and 37%, respectively. 16
Participants were recruited via emails to members of 4 regional practice networks: The Dartmouth CO-OP Northern New England Practice-based Research Network, the Northern New England Perinatal Quality Improvement Network, the Bi-State Primary Care Association, and the Northern New England Clinical and Translational Research Network. Many of the practices in these networks are located in rural communities or serve catchment areas that include rural communities in the 3 states. We collected responses at the practice level; duplicate responses from a single practice were excluded so that there was a single survey response included per practice. Practices were categorized as rural (Rural-Urban Commuting Area Code [RUCA] ≥ 4) or urban (RUCA 1-3) based on practice zip code. 17
The survey was developed by research team members with expertise in primary care, prenatal care, and rural health, as well as research in public health, food security, and nutrition. We also sought feedback on the survey questions from a care manager and a community health worker who have expertise in addressing food insecurity in the study setting. Survey topics included respondent and practice characteristics, processes for FI screening and interventions, and perceived change in FI among patients during the pandemic. Topics also included confidence in practice and community ability to address FI and perspectives on food programs in the practice and surrounding community.
Survey questions included in this analysis are presented in Supplement 1. These questions are part of a larger survey of how primary care and prenatal care practices address FI. The current analyses in this article are focused on practice experience during the COVID-19 pandemic with an emphasis on new program implementation. Practice screening processes were considered “systematic” if a formal screening tool was used and “informal” if FI was discussed but no tool was used. Respondents were asked to estimate change in FI qualitatively among their patients as “no change,” “decrease,” “small increase,” or “large increase”; this was then dichotomized to “small increase or no change” versus “large increase” for analysis (no respondents reported a decrease in FI). Confidence in community and practice ability to address FI was assessed on a 5-point Likert scale (scored 0-4) from “not confident at all” to “very confident.” Confidence pre-pandemic and during the pandemic were composite variables created by adding community and practice confidence scores and dichotomizing to low confidence (0-5) versus high confidence (6-8). Respondents were asked if they were aware of new food programs in their practices and communities that were started during the pandemic, and if so were asked to specify the type. To assess the burden experienced by practices, respondents were also asked about their perceived change in FI among patients and confidence in addressing FI.
Here we present data on changes resulting from the COVID-19 pandemic, with a focus on new food programs implemented by the practices and their surrounding communities. All variables collected were categorical and dichotomized for analysis. Data were summarized descriptively using absolute and relative frequencies. We used chi-square tests of independence to evaluate relationships between practice characteristics and both new food programs and perceived change in FI. McNemar’s test was used to evaluate for changes in the proportion of respondents reporting high confidence in addressing FI before and during the pandemic. “Don’t know or prefer not to answer” responses were considered missing data and these responses were excluded from analyses. This study was determined exempt by the Dartmouth Health Institutional Review Board.
Results
We surveyed 1 clinic staff member from each of 43 unique practices. Table 1 presents characteristics of practices and respondents. Respondents were mostly clinicians or resource specialists/community health workers from hospital-affiliated practices or federally qualified health centers (FQHCs). Practices generally provided pediatric, family medicine, obstetrics/gynecology, internal medicine, and multispecialty care and the majority had >10 providers. Almost 70% of practices were categorized as rural (RUCA ≥ 4). Approximately one-half of the practices conducted systematic screening for FI.
Characteristics of Practices and Respondents (n = 43).

Abbreviations: CHW, community health worker; FI, food insecurity; FQHC, federally qualified health center.
Physician, nurse practitioner, or physician assistant.
RN, LPN.
More than 1 selection allowed. If more than 1 specialty was selected, the practice was considered multispecialty.
Rural defined as Rural-Urban Commuting Area Code ≥4. 17
Forty-two respondents completed a question regarding new community or practice-based programs during the pandemic. Approximately 1 quarter (26.2%) of these respondents reported at least 1 new program in the practice and 59.5% reported new programs in the community. All respondents who reported new practice-based programs also reported new community programs. Types of new or expanded programs within practices and communities are displayed in Figure 1. Among respondents who reported new programs in either setting (n = 25), the most common programs reported were school lunch programs (96.0%) and food drives or food shelves (64.0%). Of the participants who responded to a question regarding program closure (n = 39), 20.5% reported closure or reduction of a community-based program during the pandemic, and only 1 respondent (2.6%) reported closure or reduction of a practice-based program.
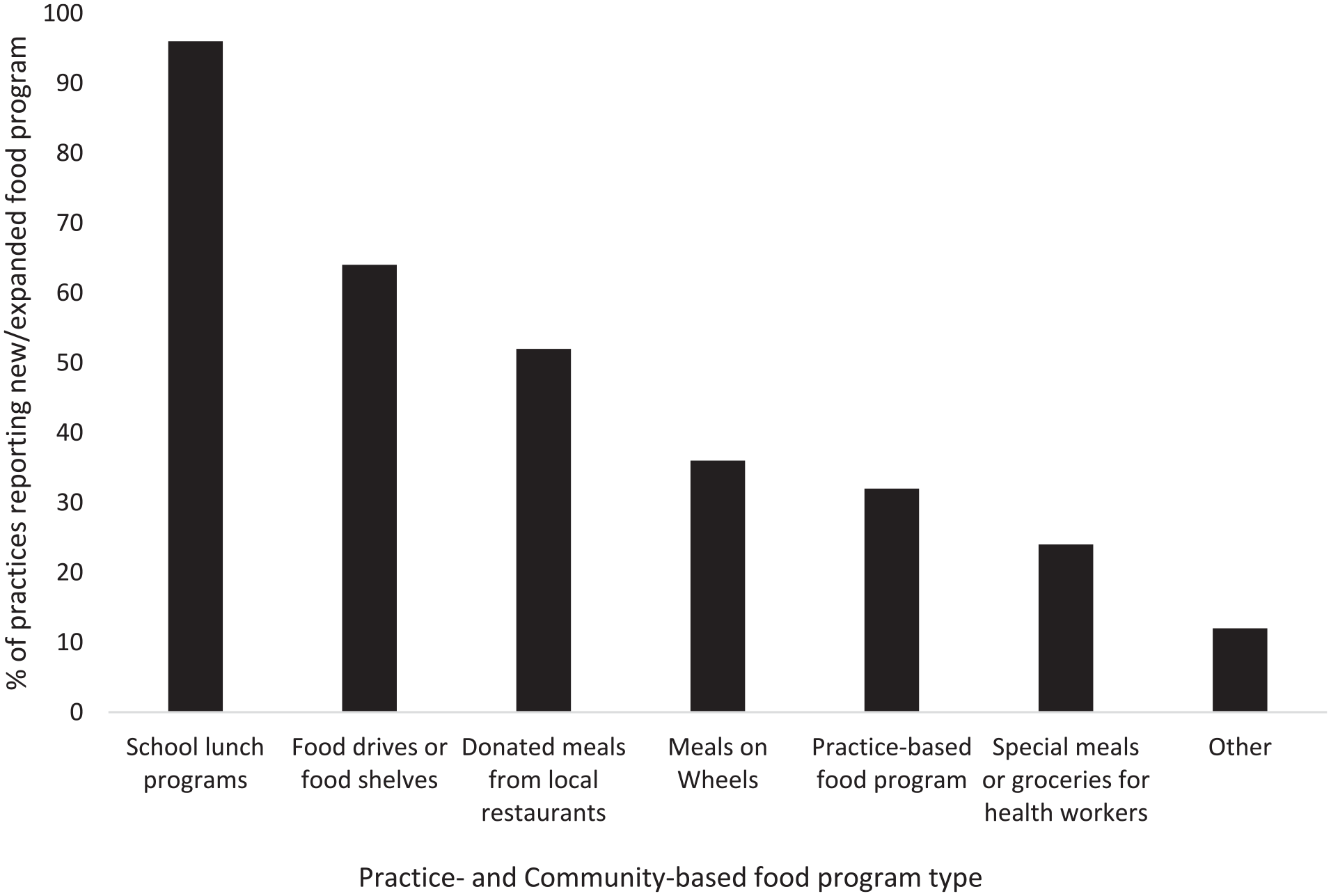
Distribution of types of new practice- and community-based food programs started or expanded during the COVID-19 pandemic as reported by practices that were aware of new programs (n = 25).
Associations between awareness of new food programs in the practice or community and practice characteristics are displayed in Table 2. FQHCs were significantly more likely to report new practice or community programs than non-FQHCs (P = .02) and rural practices were more likely to report new programs than urban practices (P = .03). Report of new programs was also associated with higher confidence in addressing FI both before the pandemic (P < .01) and during the pandemic (P < .01). There were no significant associations between knowledge of new practice or community food programs and practice size, FI screening process (systematic versus informal or no screening), or perceived change in FI during the pandemic (P > .05). Respondents were more likely to report high confidence in practice and community capacity to address FI before the pandemic (69.1%) than during the pandemic (54.8%) (P = .03, McNemar’s test).
Association of Practice Characteristics with New Food Programs in the Practice or Community During the COVID-19 Pandemic (n = 42).

Abbreviations: FI, food insecurity; FQHC, federally qualified health center.
All P-values are for chi-square tests of independence.
Confidence pre-pandemic and during the pandemic are composite variables determined by adding responses from two 5-point Likert scales (scored 0-4) for confidence in ability of practice to address FI and ability of community’s resources to address FI (total score 0-8); variable was dichotomized to high confidence (6-8) and low confidence (0-5) for analysis.
When asked about perceived change in FI among patients since the onset of the pandemic (n = 36), 47.2% of respondents estimated a large increase in FI, 47.2% estimated a small increase, and 5.6% reported no change. No respondents perceived a decrease in FI. There were no statistically significant associations between perceived change in FI and practice characteristics including rurality, FQHC status, practice size, and FI screening process (P > .05).
Discussion
The majority of respondents from primary care and prenatal care practices in this study reported new practice- or community-based food programs during the pandemic, suggesting a multi-faceted community response to FI. Practices reporting new practice- or community-based food programs were more likely to be rural and FQHCs. A qualitative study of community members in another rural region, Appalachia, similarly reported an increase in community food resources during the pandemic. 18 There is evidence that there is a greater number of Feeding America food provision services per person in rural U.S. counties than urban counties, 19 so it is possible that rural communities were more prepared to start or expand food programs. However, there is no literature to our knowledge on the initiation of food programs in rural versus non-rural communities during the pandemic. FQHCs may have been more likely to report new food programs as they typically serve vulnerable patient populations with high rates of FI, 20 are often well-connected to the community, and tend to screen for social determinants of health such as FI. 21 The sustainability of new programs started during the pandemic is unknown, and future work is needed to understand the resources practices and communities require to maintain programs post-pandemic.
Respondents reporting new food programs during the pandemic were also more likely to have greater confidence in practice and community capacity to address food insecurity. Practice confidence in addressing FI and awareness of changes in community food programs during the pandemic may reflect collaboration and connections between practices and community organizations. Studies have shown that interventions involving referrals from practices to community food resources can increase use of food resources among patients. 12 In our team’s qualitative work on FI in prenatal care settings, 22 clinics primarily addressed FI through internal referrals to clinic-based staff, such as a dedicated resource specialist, who could then refer to community resources. Practice staff discussed the importance of strong relationships between the clinic and the community organizations, and felt that better coordination between clinics and various community resources was needed to address FI. 22 Health care organizations that screen for FI and connect patients to food resources partner with a variety of community organizations, most commonly food banks. 23 This supports our findings, which suggest that collaboration between practices and community food programs is important for addressing FI. Further work is needed to determine barriers and facilitators to these connections, and whether such connections have an impact on FI among patients in primary care and prenatal settings.
Overall, respondents were more likely to report high confidence in the capacity of the practice and community to address FI before the pandemic than during the pandemic. Lower confidence during the pandemic may be due to higher observed rates of FI observed by some practices. Additional contributing factors could include increased strain on practices due to the need for rapid adoption of telemedicine,24,25 financial strain on practices, 26 and burnout experienced by staff members. 24 Additionally, the transition to more care being delivered by telemedicine during the pandemic 25 could have impacted rates of FI screening and ability to refer patients to resources. We used confidence only as an estimate of how effectively respondents felt their practices and communities addressed FI; further studies are needed to evaluate how new FI programs implemented during the pandemic impacted FI rates.
Our finding that nearly half of respondents (47.2%, n = 17) estimated a large increase in FI among their clinic patients since the start of the COVID-19 pandemic is consistent with early data indicating increased FI rates during the pandemic.7,8 The remaining practices perceived a small increase or no change in FI rates, consistent with the overall USDA finding of stable FI rates nationally from 2019 to 2020.1,9 The differences in perceived change in FI could be due to variation in FI prevalence during the pandemic. Monthly poverty rates fluctuated during the pandemic, 6 which likely impacted FI rates. Variability in food resources throughout different communities may have also impacted FI rates. The dichotomy of responses may also reflect variation in FI screening mechanisms at practices that could lead some FI to go undetected. For example, in our sample only about half of practices screened for FI systematically, while the other half screened informally or did not routinely screen at all. Strain on practices, as discussed above, could have impacted the ability of practices to identify food insecurity in patients.
Limitations
Potential limitations of our study include regional recruitment within 3 largely rural northern New England states, which could decrease the generalizability of results to other regions. Our sample size was small, potentially due to strain on practices during the pandemic. Our recruitment methods utilized Listservs as well as direct emails to practice network participants, precluding accurate calculation of response rate. We collected responses at the practice level (ie, 1 response per practice) and variability in respondent roles, experience, and knowledge of practice and community FI initiatives may have impacted our findings. Therefore, our findings may not reflect actual changes in FI rates or community resources. As survey responses were collected between the fall of 2020 and spring of 2021, variability in local COVID-19 infection rates and availability of food programs during the study period may have also affected our data. We assessed the presence of new practice or community programs that started during the pandemic but did not measure the actual or perceived effectiveness of the programs, including the patient perspective. Finally, we did not assess the impact of new food programs on FI in specific patient populations as we were collecting data at the practice level.
Conclusion
Our study reveals ways in which practices providing primary care or prenatal care in northern New England were impacted by and responded to FI during the COVID-19 pandemic. Over half of survey respondents reported increased food support programs in the practice and/or community in response to FI during the pandemic. Practices reporting new practice or community-based food programs were more likely to be rural and FQHCs. To our knowledge, this is the first study on the response of primary care and prenatal care practices to FI during the pandemic in this largely rural region of the U.S. As we only assessed practice staff perceptions of FI during the pandemic, additional work is needed to evaluate FI from the patient perspective. Future studies are needed to determine which factors contribute to the ability of practices and their surrounding communities to respond to FI, the effectiveness and sustainability of food programs started during the pandemic, and the most promising approaches for practices to address FI.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319221106626 – Supplemental material for The Impact of the COVID-19 Pandemic on Food Insecurity in Northern New England Primary and Prenatal Care Settings
Supplemental material, sj-docx-1-jpc-10.1177_21501319221106626 for The Impact of the COVID-19 Pandemic on Food Insecurity in Northern New England Primary and Prenatal Care Settings by Kayla E. Hatchell, Chelsey R. Canavan, Tiffany D’cruze, Arvind Suresh, Alka Dev, Maureen Boardman and Meaghan A. Kennedy in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors thank Pablo Martinez-Camblor, PhD for statistical consultation on this manuscript. The authors also thank participating regional practice-based research networks for their collaboration in distributing the survey: The Dartmouth CO-OP Northern New England Practice-based Research Network, the Northern New England Perinatal Quality Improvement Network, the Bi-State Primary Care Association, and the Northern New England Clinical and Translational Research Network.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part the Hitchcock Foundation and by the Bureau of Health Workforce (BHW), Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services (HHS) under cooperative agreement #UH1HP29966. The information, conclusions and opinions expressed in this presentation are those of the authors and no endorsement by BHW, HRSA, or HHS is intended or should be inferred.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.