
Abstract
Introduction:
This study determined the clinic prevalence and compared the quality of care of allergic diseases in urban, rural, and remote primary care sites.
Methods:
This was a retrospective review of electronic health records of all adult patients who consulted in the 3 sites from May 2019 to April 2022. Data of adult patients with allergic diseases was extracted from the 3 EHR systems operating across the participating sites using standardized Structured Query Language queries across the 3 systems. We computed the prevalence of allergic diseases among adults who consulted in primary care health facilities by dividing the number of patients diagnosed to have an allergic disease over the total number of adult patients who consulted within the 3-year study period. We compared the quality of care of patients across the 3 sites based on clinical practice guidelines using Chi-square test, Fisher’s exact test, or 1-way analysis of variance, as appropriate.
Results:
The prevalence of allergic disease among adults who consulted in primary care health facilities was 1.3% for the urban site, 2.2% for the rural site, and 2.1% for the remote site. The most common allergic disease was asthma (59.0%). First-line medications based on recommendations in clinical practice guidelines were prescribed more often in the urban site, including inhaled corticosteroids with long-acting beta-agonists for asthma patients (P < .001) and topical corticosteroids for atopic dermatitis (P < .001). In contrast, there was more frequent prescription of medications that were not recommended in clinical practice guidelines in the rural and remote sites.
Conclusion:
Health inequity was observed in this study, with results demonstrating that the rural and remote sites had greater allergic disease prevalence, greater underutilization of first-line medications, and more frequent overutilization of non-essential medications.
Introduction
Allergic diseases are 1 of top 3 disorders identified by the World Health Organization that need to be prevented and controlled. 1 Allergic diseases encompass a broad spectrum of disorders, including asthma, allergic rhinitis, urticaria, allergic contact dermatitis, atopic dermatitis, drug allergy, and food allergy.1,2 Worldwide, it is estimated that 500 million people have allergic rhinitis, 300 million people have asthma, and 171 million people have atopic dermatitis. 1 The economic burden of allergic disease is tremendous, including both direct costs from medications, consultations, and hospitalizations, as well as indirect costs from absenteeism and productivity losses. A study in Asia reported that the indirect cost of inadequate treatment of allergic diseases is USD 105.4 billion annually. 3
There are several modifiable and non-modifiable risk factors for the development of allergic disease, leading to significant variation in the burden of allergic diseases across settings. 4 The prevalence of allergic rhinitis in the Philippines in 2008 was 20%. Respondents from rural areas had higher prevalence (22.1%) compared to those in urban areas (18%). 5 The prevalence of food allergy was 4.1% while the prevalence of asthma based on wheezing was 8.7% in the year 2008. 6 There is a need for updated epidemiologic data on allergic diseases affecting adults in the Philippines, and to examine health disparities across different Philippine sites.
The Philippine Primary Care Studies (PPCS) program of 2016 instituted various interventions to strengthen the Philippine primary care health system. These health system interventions were implemented in selected urban, rural, and remote sites, and included health financing (provision of a primary care benefit package), implementation of an electronic health record (EHR) system, and hiring and training of healthcare workers. 7 The urban site was the health facility at the state university in Metro Manila. The rural site was a fourth-class municipality. The remote site was also a fourth-class municipality and a geographically isolated and disadvantaged area (GIDA). 7 An important element in improving primary care services is quality of care assessment. Quality of care indicators include evaluation of adherence to existing clinical practice guidelines. 8
This study aimed to determine the prevalence and characteristics of allergic disease among adults who consulted in the PPCS primary care health facilities. Specifically, this study aimed to: (1) Determine the prevalence of allergic diseases among adult patients consulting at the urban, rural, and remote sites, and (2) Compare the quality of care for common allergic diseases in the 3 sites to existing recommendations from local clinical practice guidelines (CPGs), or from international CPGs if local treatment CPGs do not exist.
Methodology
Study Design
We conducted a retrospective review of the EHR records of all adult patients who consulted in the PPCS urban, rural, and remote sites from May 1, 2019 to April 30, 2022. Patients with any allergic diagnosis, such as atopic dermatitis, allergic rhinitis, asthma, food allergy, urticaria, drug allergy, and allergic contact dermatitis, were included.
Data Collection and Processing
The demographic and clinical data of patients in the PPCS sites were encoded real time by the healthcare workers into the EHR. Data of adult patients with allergic diseases was extracted from the 3 EHR systems operating across the participating sites using standardized Structured Query Language queries across the 3 systems. Prior to data extraction, all patient and visit identifiers were anonymized to ensure patient safety. To ensure data quality and integrity, internal validity was verified through a random sampling where approximately 5% of the extracted records were temporarily de-anonymized under secure conditions and manually compared against the source EMR records by the data manager.
The following data were extracted: visit number, location, month of consult, year of consult, age, sex, chief complaint, diagnosis (atopic dermatitis, allergic rhinitis, asthma, food allergy, urticaria, drug allergy, and contact dermatitis), ICD code, pharmacologic management, non-pharmacologic management, family history of allergic disease, disease classification, and implicated trigger. The number of consults of patients with allergic disease were also obtained, regardless of reason for consult. A data extraction tool was developed and pilot tested to guide the PPCS data management team on the variables to be collected. Missing data was encoded as ‘not reported’. The data extraction tool is found in the Supplemental Table 1.
Data Analysis
The data was presented using descriptive statistics. Categorical variables were reported using frequencies and percentages, while continuous variables were reported as mean and standard deviation (SD) if normally distributed, or median and interquartile range (IQR) if not normally distributed. Prevalence was computed as the number of patients diagnosed to have an allergic disease divided by the total number of adult patients who consulted within the 3-year study period. Chi-square test, or Fisher’s exact test when appropriate, was used to compare categorical variables across the 3 sites, while 1-way analysis of variance was used to compare continuous variables. The level of significance (alpha) was set at .05. Tukey’s Honestly Significant Difference (HSD) was used to perform pairwise comparisons of the 3 locations for cases where the 1-way analysis of variance yielded a significant test at 5% level of significance.
Adherence to quality indicators was assessed based on CPGs at the time of data collection (year 2019 or earlier). Specific recommendations are summarized in Supplemental Table 2. Adherence was computed as the actual number of prescriptions divided by the ideal number of prescriptions based on guidelines. Medications which were not mentioned in clinical practice guidelines were considered ‘non-essential medications’. Due to the small number of patients with drug allergy, food allergy, and anaphylaxis, the cases of these patients were simply described.
Ethical Considerations
This study received ethical approval from the University of the Philippines Manila Research Ethics Board (UPMREB 20-15-489-01). Data was anonymized to and stored in a password-protected laptop that only study investigators had access to. Data will be destroyed 15 years after study completion.
Results
During the 3-year study period, there were 12 000 adult patients with 23 109 consults in the urban site, 17 050 adult patients with 54 828 consults in the rural site, and 8614 adult patients with 19 928 consults in the remote site. There were 155 patients with an allergic disease in the urban, 382 in the rural, and 182 in the remote site. The clinic prevalence rates were 1.3%, 2.2%, and 2.1% respectively.
Across all sites, the most common identified allergic disease was asthma (59.0%). The most common coexisting allergic disease were bronchial asthma with allergic rhinitis (87 patients, 12.1%). There was a significantly higher proportion of patients with allergic contact dermatitis in the urban site (32.9%) compared to the rural and remote sites (P < .001). There was a significantly higher proportion of patients with atopic dermatitis (19.4%, P = .005) and allergic rhinitis (18.8%, P < .001) in the rural site. There a significantly higher proportion of patients with urticaria in the remote site (11.0%, P = .003; Supplemental Table 3)
A total of 843 consultations were made among the 685 adult patients with allergic disease, with an average number of consults at 1.2 (SD = 0.8). Across the 3 sites, majority were females (65.9%). The patients in the remote site were significantly older compared to the rural site (P = .0001) and urban site (P < .0001). Significantly more patients in the remote site had a family history of allergic disease (P < .001; Supplemental Table 4).
Allergic Diseases
Asthma
There were 424 adult patients with asthma who made a total of 576 consults across the 3 sites (average of 1.3 consults, SD = 0.9; Supplemental Table 5). Allergic rhinitis was a coexisting allergic disease in 13 patients of the urban site (15.3%), 72 patients in the rural site (31.7%), and 2 patients in the remote site (1.8%). One patient in the remote site also had a diagnosis of Chronic Obstructive Pulmonary Disease (COPD).
There were more patients with dyspnea as chief complaint in the rural site (32.7%), followed by the remote site (25.9%; P < .001) Significantly more patients presented with asthma in exacerbation in the remote site (28.9%) compared to the rural (19.0%) and urban sites (13.5%; P < .001). There were 2 patients in the remote site (1.2%) requiring hospital admission. Medications for exacerbation (inhaled SABA-SAMA, systemic steroids) were prescribed most often in the remote site compared to the rural and urban sites.
First-line medications for asthma, inhaled corticosteroids with long-acting beta-agonists (ICS-LABA) or ICS, were utilized more in the urban site compared to the remote and rural sites (P < .001). Second-line medications (due to lower efficacy or poorer safety profile), namely leukotriene receptor antagonists (LRAs) and oral short-acting beta-agonists (SABA), were more frequently prescribed in the remote site, followed by the rural site (P < .001 and P = .003 respectively).
Several medications not mentioned in the CPG were prescribed in the 3 sites. Antihistamines, vitamins, and expectorants were prescribed most frequently in the rural site (P < .001, P = .002, and P = .011 respectively). Oral LABA and mucolytics were prescribed most frequently in the urban site (P = .032 and P = .003 respectively). Herbal medications were prescribed more in the remote and rural sites, but the difference did not reach statistical significance (Table 1).
Clinical Characteristics and Management of Adults With Asthma.

Abbreviations: ICS, inhaled corticosteroids; IV, intravenous; LABA, long-acting beta-agonist; LRA, leukotriene receptor antagonist.; N, number of consults; OCS, oral corticosteroids; SABA, short-acting beta-agonist; SAMA, short-acting muscarinic antagonist.
P-values in bold show statistically significant difference across the 3 sites.
Recommended for patients in exacerbation.
Insufficient evidence to make a recommendation.
Allergic Contact Dermatitis
There were 143 patients with allergic contact dermatitis, who made a total of 160 consults (average of 1.1 consults, SD = 0.3; Supplemental Table 6). Across the sites, the most common chief complaint was rash (46.9%), followed by pruritus (23.8%). Majority did not have an identified trigger (94.8%).
The most commonly prescribed medication across the sites were oral antihistamines (66.3%), which is regarded as supportive treatment for pruritus. Topical corticosteroids (as first-line treatment) and oral corticosteroids (for severe disease) was prescribed more often in the rural and remote sites, but the difference did not reach statistical significance. Oral antibiotics were prescribed more often in the remote and rural sites, while topical antibiotics were prescribed more frequently in the urban site, although statistical significance was not detected. Topical antifungals were prescribed most frequently in the remote site, followed by the urban and rural site (P < .001). Non-essential medications (vitamins and topical antipruritics) were prescribed most often in the rural site (Table 2).
Clinical Characteristics and Management of Adults With Allergic Contact Dermatitis.
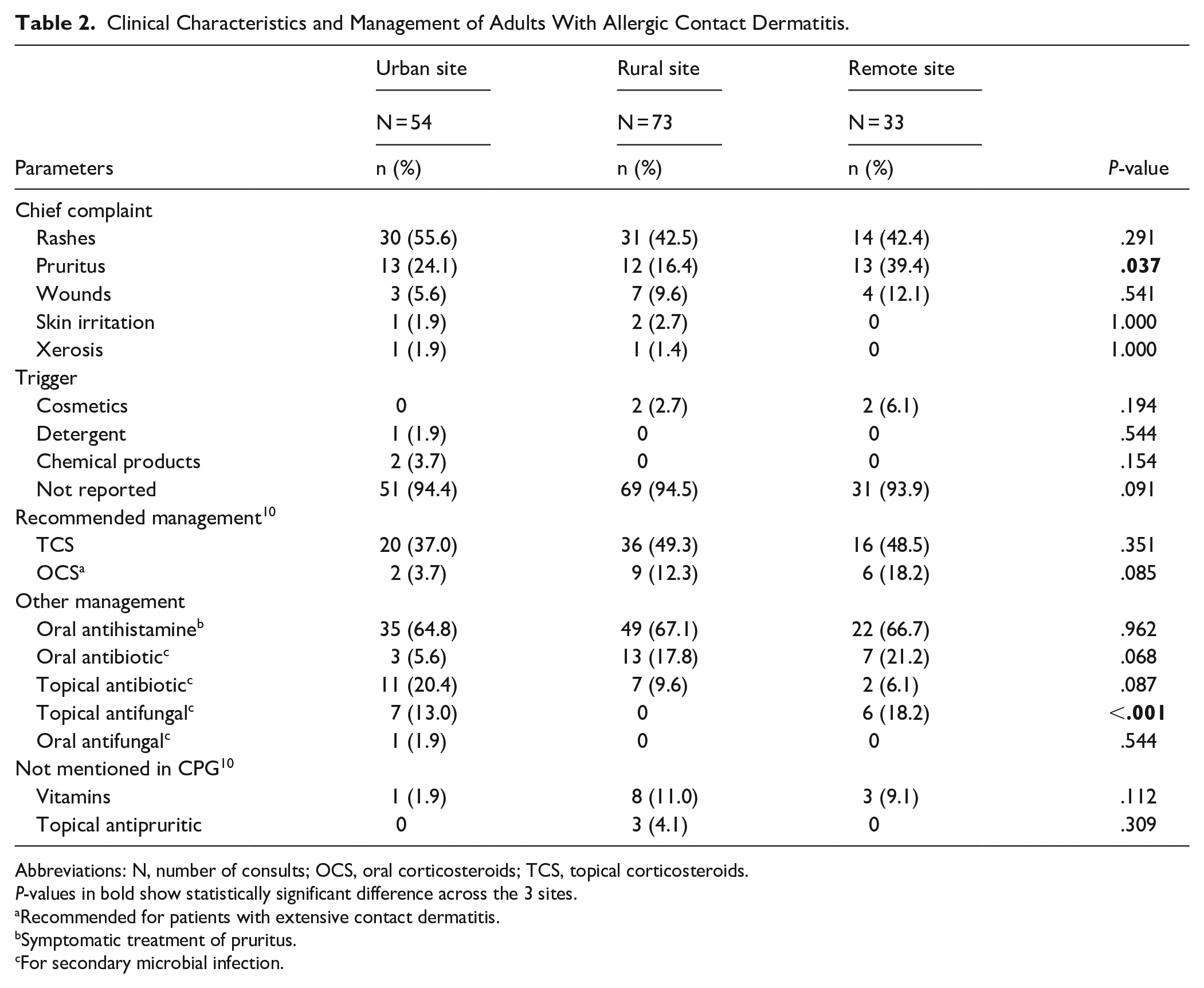
Abbreviations: N, number of consults; OCS, oral corticosteroids; TCS, topical corticosteroids.
P-values in bold show statistically significant difference across the 3 sites.
Recommended for patients with extensive contact dermatitis.
Symptomatic treatment of pruritus.
For secondary microbial infection.
Atopic Dermatitis
There were 110 patients with atopic dermatitis, who made a total of 124 consults (average of 1.1 consults, SD = 0.5). Majority came from the rural site (74, 67.3%). The average number of consults per patient was significantly higher in the remote site compared to the urban (P = .009) and rural site (P = .0005; Supplemental Table 7) The disease severity classification was not recorded for all patients.
The most common chief complaint was rash for the urban and rural sites, and pruritus for the remote site. The most commonly prescribed drug across the sites was antihistamine (62.1%), which is generally not recommended for management of atopic dermatitis. Antihistamine was prescribed most frequently in the remote site (P = .005).
Topical corticosteroids, the first-line medication, were prescribed most frequently in the urban site (52.9%), followed by the remote site (44.4%) and least often at the rural site (13.8%; P < .001). Oral corticosteroids, which is recommended only for acute, severe disease exacerbations, were prescribed most frequently at the remote site (44.4%), followed by the rural site (10.0%) and least often at the urban site (5.9%; P < .001). Non-essential medications, including topical antipruritics (calamine containing preparations) and vitamins were prescribed most frequently in the rural site (Table 3).
Clinical Characteristics and Management of Adults With Atopic Dermatitis.

Abbreviations: LRA, leukotriene receptor antagonists; N, number of consults; OCS, oral corticosteroids; TCS, topical corticosteroids.
P-values in bold show statistically significant difference across the 3 sites.
Recommended only for acute use during severe disease exacerbations.
For secondary microbial infection.
Antihistamines are not recommended for treatment of atopic dermatitis, although short-term use of sedating antihistamines may be considered for patients with disturbed sleep due to pruritus.
Allergic Rhinitis
There were 87 patients with allergic rhinitis, who made a total of 130 consults (average of 1.1 consults, SD = 0.2). All 87 patients also had coexisting bronchial asthma (Supplemental Table 8). The severity classification was not recorded for all patients. The most common chief complaint was dyspnea for the rural site (P = .001) and cough for the remote and urban sites (P = .038).
Among the recommended treatment, antihistamines were prescribed most often in the urban site (P < .001) while LRAs were prescribed most often in the remote site (P = .030). Intranasal corticosteroids were prescribed in only 2 patients in the rural site. Oral corticosteroids, recommended only for acute use in severe disease, was prescribed most often in the remote site (P = .009). Non-essential medications, including vitamins, herbal medication, mucolytics, and expectorants, were prescribed in the rural site. (Supplemental Table 8).
Urticaria
There were 47 patients with urticaria, who made a total of 50 consults (average of 1.0 consults, SD = 0.2). Urticaria was classified as acute in 2 patients (66.7%) in the urban site, 11 patients (55.0%) in the remote site, and 7 patients (29.2%) in the rural site. Chronic urticaria was noted in 2 patients (8.3%) in the rural site and 1 patient (5.0%) in the remote site. The rest of the patients could not be classified due to inadequate information in the records. Majority (91.5%) did not have any identified or suspected triggers identified in the records (Supplemental Table 9).
The most common chief complaint was rash in the urban and rural site, and pruritus in the remote site. Across the sites, the first-line medication antihistamine was the most commonly prescribed drug. Oral corticosteroids, recommended for acute exacerbations of urticaria, were prescribed more often in the rural site (29.6%), followed by the remote site (14.3%), compared to none in the urban site, but the difference did not reach statistical significance. Topical corticosteroids, which are not recommended, were prescribed in the rural site. Leukotriene receptor antagonists, where evidence is insufficient to create a recommendation, was also prescribed in the remote and rural site. Non-essential medications (vitamins and topical antipruritic agents) were prescribed in the rural site (Supplemental Table 9).
Drug Allergy
There were 6 patients with drug allergy (2 patients for each site), who made a total of 7 consults. The ages ranged from 20 to 84 years. The culprit drugs were antibiotics (1 patient in the urban site) and prednisone (1 patient in the rural site). The rest of the patients had no culprit drug specified in the patient records.
Food Allergy
There was 1 patient in the rural site who was suspected to have food allergy, but the culprit food was not specified in the patient records.
Anaphylaxis
There was 1 patient in the remote site with a diagnosis of anaphylaxis, but the trigger not specified in the patient records.
Adherence to Guidelines
Adherence to the recommended treatment across the sites is shown in Table 4. All sites had underutilization of ICS for asthma, with the rural and remote sites with significantly lower utilization of ICS (P < .001). All sites also had underutilization of topical corticosteroids for atopic dermatitis, which was most marked at the rural site (P < .001). Prescription of antihistamines for treatment of urticaria showed 100% adherence for the urban and remote sites, and slight underutilization in the rural site (81.5%).
Adherence to Recommended Treatment for Common Allergic Diseases.

Abbreviations: n, actual number of prescriptions; N, ideal number of prescriptions based on guidelines.
Discussion
The prevalence of allergic disease among adult patients who consulted in 3 primary care sites was 1.9%, with lower prevalence in the urban site (1.3%) compared to the rural site (2.2%) and remote site (2.1%). These findings are similar to the 2008 Philippine survey which showed lower prevalence of allergic rhinitis in urban compared to rural areas. 6 In contrast, international studies report lower prevalence of allergic disease in rural compared to urban areas.12,13 The higher rates of Mycobacterium tuberculosis and helminthic infection in urban areas in the Philippines may contribute to the lower allergy prevalence in this area.14,15 Mycobacterium tuberculosis has been shown to induce Th1 responses, which decreases the risk for developing allergic disease. 15 Chronic infections with certain intestinal helminths have been reported to confer protection against allergic disease. 14
Health disparities were observed across the 3 sites in terms of disease severity and clinical management. There was poorer disease control among asthmatic patients in the remote and rural sites, as evidenced by the significantly higher proportion of patients with dyspnea as the chief complaint and assessed to be in acute exacerbation. These findings are consistent with international literature reporting that asthmatic patients in rural sites compared to urban sites have increased morbidity and mortality risk. Reasons for this health disparity include economic disparities (lower income and insurance coverage), supply disparities (low supply of primary care providers and specialists), and limited access to available health care. 16
Oral corticosteroids and oral antibiotics were prescribed more often in the remote site and rural sites across the different allergic diseases. These results suggest more severe disease presentation with possible secondary bacterial infection necessitating systemic antibiotics. Another possible reason would be variation in physician prescribing practices, with increased prescription of corticosteroids and antibiotics in these sites. Overprescription of these drugs, particularly in rural communities, have been reported in both local and international literature.17,18
Significant underutilization of first-line medications for asthma and atopic dermatitis was observed in the study across all sites, with the rural site showing the lowest utilization. In contrast, second-line medications such as LRA, and other medications not included in the guidelines such as antimicrobials, vitamins, and expectorants were prescribed more often in the rural and remote areas. This finding points to a problem of underutilization of first-line medications, and overutilization of non-essential medications, which further aggravates health disparities.
A scoping review in low- and middle-income countries reported that the proportion of overuse in medicines ranged from 7.3% to 98.2%, with an interquartile range of 30.2% to 64.5%. The most common drug classes involved were antimicrobials, psychotropic drugs, proton pump inhibitors, and antihypertensive drugs. The drivers for overuse of medications included limited clinician knowledge, poor regulation, limited access to diagnostic facilities, patients’ demands for antibiotic therapy, and financial influences (industry influence and profitability of healthcare providers). 19
There are some limitations to this study. The data from this study was based on review of electronic health records. Certain important variables, including disease severity, response to medications, and non-pharmacologic advice, were often not recorded. This makes it difficult to assess the quality of care received by patients in the sites. Furthermore, there may be misdiagnosis and underdiagnosis of allergic diseases. The triggers for certain diseases such as asthma, atopic dermatitis, and allergic rhinitis may be allergic or non-allergic. Due to the unavailability of diagnostic tests needed to differentiate these in the primary care level, we included all patients diagnosed with these allergic diseases in this study. Future studies that explore patients’ and providers’ knowledge, attitudes, practices, and preferences are needed to understand the disparities observed in this study.
Conclusion
The prevalence of allergic disease among adult patients who consulted in primary care sites was 2.2% in the rural site, 2.1% in the remote site, and 1.3% in the urban site. Across all sites, the most common allergic disease was asthma. Health inequity was observed with the rural and remote sites experiencing greater disease prevalence, underutilization of first-line medications, and overutilization of non-essential medications.
Recommendations
Quality of care of common allergic diseases in the primary care setting in the Philippines may be improved through multifaceted strategies including wider dissemination of CPGs, provision of clinical decision aids, regular monitoring of quality of care, and timely provision of the results of the quality of care monitoring for clinician feedback and guidance. Improving quality of care is a critical component to reducing health disparities in the Philippine setting.
Supplemental Material
sj-docx-1-jpc-10.1177_21501319251353599 – Supplemental material for Quality of Care of Adult Patients With Allergic Diseases in Urban, Rural, and Remote Primary Care Sites in the Philippines
Supplemental material, sj-docx-1-jpc-10.1177_21501319251353599 for Quality of Care of Adult Patients With Allergic Diseases in Urban, Rural, and Remote Primary Care Sites in the Philippines by Carol Stephanie C. Tan-Lim, Robbi Miguel G. Falcon, Jeremiah F. Feliciano, Michael B. Fong, Mark Anthony U. Javelosa, Leonila F. Dans, Iris Thiele C. Isip-Tan, Josephine T. Sanchez, Mia P. Rey and Antonio Miguel L. Dans in Journal of Primary Care & Community Health
Footnotes
Acknowledgements
The authors would like to thank the field staff in the University of the Philippines Diliman, Samal, Bataan, and Bulusan, Sorsogon.
Authors Note
Michael B. Fong and Iris Thiele C. Isip-Tan is also affiliated to Medical Informatics Unit, College of Medicine, University of the Philippines Manila, Philippines.
Antonio Miguel L. Dans is also affiliated to 6 St. Luke’s Medical Center, Health Equity Research Foundation, Taguig City, Metro Manila, Philippines.
Ethical Considerations
This study received ethical approval from the University of the Philippines Manila Research Ethics Board (UPMREB 20-15-489-01). Data was anonymized to and stored in a password-protected laptop that only study investigators had access to. Data will be destroyed 15 years after study completion.
Consent to Participate
Written informed consent for involvement in PPCS-related research was obtained from all patients at the PPCS sites.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Philippine Department of Health (DOH), the Philippine Health Insurance Corporation (PhilHealth), the Emerging Interdisciplinary Research Program (EIDR), the University of the Philippines Center for Integrative and Development Studies (CIDS), and the Philippine Council on Health Research and Development (PCHRD).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available upon request from the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.