
Abstract
Background:
Primary care physicians’ (PCPs) prescription of oral anti-diabetic drugs (OADs) is pivotal to optimise glycaemic control of patients with type 2 diabetes mellitus (T2DM). Their decision-making process is not well-understood and is postulated to be multi-factorial. The study aimed to explore the factors influencing the prescribing behaviour of PCPs managing patients with T2DM in an urban setting.
Methods:
A qualitative methodology using a descriptive-interpretive approach was employed for this study. Qualitative data from 23 PCPs was collected via 3 focus group discussions and 10 in-depth interviews using a semi-structured topic guide. PCPs with various experiences, qualifications and backgrounds were purposively recruited from public and private primary care clinics in Singapore. The audio-recorded interviews were transcribed verbatim and audited for accuracy. Thematic analysis was conducted and the emergent themes were grouped under the domains of the ‘Generalist Wheel of Knowledge, Understanding and Inquiry’ framework. The data was managed using Nvivo qualitative management software.
Results:
The 4 main themes identified were clinician experience and knowledge, patient clinical risk stratification and preference, diabetes severity and drug factors, and healthcare system. PCPs’ prior experience with OADs, years of practice, academic roles and knowledge resources influenced their decision-making when prescribing OADs. Their prescription was guided by patient preferences and comorbidities, such as selecting sodium-glucose cotransporter-2 inhibitors for patients with proteinuria. Disease severity, OADs safety profile, efficacy, stipulations in the drug formulary, cost and availability of OADs in their pharmacy, and social worker support were other factors affecting PCPs’ prescribing habits of OADs. Clinical decision support functionality in the electronic medical record (EMR) system prompted PCPs to select the type of OADs during the consultation.
Conclusions:
The study highlights the multifaceted factors influencing PCPs’ prescribing of OADs, including clinical experience, patient preferences, drug formulary limitations, medication costs and EMR utilisation. To enhance prescribing habits, interventions should focus on continuous education for PCPs, expanding drug formularies, addressing patients’ preferences, cost and access barriers through subsidies and promoting the adoption of EMRs with clinical decision support systems in both public and private sectors.
Keywords
Introduction
Globally, the number of adults with type 2 diabetes mellitus (T2DM) is over 537 million and is projected to increase to over 643 million by 2030. 1 Diabetes-related deaths reached 6.7 million worldwide in 2021, with poor glycaemic control causing an additional 2.2 million deaths due to cardiovascular and chronic kidney disease. 1 In Singapore, the prevalence of diabetes is expected to increase to 13.7% by 2030 from 8.6% in 2017. 2 Recognising this significant disease burden to this tiny island state, Singapore launched a ‘War on Diabetes’ in 2016, 3 emphasising the need for effective T2DM management to reduce its morbidity and mortality. 4
T2DM management includes both non-pharmacological and pharmacological therapy. Oral anti-diabetic drugs (OADs) are regarded as ‘weapons’ to optimise the glycaemic control of patients with T2DM and reduce their risks of debilitating vascular complications. Over the past decade, newer OADs have been available for T2DM management, including DPP4 (dipeptidyl peptidase-4) inhibitors or incretin mimetics, glucagon-like peptide-1 (GLP1-ra) agonists and sodium-glucose cotransporter-2 (SGLT-2) inhibitors.5,6 These OADs, designed to target specific pathways in T2DM management, effectively lower blood glucose levels, improve glycaemic control and mitigate associated cardiovascular and renal complications. International and local clinical practice guidelines direct physicians to prescribe these medications appropriately.7 -9
Despite the availability of these medications and evidence-based guidelines on T2DM management, a systematic review revealed that therapeutic inertia, or the failure to initiate or intensify medications when indicated, is a major concern in managing hyperglycaemia in patients with T2DM, especially in Western countries. 10 Literature also reports non-clinical influences which impact the medication prescribed by physicians; these include patient’s expectations, personal characteristics, physician personal characteristics, clinical practice setting and local management policies. 11 With the availability of newer OADs, it would be essential to understand the evolving thought processes and impact on the OADs prescribing behaviour of primary care physicians (PCPs).
A survey of American specialists and academic generalists reported that physicians relied on various clinical and patient-related factors to guide OAD prescriptions. 12 DPP4 inhibitors and metformin were preferred as first-line OADs in a survey of Japanese physicians. 13 A qualitative systematic review highlighted the need to upskill the PCPs and to moderate their emotions as essential factors to enhance their therapeutic management of their patients with T2DM. 14
PCPs manage most patients with T2DM in Singapore in a dual private and public fee-for-service healthcare system. Consultation fees and the cost of OADs, partially subsidised by the government, can vary between private and public primary care clinics. De Foo et al 15 have reported improved glycaemic control among patients treated by PCPs receiving these subsidies. With rising T2DM prevalence in the local multi-ethnic Asian population, PCPs’ role in its management becomes pivotal to alleviating the disease burden. 16 However, despite the increasing availability of newer classes of OADs, metformin and sulfonylureas continue to be the main medications used by patients with T2DM in Singapore. 7 The prescribing behaviour of PCPs is poorly understood, as few studies over the past decade have delved into their decision-making process in selecting the OADs for their patients.
Thus, the current study aimed to explore factors influencing the prescribing behaviour of OADs by PCPs. Understanding the factors influencing OAD prescription in T2DM treatment initiation and therapy intensification may enable PCPs to develop a rational shared decision-making approach in selecting OADs that will be acceptable to their patients with T2DM.
Methodology
Study Design
Qualitative methodology using a descriptive-interpretive approach explored factors influencing the PCP’s prescribing habits of OADs through in-depth interviews (IDIs) and focus group discussions (FGDs). 17 Such an approach allows the researchers to explore new frontiers by uncovering richer insights into the experiences and perspectives of the participants and interpreting them in the appropriate context. 17
Theoretical Framework
The Generalist Wheel of Knowledge, Understanding and Inquiry was selected and adopted as the theoretical framework. 18 The framework offers a structure for comprehensive patient care in family medicine. It weaves together 4 domains: ‘clinician’ (clinician knowledge and skills), ‘patient’ (the patient’s unique background and illness perspective), ‘disease’ (established disease knowledge) and ‘healthcare system & policy’ (the surrounding healthcare system with its limitations and policies). The domains are also interconnected via ‘information mastery’, ‘relationship’, ‘justice’, ‘prioritisation’, and ‘integration’. This interconnected view empowers physicians to make informed decisions which consider not just the disease process but also the perspective of the individual patient and the realities of the healthcare environment where the physician practises.
Research Team
A team consisting of 1 male (TNC) and 4 female PCPs (NL, SC, SM, PC), a female nurse clinician (LLG), 2 female medical students and 1 male medical student (NH, BL, LZH) were assembled to conduct the study. TNC is a senior researcher experienced in both qualitative and quantitative research methodologies. All PCPs and nurse clinicians are trained in conducting qualitative studies. The 3 medical students received qualitative training while doing the study. All PCPs and nurse clinicians routinely manage and counsel patients with diabetes in the primary care setting.
Study Setting
In Singapore, primary care services are provided by both public and private primary care clinics. The primary site for this study was a public primary care clinic in Singapore, situated in the Bukit Merah estate in the southern part of Singapore. This clinic serves a community with a significant number of adults suffering from chronic diseases, including T2DM. The clinic’s registry includes 9175 patients, of which 11.2% are diagnosed with T2DM.
Study Population and Recruitment
PCPs with varying levels of experience and postgraduate family medicine training qualifications, including the Graduate Diploma in Family Medicine (GDFM), Masters of Medicine in Family Medicine (MMed(FM)) and the Fellowship programme (FCFPS), 19 practising in public and private ambulatory primary care settings and managing patients with T2DM (self-reported by the PCPs), were eligible for this study. PCPs not in active clinical practice, working in tertiary or community hospitals and those not involved in managing T2DM patients were excluded from the study.
Eligible PCPs were invited to participate in the study via email or in-person. They were purposively selected and recruited based on maximum variation in their levels of training, years of experience and practice settings (working in both private and public primary care). Written informed consent was obtained from the PCPs before arranging a face-to-face or a virtual interview. IDIs were conducted for senior PCPs holding specific academic and administrative positions. It allowed them to share their unique perspectives and experiences in greater depth. For the FGDs, PCPs with similar experience and qualifications were included to create a conducive environment for open discussion without undue influences from their senior peers. The interviews were conducted over 7 months from April to November 2022.
Study Instruments
Demographic Characteristics and Practice Profile
PCPs were given a demographic characteristics data form (Appendix 1) to collect data such as basic demographics, seniority at the place of practice, length of practice in primary care and postgraduate qualifications.
Topic Guide
A semi-structured topic guide (Appendix 2) was developed based on literature review, discussion with the research team and the theoretical framework. The topic guide was pre-tested on 2 PCPs and revised before subsequent interviews. The same topic guide was chosen for both IDIs and FGDs to ensure consistency in data collection. Additionally, the semi-structured nature of the guide provided flexibility as researchers could probe specific topics while adapting to participants’ responses during both FGDs and IDIs. The topic guide covered PCPs’ management of patients with T2DM, their experience with OADs, the practical aspects of their prescribing habits, their methods of engaging patients during OAD selection and their views on artificial intelligence in T2DM management. These broad, open-ended questions enabled participants to address the 4 key domains of the Generalist Wheel theoretical framework. 18
Data Collection
PCPs completed the demographic data collection, followed by the interview. The interviews were either IDIs or FGDs, conducted in-person or remotely via video conferencing platforms. The FGDs consisted of the same category of PCPs to enable free sharing of ideas and to ensure that the junior PCPs do not feel intimidated by their senior colleagues. PCPs working at and participating in the study site were interviewed at the study site. Remote interviews were conducted over teleconferencing platforms as an interim measure during COVID-19. The same questions from the semi-structured topic guide were used in the IDIs and FGDs. All interviews were audio recorded. Each FGD or IDI session lasted 40 to 60 min. There were no repeated interviews.
Data Analysis
The recorded audio was transcribed verbatim and checked for accuracy. Two researchers (NL and SM) read and re-read the transcripts to familiarise themselves with the transcripts. An inductive and deductive thematic analysis approach was adopted. The inductive thematic analysis was employed to identify themes directly arising from the data. The deductive elements were guided by the theoretical framework and were linked with the main research questions. The first 3 interviews were coded line-by-line (open coding) independently by NL and SM. The investigators deliberated these codes and harmonised them. Codes with similar content were grouped into categories and further refined to develop an initial coding frame (axial coding) before the subsequent interviews. All contradictory responses were accepted for analysis, and any discrepancies were resolved after discussions with a third investigator (TNC). The data was managed using Nvivo qualitative data management software. The emergent themes identified were subsequently summarised under the Generalist Wheel of Knowledge, Understanding and Inquiry domains. 18 Representative quotes were chosen to illustrate the study findings effectively through a collaborative agreement among the investigators. Data collection and analysis were performed concurrently as an iterative process until data saturation. No new data emerged after 3 FGDs and 8 IDIs; subsequent 2 IDIs were conducted to ensure data saturation. 20
All the demographic data collection forms, audio recordings, transcripts, field notes, coding frames and codes were maintained in secure archives.
Rigour
To ensure the quality and consistency of the interviews, a single trained researcher (NL) conducted all interviews using a standardised topic guide developed with input from independent PCPs with special interests in diabetes management. Trained researchers regularly met and ‘challenged’ their data interpretation to ensure that data interpretation and analysis were unbiased. The researchers constantly reflected to mitigate the potential bias due to their professional and academic backgrounds.
Results
A total of 26 PCPs were approached, and 23 consented to participate (response rate 88.5%). Reasons for declining participation included time constraints, lack of interest or other commitments. All PCPs completed the demographic data collection form and the interviews. Ten individual IDIs and 3 FGDs were conducted.
Participant Characteristics
The demographic characteristics and practice profiles of the 23 PCPs recruited are reported in Table 1. The majority of the PCPs were females (70%) who were working in the public primary care (polyclinic) 21 setting. The median age of PCPs and years of practice were 37 years and 11 years, respectively. The majority of the participants were educators (44%), followed by advisors/leaders (22%) and researchers (4%). Clinical educators included PCPs involved in medical undergraduate and postgraduate teaching, whereas, advisors/leaders had various advisory and leadership roles in clinical workgroups and clinics.
Characteristics of Participating PCPs.
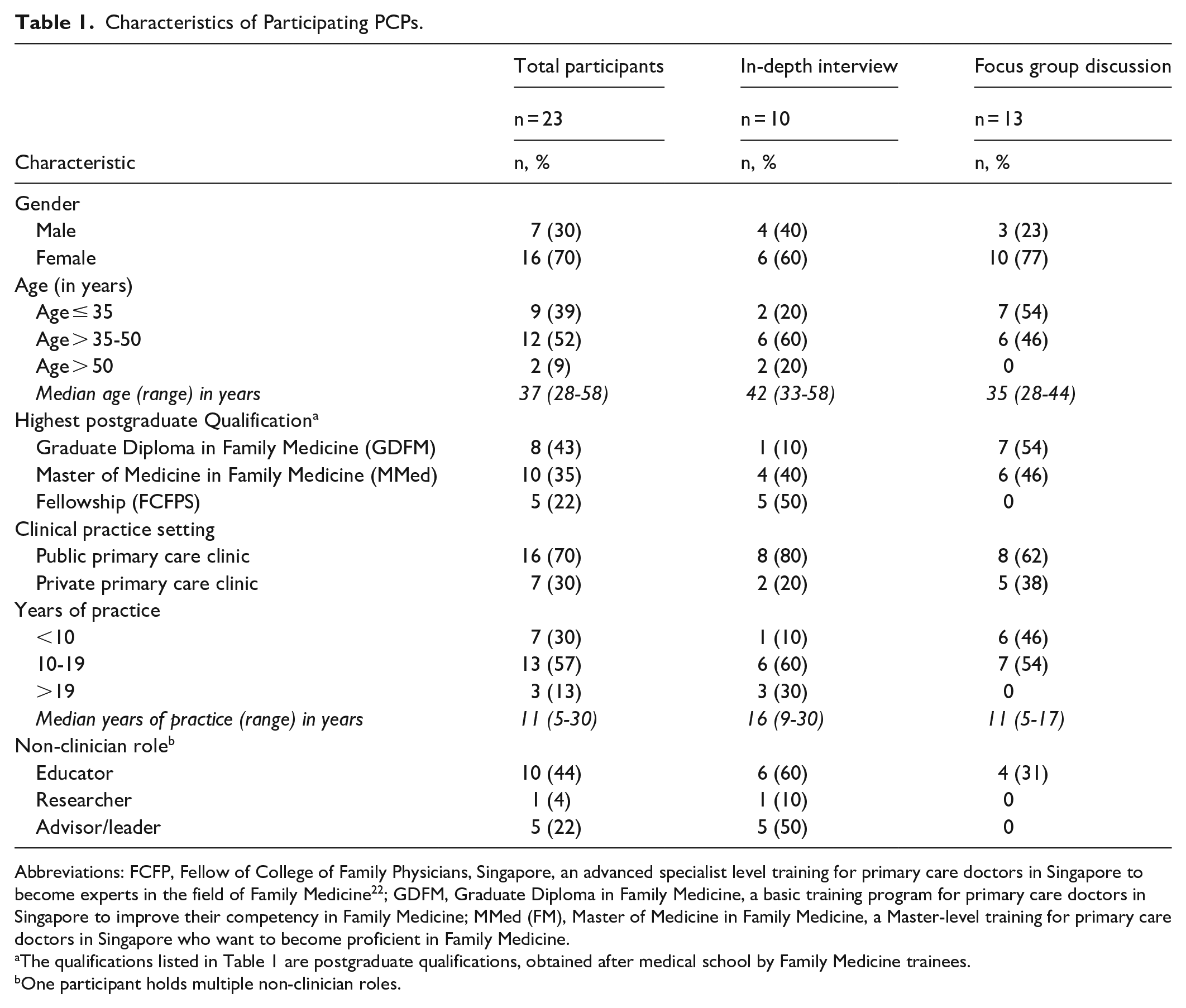
Abbreviations: FCFP, Fellow of College of Family Physicians, Singapore, an advanced specialist level training for primary care doctors in Singapore to become experts in the field of Family Medicine 22 ; GDFM, Graduate Diploma in Family Medicine, a basic training program for primary care doctors in Singapore to improve their competency in Family Medicine; MMed (FM), Master of Medicine in Family Medicine, a Master-level training for primary care doctors in Singapore who want to become proficient in Family Medicine.
The qualifications listed in Table 1 are postgraduate qualifications, obtained after medical school by Family Medicine trainees.
One participant holds multiple non-clinician roles.
Main Findings
The findings of factors influencing PCPs’ prescribing habits in managing patients with T2DM are grouped into themes and subthemes according to the domains of the Generalist Wheel of Knowledge framework. 18 A summary of the themes and subthemes are illustrated in Figure 1.

Themes and subthemes on factors influencing PCPs prescribing habits in managing patients with T2DM.
Clinician: Experience and Knowledge
. . . I base my (decision) on the local guidelines, and it is called ACE clinical guidelines. . .they give us a table, a flowchart to say which one is first line, then (for) second line, you can consider either SGLT2 inhibitors or sulfonylureas. (P9, Educator, 11 years of practice) . . . based on all the recent talks and not guidelines, CMEs, (if) patient has kidney or heart failure, you can start discussing about SGLT2 inhibitors as a starting point (of medication). (P3, Educator, 9 years of practice)
I’m in the ministry’s drug advisory committee, that’s when they talk about which drugs to subsidise and so recently, sitagliptin came from that kind of discussion. And that makes me read up about DPP4 inhibitors, sitagliptin. That will remind me of this drug, and when I come back to polyclinic, I might use this more, because of that knowledge. (P5, Educator, Advisor/Leader, 25 years of practice) I guess there are various factors that are non-clinical, that influence how I practice overtime. For example, through dabbling in research and learning how to read a journal or critique a journal, helps me to keep up to date with the latest evidence and try to apply that evidence to my pool of patient(s). (P6, Educator, Advisor/Leader, 10 years of practice) I teach the residents from the GDFM, MMed, those two levels, and educate the medical students that come for attachment. So, I share with them the latest guidelines available. Apart from that, I’m in the endocrine specialty advisory group, and we actually go through the latest research and try to incorporate that into our clinical practice guideline. So, that somehow indirectly affects how I practice. (P6, Educator, Advisor/Leader, 10 years of practice)
Many PCPs preferred initiating and titrating the OADs based on their own experiences, with a tendency to maximise multiple OADs first, before broaching conversations about insulin initiation:
If it’s a monotherapy, I would increase gradually to the upper limit (of medication dose), and if it doesn’t work, then (start) a dual therapy. Usually, my preference is that if the patient is already on dual or triple maximum OADs, I would have discussed the role of insulin. (P21, Educator, Advisor/Leader, 18 years of practice)
Patient-Centred Care
For elderly diabetics, we tend to be not-so-aggressive in upfront pharmacotherapy. Whereas for the younger diabetics, sometimes we will select a few which we feel might benefit from aggressive pharmacotherapy, to remove the glucose toxicity, in hopes of a future recovery of the pancreas. (P21, Educator, Advisor/Leader, 18 years of practice) . . . I talk about the occupation first. I want to find out whether they are working regular hours or are they working shift. What are their meal times? Are their meals taken at home, work or outside? Can they bring the medicines along with them even to work? As that would affect the timing of the medicines. (P22, Advisor/Leader, 14 years of practice) If they are not elderly, it depends on also whether they are obese, like high BMI, whether they have other comorbidities like ischaemic heart disease, hypertension, chronic kidney disease and so on. (P1, Advisor/Leader, 24 years of practice)
PCPs factored in comorbidities like proteinuria when initiating or up-titrating certain medications such as the SGLT2 inhibitors:
. . . the other factors, like proteinuria, if they have proteinuria, then I would like to consider SGLT2 inhibitors or if the sugar is difficult to control or if there are weight issues. (P4, Educator, Researcher, 30 years of practice)
Because if it’s (previous experience is) a bad side effect, patient won’t take it. Those are the patient experience. In fact, I tell them this is the side effect of the medication, if they (are) not agreeable to continue with it, or if they say, “Oh I have tried it for two weeks. Still cannot get over that (side effect).”, then I will either reduce or stop it altogether. (P3, Educator, 9 years of practice) . . . I mean, patient preference, sometimes patients ask for it. You know, (they) see their family members also taking that (medication). (P23, Educator, 12 years of practice)
One PCP was concerned that patients’ requests to discontinue medications were influenced by negative news; this was despite the medication improving their glycaemic control:
Unfortunately, the news came out that sitagliptin has a slight increase with ischemic heart disease, and then, all of the sudden, a lot of patients came in, telling me that they have chest pain. In fact, one of them told me that he had chest pain and it’s because we gave him the medication. So, unfortunately, we have to stop the medication, but it took quite a lot of explanation, especially when the news broke out (that) it has increased risk of ischemic heart disease, even though the patients have a better or normal HbA1c (glycosylated hemoglobin) control (with the medication). (P17, 17 years of practice)
Healthcare System and Clinical Decision Support System
. . . our polyclinic has got a pharmacy and a formulary here, it’s convenient for patients to use medications that we have here. . .But if a medication is not available here and it’s important for that patient to have this medication, then we can always write a prescription, but they will then need to go to either the private pharmacy or the nearby hospital to pick it up. It’s not just a one-off, but it’s a chronic medication, so some patients may not find it convenient,. .they would still want a medication that is available in the polyclinic itself. (P5, Advisor/Leader, 25 years of practice) We need to place an emphasis on logistics stability, that is the medicine can be readily available, so that we can supply our patients. We look at a few things, such as the availability of the medication. (P21, Educator, Advisor/Leader, 18 years in private practice)
. . . the clinical decision support built into the EMR that I use to manage the patient’s condition. So, they can help to trend the sugar control. It can show what the underlying medical issues a patient has. . . .that will give more information to help decide what kind of medications you (physician) want to start the patients on. Through the past records, can also see whether the patient has started on, like, various classes of diabetic medications, and then you (physician) can decide (and) it can help filter out those medications that are not suitable for the patient, because they (patients) have tried it and they cannot tolerate it. (P1, Advisor/Leader, 24 years of practice) I think, because my institution uses a computer system where the price of the medications gets auto-populated, so that helps in my decision on deciding on the medications. (P9, Educator, 11 years of practice)
. . for the cost, it depends on the patient’s insurance policy cover or whether they are having any subsidies or not. So, there are quite many government subsidies which can allay some of the costs. But still, I would say mostly would be quite pricey as well. Those who are on certain form of company coverage, I find it easier to prescribe certain medicines, because some of them are covered. (P16, 9 years of practice) So, after that, we will actually make an appointment to see the social worker, to try and work out how much subsidy they can actually get, while prescribing this medicine first. (P14, 6 years of practice)
Diabetes Severity and Drug Factors
. . . unless the HbA1c is very high and even if the patient controls the diet, it’s not likely to come down to the target level, then I would increase the medication. If the HbA1c is only maybe less than 8%, then I would provide diet advice first, and then get the patient to come back another time to check on the sugar. I’m not very aggressive. I’m more conservative, because I would give the patient an earlier review, but I wouldn’t want to rush into medications for the patient. (P1, Advisor/Leader, 24 years of practice) I would also need to look at the HbA1c so, in assessing the severity of the T2DM because that would allow me to decide whether I should start just one OADs, or whether I should start two and titrate accordingly. (P2, Educator, 10 years of practice)
However, few PCPs also revealed that their medication titration depended on patient symptoms rather than the glycaemic control or disease severity:
. . . when I would consider reducing the medication depends on their (patients) hypoglycaemic symptoms. So, if they are having hypoglycaemia symptoms at a HbA1c of less than 7.5%, I may consider cutting down on their medication. So, it really depends on their symptoms, rather than a specific level. (P6, Educator, Advisor/Leader, 10 years of practice)
In addition to glycaemic control, PCPs reported that the next key determinant of choice of OADs was to reduce or prevent diabetic complications:
So, there are quite a number of factors that I need to discuss with the (patient) for choosing the next step of treatment. But ideally, I’ll base (it) on patients’ complications that he or she is currently having. (P16, 9 years of practice)
. . . because we do recognise that diabetes is a chronic disease. We try to calculate and help the patient budget, such that the patient can remain (on) an affordable treatment. The important over-riding factor is compliance, so if the patient mentions the treatment is too costly, and the patient is unable to afford it or cannot take it regularly or on time, then the outcome of the treatment will be poorer, so we do take into consideration all (of) that when prescribing. (P21, Educator, Advisor/Leader, 18 years of practice) For SGLT2 inhibitors like dapa(gliflozin) or like empagliflozin, I find that it tends to bring down the HbA1c quite well, but it’s quite expensive. (P12, 5 years of practice)
Potential side effects of some medications, such as hypoglycaemia, flatulence and urinary tract infections, were considered by the PCPs while initiating or titrating certain OADs:
acarbose, I use it rarely. In fact, I don’t usually start acarbose, because it’s expensive and it causes a lot of abdominal bloatedness. (P6, Educator, Advisor/Leader, 10 years of practice) A few things will affect my decision on adjusting the OADs, be it increase, decrease or change. First, whether the patient had side effects to the medications, like gastrointestinal symptoms with metformin, urogenital symptoms with SGLT2 inhibitors, (and) hypoglycaemia with sulfonylureas. (P8, Educator, 11 years of practice)
PCPs also chose OADs based on their potency:
. . . the other factor is the potency of the drug itself. Nowadays, I don’t really use medications like acarbose. I think they are quite costly, and I find that they are not really effective. For the other group, like the DPP4 Inhibitors, I find that it’s gentler. Most patients actually tolerate it quite well, but it also doesn’t seem to be very potent. (P4, Educator, Researcher, 30 years of practice) I think the evidence for metformin is very strong. Additionally, the risk of hypoglycaemia is low. I think it also helps with the weight loss. So, in terms of side-effects-wise, I think metformin has one of the better side effect profiles and also better efficacy. (P6, Educator, Advisor/Leader, 10 years of practice)
Discussion
Our study highlights the multi-factorial influences on PCPs when they prescribe OADs. PCPs who were familiar with evidence-based practices felt confident prescribing according to established guidelines. Previous clinical experience also influenced the prescribing decisions of OADs by the PCPs. However, some PCPs hesitated in prescribing certain OADs due to consideration of patient preferences, limited drug formulary and medication cost. EMRs with embedded CDSS prompted PCPs in the public sector to prescribe OADs individualised to patient profiles.
Our study found that PCPs who helmed various academic roles and clinical advisory committees in addition to clinical work, were likely to keep abreast of updated guidelines for OADs prescription. These PCPs were inclined to apply these guidelines while optimising medications or adding newer agents such as SGLT2 inhibitors. Limited existing literature directly explored how PCPs’ academic roles influence their clinical practice, particularly their prescribing behaviours. However, a systematic review of studies from America and Europe informed that the quality of care among physicians decreased with increased clinical experience. 23 Senior physicians were less likely to adhere to recommended practices or adopt newly proven therapies. They were less receptive to new standards of care due to unfamiliarity with evidence-based medicine and quality assurance techniques. 23 While PCPs in academic roles may often be senior clinicians, their active engagement in teaching, research and committee work may foster a culture of continuous learning and exposure to current best practices, potentially creating a different dynamic than that in earlier studies. Peterson et al 24 observed that providing guidance and reminders on appropriate management practices improved diabetes management and outcomes. Thus, encouraging PCPs to take on academic and clinical advisory roles could ensure they receive continued education. Future studies should consider assessing the influence of various academic roles on clinical practice.
PCPs perceived that patients’ preferences influenced the initiation or continuation of specific OADs by their physicians. Additionally, one PCP in our study highlighted the influence of news on patient preferences. Similarly, Broom 25 reported that patients had challenged healthcare professionals’ selection of OADs due to skewed or non-scientific media reports. Conversely, reliable, evidence-based social media can empower patients to comply with physician recommendations. 26 Therefore, PCPs should be mindful of the influence of news and social media on patient preference and direct patients to reliable evidence-based information through official platforms like the Ministry of Health or local healthcare institutions’ websites, portals or mobile applications. These platforms provide accurate health information tailored to the local context. In addition, effective communication and rapport between the PCP and patient is crucial to rectify fabricated and unsolicited information and ensure patient acceptance of prescribed treatment. 27 It paves the way for shared decision-making during the consultation, as patients are also more willing to listen and heed advice from their PCP if they can get involved and play a part in managing their health. 28
One of the challenges highlighted by PCPs in the private sector was the reduced availability of OADs they could prescribe due to a limited drug formulary. A study by King et al 29 in 2019 found that the commonest OADs prescribed were metformin and sulphonylureas because these were affordable and available at all on-site pharmacies in the health system, whereas SGLT2 inhibitors and Glucagon-like peptide-1 agonists (GLP1-ra) were less prescribed due to their high cost despite their numerous benefits. Limited availability and accessibility of OADs were a pivotal barrier to optimal prescribing by PCPs, particularly in the private sector.30,31
In addition to prioritising OAD prescriptions based on the available drug formulary, PCPs also considered drug affordability while prescribing OADs.31,32 In Singapore, patients must pay out-of-pocket for healthcare services and medications. Medication costs can be high, especially for certain OADs, such as DPP4 inhibitors and SGLT2 inhibitors. Like our study, another local study on PCPs’ prescribing behaviour of anticoagulant therapy for the management of non-valvular atrial fibrillation found that medication cost was a barrier to prescription, especially for patients who have financial constraints. 33
To address financial constraints faced by needy patients, medical social workers support the PCPs in the polyclinics by reviewing the socioeconomic status of referred patients and arranging for higher subsidies of expensive medications for eligible patients. In contrast, such a service is hitherto unavailable in private clinics to address medication cost. Primary Care Networks were set up by the Singapore Ministry of Health in 2020 to enable PCPs in private practice to offer medical social services for their patients. 34 PCPs enrolled in Primary Care Networks can now offer medications at a lower cost to their patients who require financial assistance; this might eventually allow more patients in the private sector to have ready access to OADs, despite their economic status.
Similar to our findings, literature has shown that decision support tools integrated with EMR systems increase efficiency, reduce prescription errors and improve patient safety. 35 Such tools are increasingly incorporated in the EMR in local primary care practices, which will assist PCPs in prescribing evidence-based therapeutics safely and appropriately to their patients with T2DM. However, it can trigger privacy and security concerns, over-dependence on technology and decreased autonomy among physicians. 35 Thus, such tools’ utility, usability, and acceptability must be assessed in future studies to widen their adoption by PCPs.
The diverse factors influencing OAD prescribing in primary care have significant clinical implications and contribute to practice variability. To reduce this variability and promote equitable, evidence-based care, a clearer understanding of these influences is essential for aligning real-world prescribing with clinical guidelines. This alignment is crucial for optimising glycaemic control and improving outcomes for patients with T2DM. By addressing factors like guideline familiarity, patient preferences and drug access, more standardised and effective prescribing practices can be fostered in primary care.
Strengths and Limitations
The use of the Generalist Wheel framework is a strength in this study. It enables a more comprehensive understanding of the complex inter-related issues influencing OAD prescribing behaviour among PCPs. This framework also serves as a model to address specific areas within primary care, such as empowering patients in shared decision-making and integrating evidence-based decision support systems for appropriate OAD prescribing. Combining FGDs and IDIs enhanced our findings; FGDs allowed participants to contest each other and share everyday experiences, while IDIs delved into individual experiences.
There are limitations in restricting the data analysis and findings to a specific theoretical framework, as some findings relating to prescribing habits may not be captured adequately. Considering the breadth of the findings based on the theoretical framework, these findings sufficiently highlight barriers to prescribing habits among PCPs. Addressing these factors can improve the appropriate prescribing of OADs for patients with T2DM. The study did not specifically examine how the prescribing behaviour of PCPs varies across different sub-categories of their patients with T2DM, based on their glycaemic control status. Nevertheless, PCPs shared that the severity of the disease influenced their decision to initiate or titrate medications in addition to lifestyle modification measures. Logistical challenges led to FGDs involving PCPs from the same institute, potentially introducing homogeneity bias, as participants may share similar perspectives due to their common background. However, IDIs included PCPs from diverse backgrounds to ensure adequate representation of diverse opinions and insights. PCPs highlighted perceived patient factors which influenced their prescribing habits. However, such perception could not be verified as this study did not directly explore patients’ perspectives. A qualitative research study to gather the patients’ views on their T2DM management in primary care is being planned in the next phase of the study. The results of this study are specific to PCPs managing Asian patients with T2DM in a dual primary healthcare system. Thus, the findings will need to be contextualised and cannot be generalised to other healthcare professionals in different settings.
Conclusion
This study offers a novel contribution by specifically highlighting the significant influence of academic roles undertaken by PCPs on their prescribing practices for OADs. Beyond this insight, the findings underscore the multifaceted factors influencing PCPs’ prescribing of OADs, including patient preferences, drug formulary limitations, medication costs and EMR utilisation. To enhance clinical practice, interventions should focus on continuous education for PCPs, expanding drug formularies, addressing patients’ preferences, cost and access barriers through subsidies and promoting the adoption of EMRs with CDSS in both public and private sectors. Future research should evaluate the effectiveness of these interventions in improving prescribing practices and patient outcomes.
Footnotes
Appendix 1
Appendix 2
Appendix 3
Factors Influencing Primary Care Physicians’ Adjustment of Oral Anti-Diabetic Medications in Patients With Type 2 Diabetes Mellitus: A Qualitative Research Consolidated Criteria for Reporting Qualitative Studies (COREQ): 32-Item Checklist.
Acknowledgements
The authors are grateful to the FM ACP secretariat, SingHealth Polyclinics Bukit Merah staff, and the institute’s Department of Research for their assistance in implementing the study.
Abbreviation list
T2DM Type 2 diabetes mellitus
OADs Oral anti-diabetic drugs
DPP4 Dipeptidyl peptidase-4
SGLT2 Sodium-glucose cotransporter-2
PCPs primary care physicians
IDI in-depth interview
FGD focus group discussion
GDFM Graduate diploma in family medicine
MMed Masters of medicine in Family Medicine
FCFPS Fellowship programme
CME Continuing Medical Education
ACE Agency for Care Effectiveness
BMI body mass index
HbA1C glycosylated haemoglobin
EMR electronic medical records
CDSS clinical decision support system
GLP1-ra Glucagon-like peptide-1 agonists
Ethics Consideration
The study was approved by the SingHealth Centralized Institutional Review Board (CIRB 2021/2711). All participants provided written informed consent. The research complied with the International Conference on Harmonization Guidelines for Good Clinical Practice.
Author Contribution
NSYL and NCT conceptualised the study. NSYL conducted all the interviews. LGL and PCYC checked the data for accuracy. NSYL, ASM, NMFH, BSRL and ZL analysed the data. NSYL wrote the first draft. NSYL, ASM, SC and NCT revised the draft. All authors reviewed and approved the final draft before journal submission.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Family Medicine Academic Clinical Programme Collaborative Research Support Grant (FM ACP CRSG).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting this study’s findings are available from the corresponding author on reasonable request.