
Abstract
Objective:
The COVID-19 vaccine is vital for protecting pregnant women and their babies, yet many foreign-born women face unique challenges in vaccine uptake. This study explores COVID-19-related fears and vaccine acceptance among from the Northern Triangle countries—El Salvador, Guatemala, and Honduras in the United States (U.S.).
Methods:
This cross-sectional study aimed to identify factors influencing COVID-19 vaccination among foreign-born pregnant women from Central America, specifically El Salvador, Guatemala, and Honduras, living in the U.S.
Results:
The study included 93 women (mean gestation: 23.3 weeks), most of whom had lived in the U.S. for at least 10 years and had low acculturation. Over two-thirds (66.7%) were fully vaccinated. Key factors driving vaccine acceptance included healthcare access, community health initiatives, and trusted provider recommendations. Cultural values emphasizing family protection and a heightened sense of vulnerability to COVID-19 also contributed to higher vaccination rates. However, 33.3% expressed hesitancy, particularly due to distrust in government, fear of needles, and concerns about the vaccine’s rapid development, with Guatemalan participants showing the highest hesitancy.
Conclusions:
The findings underscore the critical role of healthcare providers in vaccination decisions. Tailored communication strategies that address cultural and emotional factors are essential for improving vaccine uptake, particularly within immigrant communities.
Introduction
The COVID-19 pandemic led to the rapid development of vaccines such as Moderna (mRNA-1237) and Pfizer (BNT162b2), which sparked debates on vaccine uptake.1,2 These discussions were influenced by factors like prior experiences, misinformation, beliefs about side effects, political ideology, and perceptions of COVID-19 as a low-risk disease.1,2
Pregnant women, a vulnerable group who were excluded from clinical trials, expressed heightened concerns about the safety of the vaccine during pregnancy. 2 Pregnancy-related physiological changes, such as shifts in cardiovascular and respiratory systems, increase susceptibility to infections like COVID-19.3,4 Pregnant women contracting COVID-19 are at significantly higher risk of severe illness, including mortality, ICU admissions, and preterm birth.2,4 While COVID-19 vaccines have proven effective in the general population, healthcare providers (HCPs) were initially hesitant to recommend vaccination for pregnant patients due to limited data.5,6 Leading organizations in the United States (U.S.), such as the Centers for Disease Control and Prevention (CDC) and the American College of Obstetricians and Gynecologists (ACOG), now recommend vaccination when the benefits outweigh the risks.7,8 Despite these recommendations, pregnant women have shown lower vaccination rates, with fewer than 45% expressing intent to vaccinate due to concerns about fetal safety and vaccine side effects.8 -10
The challenges of vaccine uptake are further compounded for immigrants, who often face significant health disparities, including limited access to healthcare, language barriers, and cultural differences. The Central American population in the U.S., particularly from El Salvador, Guatemala, and Honduras, is one of the largest and fastest-growing immigrant groups. 11 Many of these individuals experience lower socioeconomic status, limited health insurance, and higher rates of untreated chronic conditions, all of which hinder healthcare access and vaccine uptake. For pregnant women from Central America in the U.S., additional barriers such as misinformation and distrust in healthcare further contribute to vaccine hesitancy, placing them at greater risk for adverse health outcomes from COVID-19. 12
Although data on Central Americans in the U.S. is limited, studies on the broader Hispanic population highlight similar disparities in vaccine uptake. For example, a study of racial/ethnic disparities across 27 U.S. cities found that Hispanics had COVID-19 incidence rates 2.2 to 6.7 times higher than non-Hispanic Whites. 13 Similarly, vaccination coverage among Hispanics was lower than that of non-Hispanic Whites. 14 Among pregnant women, only 11.9% of Hispanic women received at least one COVID-19 vaccine dose during pregnancy, compared to 24.7% of non-Hispanic Asian women and 19.7% of non-Hispanic White women. 15
Given the elevated risks and lower vaccination rates among Hispanic pregnant women in the U.S., along with the lack of specific data on pregnant Central American immigrants, this study aims to explore COVID-19-related fears and vaccine uptake among pregnant women from the Northern Triangle countries of El Salvador, Guatemala, and Honduras residing in the U.S.
Materials and Methods
Study Design
Data from the present study were collected as part of an exploratory cross-sectional study designed to assess beliefs, experiences, and sources of information regarding gestational weight gain (GWG), diet, exercise, and oral health during pregnancy among pregnant Central American immigrant women from the Northern Triangle countries–El Salvador, Guatemala and Honduras. 16 Initially, the study focused solely on health behaviors and information sources during pregnancy. However, following the onset of the COVID-19 pandemic in March 2020, the research team decided to include questions related to the pandemic and COVID-19 vaccination.
Eligibility, Recruitment, and Data Collection
Women were eligible if they: (a) self-identified as Salvadoran, Guatemalan, or Honduran; (b) were pregnant with a single birth; (c) were at least 14 weeks gestation; (d) were 18 or older; (e) lived in Massachusetts communities with significant Central American populations; (f) spoke Spanish or English; and (g) provided informed consent.
Participants were recruited using methods that had been successfully employed in previous community-based studies involving immigrant Central American populations in Massachusetts, such as flyers at local businesses and churches, announcements, and network sampling.17,18 Research staff, including Central American immigrants, utilized community networks and social media, particularly Facebook, for recruitment. Participants were primarily recruited from towns in the Greater Boston area with large Central American populations, such as Revere, East Boston, Chelsea, and Somerville. Interested individuals were screened in-person or by phone. After confirming eligibility, bilingual interviewers explained the informed consent form, and participants completed a brief survey consisting of 72 items. 16
Survey Measures
The survey, adapted from previous research, included questions on health practices (eg, gestational weight gain, diet, physical activity, oral health), sociodemographic, acculturation, and two scales addressing COVID-19 fear and vaccination hesitancy.16,19 -22 The focus was on participants’ fears about COVID-19, vaccine uptake and hesitancy, and information sources.
COVID-19 Fear Scale for the Perinatal Period
We used nine items from the “Fear of COVID-19” scale, focusing on personal safety, pregnancy impacts, and transmission to the baby. 19 The scale, validated in Spanish, uses a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree).20,21
Vaccination Concerns and Reasons for Hesitancy
Eighteen questions adapted from the CDC survey addressed concerns about the vaccine, including side effects, distrust in government and pharmaceutical companies, and rapid development. 22 Participants selected the main reason for vaccine hesitancy from multiple options.
Sociodemographic, Acculturation, and Healthcare Access
The survey collected data on age, marital status, country of birth, U.S. residency, language, education, household income, pre-pregnancy weight status, and healthcare access (eg, regular provider, insurance, WIC). These questions were adapted from previous studies with Central American immigrants.17,18 Acculturation was assessed using the Short Acculturation Scale for Hispanics (SASH), a validated 12-item scale with high reliability (Cronbach’s α: .72–.92).23,24 Scores were dichotomized at 2.99 to classify participants as high or low acculturation. 23
The survey was pilot tested with three pregnant women, taking an average of 15 minutes to complete. Participants received a $25 gift card.
Ethical Considerations
The study adhered to the ethical principles outlined in the Helsinki Declaration and received ethical approval from the Institutional Review Board at the University of Massachusetts Boston (IRB: #2915 2021102). Participants were informed about the study both verbally and in writing, and their participation was voluntary, with the option of withdrawing at any time without consequence.
Data Analysis
Descriptive statistics were calculated for all variables, with means and standard deviations for continuous variables and frequencies and percentages for categorical variables. Responses to the “Fear of COVID-19” scale were dichotomized into two groups: “strongly agree/agree” versus “neutral/disagree/strongly disagree,” with frequencies reported for the “strongly agree/agree” category due to the small sample size. Chi-square (χ²) and Fisher’s exact tests were used, as appropriate, to assess differences in fear of COVID-19, vaccine uptake, and vaccine hesitancy by country of origin (El Salvador, Guatemala, and Honduras). All analyses were performed using SAS 9.4. 25
Results
As shown in Table 1, the study included 93 foreign-born pregnant women from El Salvador, Guatemala, or Honduras, with a mean gestation of 23.3 weeks (SD = 6.6). The majority (59.1%; n = 55) had lived in the U.S. for at least 10 years. Most participants were from Guatemala (46.2 %, n = 43), married or cohabiting with a partner (91.4%; n = 85), had at least a high school degree (83.9%; n = 78), and reported a household income of less than US $40,000 per year (91.2%; n = 62), which is below the federal poverty line. 26 Most participants had a SASH score of less than 2.99 (76.3%; n = 71), indicating low levels of acculturation.
Demographic, Socioeconomic, and Health-related Characteristics of the Study Sample (N = 93).
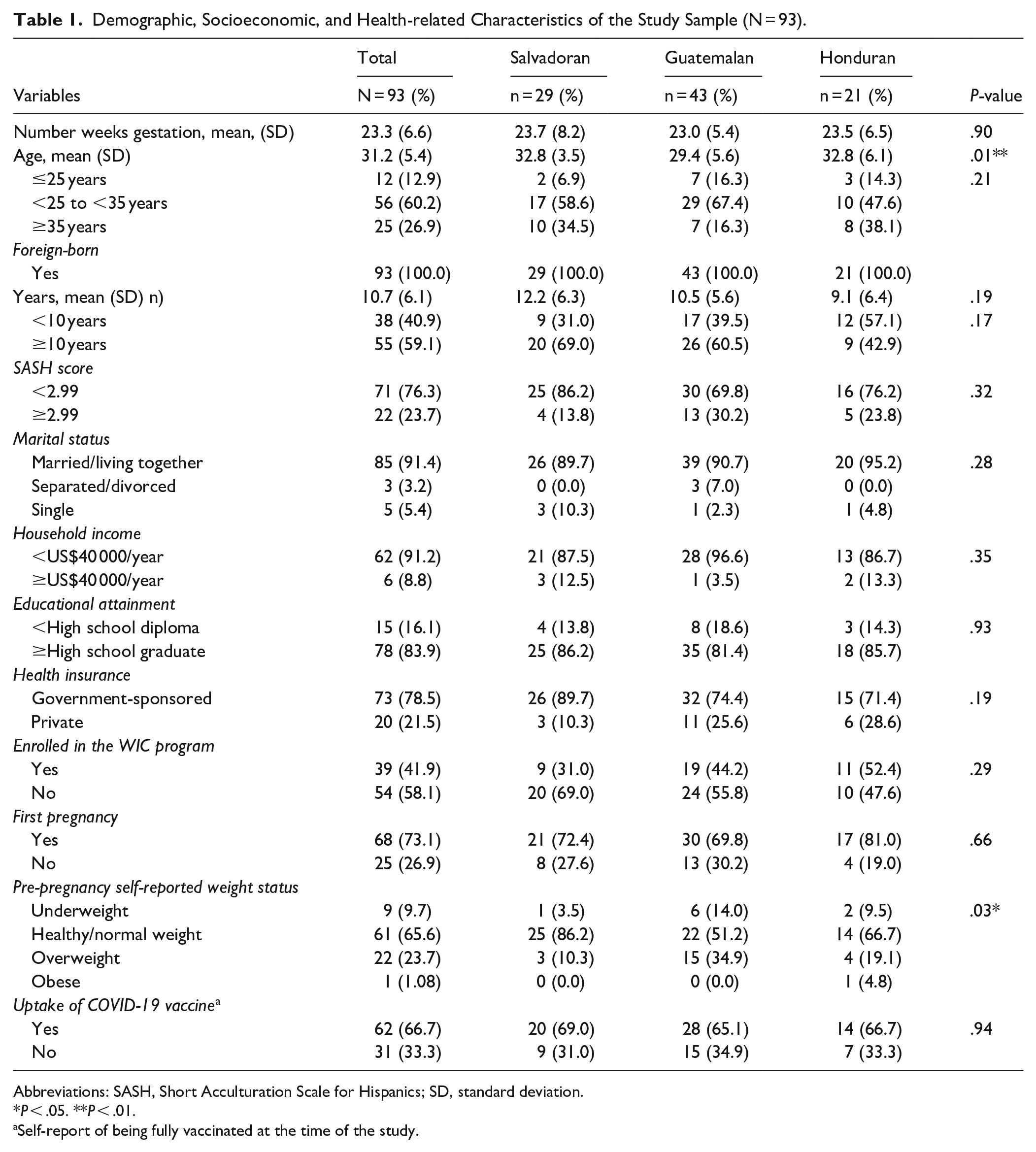
Abbreviations: SASH, Short Acculturation Scale for Hispanics; SD, standard deviation.
P < .05. **P < .01.
Self-report of being fully vaccinated at the time of the study.
All participants reported having health insurance, with the majority stating it was government-sponsored insurance (78.5%; n = 73), and 21.5% (n = 20) had private health insurance. Over half of the women (58.1%; n = 54) were enrolled in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). Over three-quarters of participants reported that this was their first pregnancy (73.1%; n = 68).
Finally, of the 93 participants, more than two-thirds (66.7%; n = 62) self-reported being fully vaccinated for COVID-19, with 69.0% (n = 20) of Salvadoran, 65.1% (n = 28) of Guatemalan, and 66.7% (n = 14) of Honduran pregnant women reporting full vaccination. The differences in vaccine uptake between the groups were not significant (P = .94).
Fear of COVID-19
Most women expressed concerns about being vaccinated against COVID-19, with their primary worries focused on the potential impact on their babies rather than themselves (Table 2). Over half of the women surveyed were afraid that their baby might become infected with COVID-19 (57%, n = 53) or that something negative could happen during pregnancy, childbirth, or the postpartum period because of COVID-19 (51.6%, n = 48). Nearly 42% (41.9%, n = 39) reported being very afraid of COVID-19. Other fears included feeling uncomfortable at the thought of COVID-19 (31.2%, n = 29) and being afraid of losing their own life due to the virus (40.9%, n = 38). There were no statistically significant differences in any of these concerns by country of origin, except for the level of fear regarding COVID-19 (P = .04).
Fear of COVID-19 (N = 93).

P-values are for χ² test (or Fisher’s Exact Test) assessing differences by country of origin.
P < .05. **P < .01.
COVID-19 Vaccine Uptake and Sources of Information
As shown in Table 3, over two-thirds of the participants (66.7%, n = 62) reported receiving the COVID-19 vaccine. When asked about their sources of information on the COVID-19 vaccine, the most common source reported was their healthcare providers (doctors or nurses); more than half of the participants (52.7%, n = 49) reported healthcare providers (doctors or nurses) as their primary source of information about the COVID-19 vaccine. The results of the analysis determined that there were significant differences in information sources by country of origin, with more Hondurans (66.7%, n = 14) and Salvadorans (65.5%, n = 19) relying on healthcare providers (doctors or nurses) for information compared to Guatemalans (37.2%, n = 16; P = .02). Other sources of information included social media (17.2%; n = 16), with WhatsApp and Facebook being the primary platforms cited, public health campaigns (11.8%; n = 11), and family members (10.8%; n = 10).
Uptake of COVID-19 Vaccine and Sources of Information About the COVID-19 Vaccine (N = 93).

P-values are for χ² test (or Fisher’s Exact Test) assessing differences by country of origin.
P < .05.
Self-report of being fully vaccinated at the time of the study.
Multiple response options allowed.
COVID-19 Vaccination Hesitancy
Table 4 outlines the primary reasons for hesitancy or refusal to get the COVID-19 vaccine among unvaccinated participants (33.3%; n = 31). The most cited reason was a lack of trust in the government (32.3%, n = 10). Other notable concerns included a dislike of needles (19.4%, n = 6) and the intention to wait and see if the vaccine is proven to be safe (16.1%, n = 5). Additionally, a few some women expressed concerns about vaccine safety and side effects (9.7%, n = 3) or believed that having had COVID-19 provided immunity, making vaccination unnecessary (9.7%, n = 3). One woman (3.2%) mentioned preferring to rely on masks and other precautions instead of getting vaccinated, while another (3.2%) cited religious reasons for their objection and hesitancy to get vaccinated.
Reasons for Not Getting Vaccinated Against COVID-19 Vaccine Among Unvaccinated Pregnant Women (n = 31).
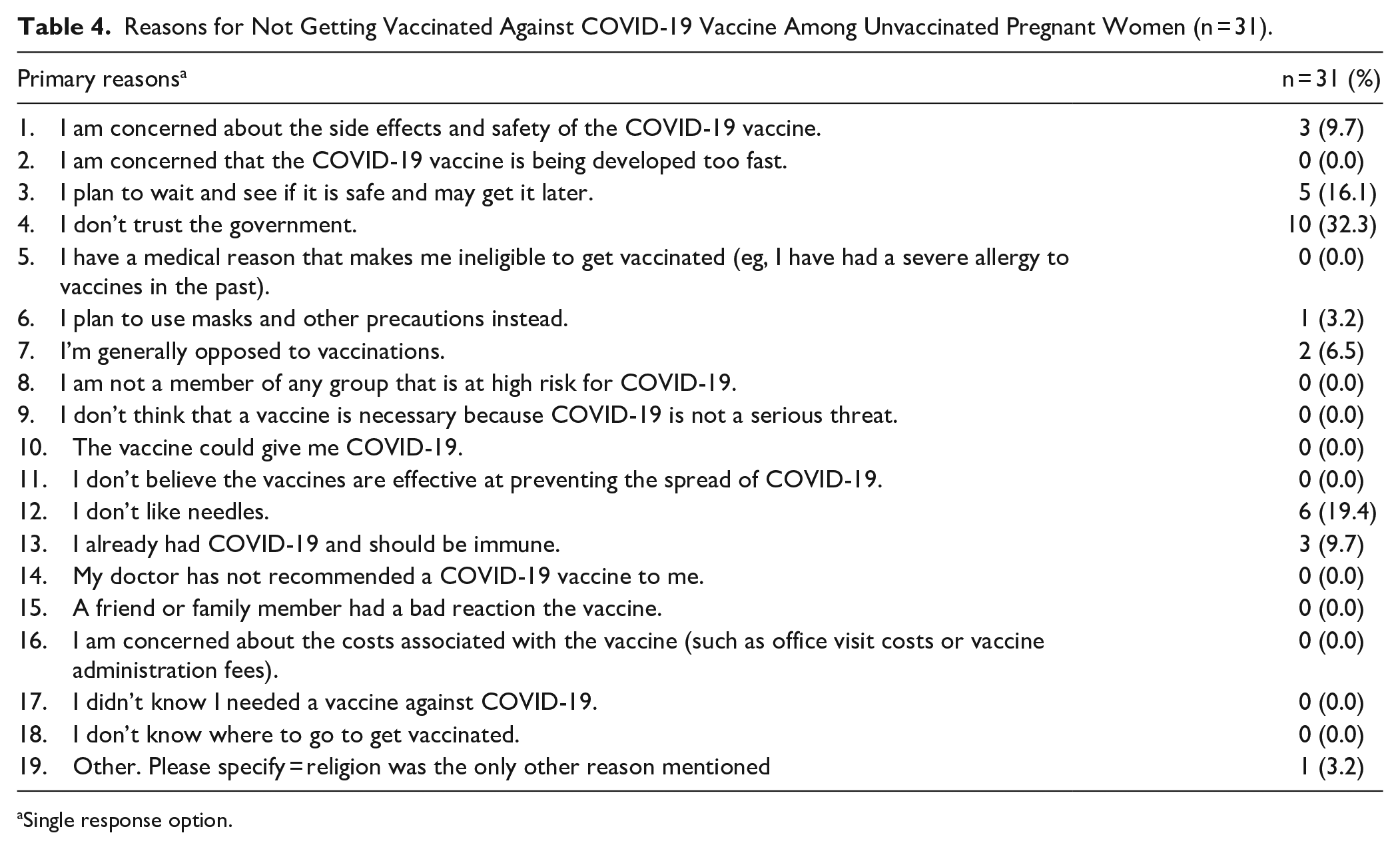
Single response option.
Discussion
This study explored COVID-19 fears, vaccination uptake, and hesitancy among pregnant Central American women from El Salvador, Guatemala, and Honduras in the U.S. Over two-thirds of participants (66.7%) reported being fully vaccinated, reflecting higher uptake compared to other multi-ethnic studies, where vaccination rates were lower (11.9%), 15 and 26.7%. 27 Future research could explore these differences.
Several factors contributed to the higher vaccination rate. All participants had health insurance and a regular healthcare provider, with community-based health initiatives, tailored messaging, and strong provider recommendations boosting vaccine acceptance. 28 Many participants viewed themselves and their families as vulnerable to COVID-19, and cultural values prioritizing family protection may have further increased vaccine uptake. 29
Fear of COVID-19 was a major concern, especially regarding pregnancy and infant health. Over half (57%) feared transmitting the virus to their babies or pregnancy complications, reflecting a desire to protect their children, consistent with prior research showing that pregnant women prioritize baby health over personal concerns. 30 Many also feared dying from COVID-19, underscoring the need for tailored mental health support for pregnant women. Public health messaging should emphasize vaccination’s benefits for both mother and child and address these fears directly.31,32
Despite high vaccination rates, one-third of participants expressed hesitancy, particularly among Guatemalan women, who had the lowest uptake. Reasons for hesitancy included distrust in government and fear of needles, consistent with literature on vaccine hesitancy in marginalized communities.33,34 Some also questioned the need for vaccination, believing natural immunity from prior infection was sufficient.35,36 These findings highlight the need for tailored communication strategies to address individual concerns and misinformation in Latino communities.28,34,36,37
Healthcare providers, especially doctors and nurses, were the primary sources of vaccine information, reinforcing their role in shaping health decisions.28,38,39 Targeted public health initiatives engaging HCPs are essential to address vaccine concerns and improve uptake, particularly among immigrant populations.
Healthcare providers, especially doctors and nurses, were the primary sources of vaccine information, reinforcing their role in shaping health decisions. 39 Targeted public health initiatives engaging HCPs are essential to address vaccine concerns and improve uptake, particularly among immigrant populations.36 -40 To effectively reach these communities, campaigns should leverage culturally relevant messaging through accessible mediums such as radio, television, social media, and visual materials. Previous successful initiatives, like “Juntos Sí Podemos” 39 and “De Ti Depende” 40 have demonstrated the power of simple, family-centered messages and visual storytelling, highlighting the importance of tailoring campaigns to language and cultural preferences to enhance health communication and outcomes.28 -30,41 -45
Ethnic differences in reliance on healthcare providers were noted, with Guatemalan women showing less trust in doctors and nurses than Salvadorans and Hondurans, suggesting that cultural factors may influence vaccine perceptions.44,46 These findings highlight the need for future research to explore how these ethnic differences in trust affect vaccine hesitancy and acceptance in these communities. Although no significant differences in acculturation were found, Guatemalans reported greater acculturation than Salvadorans and Hondurans, which may have contributed to vaccine hesitancy.1,31,34,36,41,45,47
Limitations
The study’s cross-sectional design limits the ability to establish causal relationships between vaccine uptake and information sources, as it provides only a snapshot of vaccine perceptions. 48 Self-reported data may introduce bias, with potential under- or over-reporting of vaccination status and fears due to social desirability. 49 Additionally, the small sample size poses constraints for data analysis, limiting the generalizability of the findings and the ability to draw broad conclusions. 50 While the sample may not fully represent the diverse experiences of pregnant Central American immigrant women in the U.S., this study is one of the first to focus specifically on Latina women from the Northern Triangle countries—El Salvador, Guatemala, and Honduras—providing valuable insights and laying the groundwork for future, larger studies to further explore these issues.
Conclusions
This study highlights the complex relationship between fear of COVID-19, vaccine uptake, hesitancy, and information sources among pregnant Central American immigrant women. Overcoming barriers to vaccine uptake requires culturally tailored interventions that build trust in healthcare systems and provide clear, accurate vaccine information. Public health strategies should focus on strengthening trust in healthcare providers and addressing emotional concerns about vaccination. While the pandemic is over, COVID-19 continues to impact communities, underscoring the ongoing relevance of this research. Vaccine hesitancy remains a challenge, especially with new variants. Future research should explore how the dynamics of vaccine hesitancy evolve over time, particularly through follow-up studies with participants, to assess whether concerns and hesitancy persist beyond initial intervention efforts. This could lead to a clearer identification of the long-term impact of culturally tailored interventions and the effectiveness of strategies aimed at improving trust in healthcare systems. Further, studies should continue to explore targeted approaches to enhance vaccine acceptance and address healthcare access barriers in diverse ethnic groups.
Footnotes
Acknowledgements
The authors sincerely thank the women who participated in this study for their valuable insights. We also appreciate the support from community members and organizations serving Central American immigrants in Massachusetts, which was essential to the success of this research.
Author Contributions
Conceptualization, A.C.L.; methodology, A.C.L., M.L.G., and Q.L.; software, Q.L.; formal analysis, Q.L.; investigation, N.R.-C., V.A.M., D.L., and A.C.L.; resources, A.C.L.; data curation, A.C.L., V.A.M., D.L, and N.R-C.; writing—original draft preparation, N.R.-C, M.L.G., and A.C.L.; writing—review and editing, V.A.M., D.L., N.R-C., Q.L, M.L.G., and A.C.L.; supervision, A.C.L.; project administration, V.A.M., D.L, and N.R.-C.; funding acquisition, A.C.L., D.L., V.A.M., and N. R-C. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by research trust funds from the University of Massachusetts Boston (Ana Cristina Lindsay). Nachalie Rodriguez-Cruz and Virginia A. Moreno received funding through the Beacon Student Success Fellowship, University of Massachusetts Boston. Doris Lucero was supported by a summer fellowship from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD/R25HD090723-02).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to privacy or ethical restrictions, the data that support the findings of this analysis are not publicly available; however, they are available upon request from the corresponding author.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the University of Massachusetts Boston (protocol #2915, approved on May 19, 2021).