
Abstract
Background:
Despite increased focus on social determinants of health, little is known about screening and intervention for asylum seekers, a highly marginalized group. We present the feasibility of a pilot social needs screening and resource navigation program at the Massachusetts General Hospital (MGH) Asylum Clinic in Boston, Massachusetts.
Methods:
Clinicians and staff referred patients who had a forensic evaluation in the clinic for screening. We screened across ten domains: (1) Housing and utilities, (2) Food security, (3) Access to healthcare, (4) Transportation, (5) Education/ Literacy, (6) Employment, (7) Childcare, (8) Disability/Disabling conditions, (9) Psychosocial well-being, and (10) Personal safety.
Results:
From April 2021 to June 2022, we evaluated 118 patients in the clinic. Twenty-eight (24%) completed screening. Their average age was 35.5 years (range = 18-67) and 50% were men. They came from 11 countries, with Uganda (25%), Cameroon (14%), El Salvador (14%), and Ecuador (14%) most represented. Most common needs were access to healthcare (86%), employment (46%), psychosocial wellbeing (43%), and education (43%). Applicants also typically screened positive for multiple domains (mean = 3.3, SD = 2.2, range = 1-8 domains).
Conclusion:
Our pilot social needs screening and resource navigation program in an academic asylum clinic demonstrates the model’s feasibility. Future studies should explore patient experiences and outcomes following referral.
Keywords
Background
Humanitarian crises around the world have forcibly displaced an increasing number of individuals worldwide. Among these are individuals applying for asylum, or asylum applicants who have fled their home countries to seek refuge due to persecution on the basis of internationally-protected grounds: race, religion, nationality, membership in a particular social group, and/or political opinion. Because their requests for protection have not yet been determined, their immigration status is precarious. According to the latest report published by the United Nations High Commissioner for Refugees (UNHCR), the global number of asylum applicants exceeded 8 million globally by June 2024. 1
In 2022, the United States (U.S.) recorded the largest number of pending asylum applications on record, with 1.6 million individuals awaiting the adjudication of their asylum immigration case. 2 As they wait, they must meet their immediate needs in the face of barriers related to immigration including language, discrimination, and ineligibility for public services like medical insurance or other public safety net and community programs. 3
Health-related social needs screening and intervention have been increasingly implemented as part of routine care across a variety of health settings including primary care clinics, emergency departments, and community health centers with trials showing positive impact on access to resources and health outcomes across diverse populations.4 -8 The approach to screening has varied from self-administered to facilitated, and at times provided unexpected results, for example, increased reporting of sensitive social needs with the use of electronic versus face-to-face screening. 6 A variety of screening tools have been developed and deployed including the Centers for Medicare & Medicaid Services Accountable Health Communities Model Screening Tool, 9 the National Association of Community Health Centers Protocol for Responding to and Assessing Patient Assets, Risks, and Experiences (PRAPARE), 10 the Health Leads Screening Toolkit, 11 and the American Academy of Family Physicians Social Needs Screening Tool. 12 Tools and methods of administration vary widely, 13 including personnel and training, location, the number and breadth of domains screened, integration with electronic health records, and protocols for referral and navigation around positive screens. The National Academy of Sciences has endorsed screening for unmet social needs, 14 while payers like Medicaid have incentivized it in states like Massachusetts. Despite the growing attention to social determinants of health as critical to health, there is a dearth of knowledge and implementation of screening and intervention among people applying for asylum in particular, who represent a highly marginalized group.
Forensic medical evaluations commonly involve 1-time evaluations of people seeking asylum or other forms of humanitarian relief who are referred by their attorney. Over the past 3 decades, medical providers including physicians, social workers, psychologists, advanced practice providers and other qualified experts who perform forensic medical evaluations have participated in various organizing models of care including the Physicians for Human Rights Asylum Network,15,16 clinics at academic medical centers,17 -19 and clinics specializing in refugee health. 20 Although the primary objective of asylum clinics is to provide medical expertise in the form of forensic medical evaluations, these clinics have the opportunity to assess and respond to asylum applicants’ social and health needs. We examined the workflow, demographics, and illustrative examples of health-related social needs screening and resource navigation in order to assess the feasibility of implementing a pilot program at the Massachusetts General Hospital (MGH) Asylum Clinic in Boston, Massachusetts, USA.
Methods
Context and Setting
The MGH Asylum Clinic is an academic asylum clinic engaging multidisciplinary volunteer clinicians to perform forensic medical evaluations in a stand-alone setting distinct from primary care and other clinical care delivery sites in the hospital. Asylum applicants seen in the clinic generally reside in the Greater Boston Area. Between 2017 and 2022, more than 200 clinicians evaluated 550 asylum applicants from 69 countries.
Screening Process and Tool
The MGH Asylum Clinic HRSN screening tool was informed by existing validated screening tools, including PRAPARE and the Health Leads’ Social Needs Screening Toolkit,10,11 and adapted based on expert opinion of Asylum Clinic leadership team to accommodate unique local needs and resource availability. The screening tool was designed to be verbally administered by a staff member in an in-person or telephonic setting. The final version contained 28 questions across ten domains: (1) Housing and utilities, (2) Food security, (3) Access to medical, mental, and oral healthcare, (4) Transportation, (5) Education and Literacy, (6) Employment, (7) Childcare, (8) Disability/Disabling conditions, (9) Psychosocial well-being, and (10) Personal safety (Figure 1).
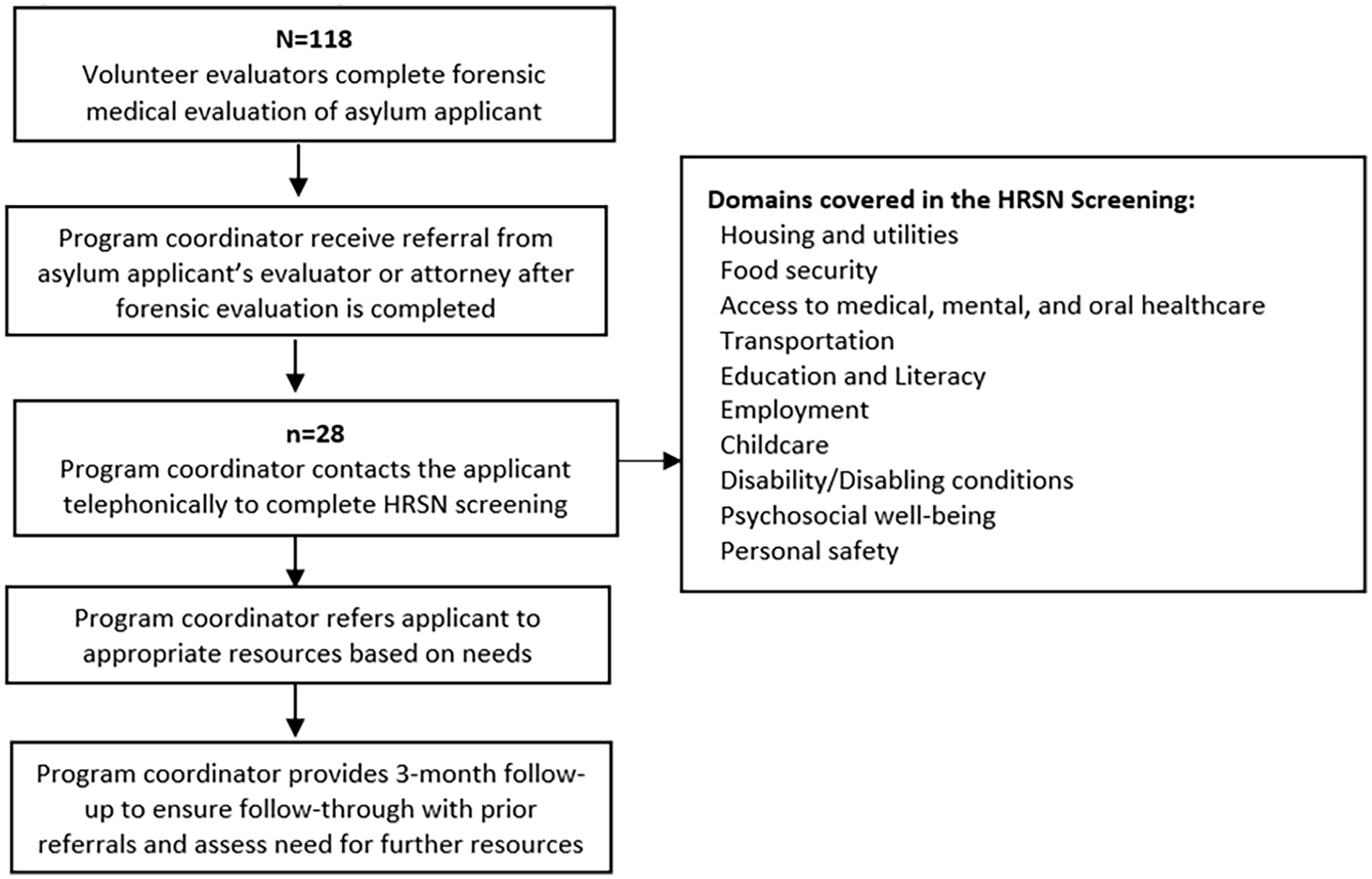
HRSN screening and resource navigation.
Implementation
We included in our pilot any adult who had a forensic medical evaluation completed in the MGH Asylum Clinic. Clinicians and staff identified and referred patients for screening. A program coordinator administered the screening.
The personnel in this role during the pilot phase of the intervention had at least a bachelor’s degree, experience working with immigrant or other marginalized communities, and training in trauma-informed care (TIC). One program coordinator was a bilingual Spanish-English speaker. Both used medically certified interpreters in our health system to conduct these screenings according to patient language preference. Screening was performed across 1 or more sessions to accommodate participants’ availability. If a patient screened positive, the program coordinator used shared decision-making to prioritize and meet needs identified by the asylum applicant. We created a protocol for the program coordinator to contact a clinician in the MGH Asylum Clinic leadership if any urgent or emergent mental health or other needs were identified during screening. Demographic data, screening results, and comments on resource navigation were recorded in REDCap. This information was not connected to an applicant’s electronic health records. We performed descriptive analyses. This study was determined exempt by the Massachusetts General Hospital Institutional Review Board.
Results
From April 2021 to June 2022, the MGH Asylum Clinic evaluated 118 patients. Twenty-eight (24%) completed screening. The median age was 35.5 years (range = 18-67) and 50% (n = 14) were male. There were 11 countries of origin, with Uganda (n = 7, 25%), Cameroon (n = 4, 14%), El Salvador (n = 4, 14%), and Ecuador (n = 4, 14%) most represented (Table 1).
Demographic Characteristics of Applicants Screened in Pilot Study (n = 28).

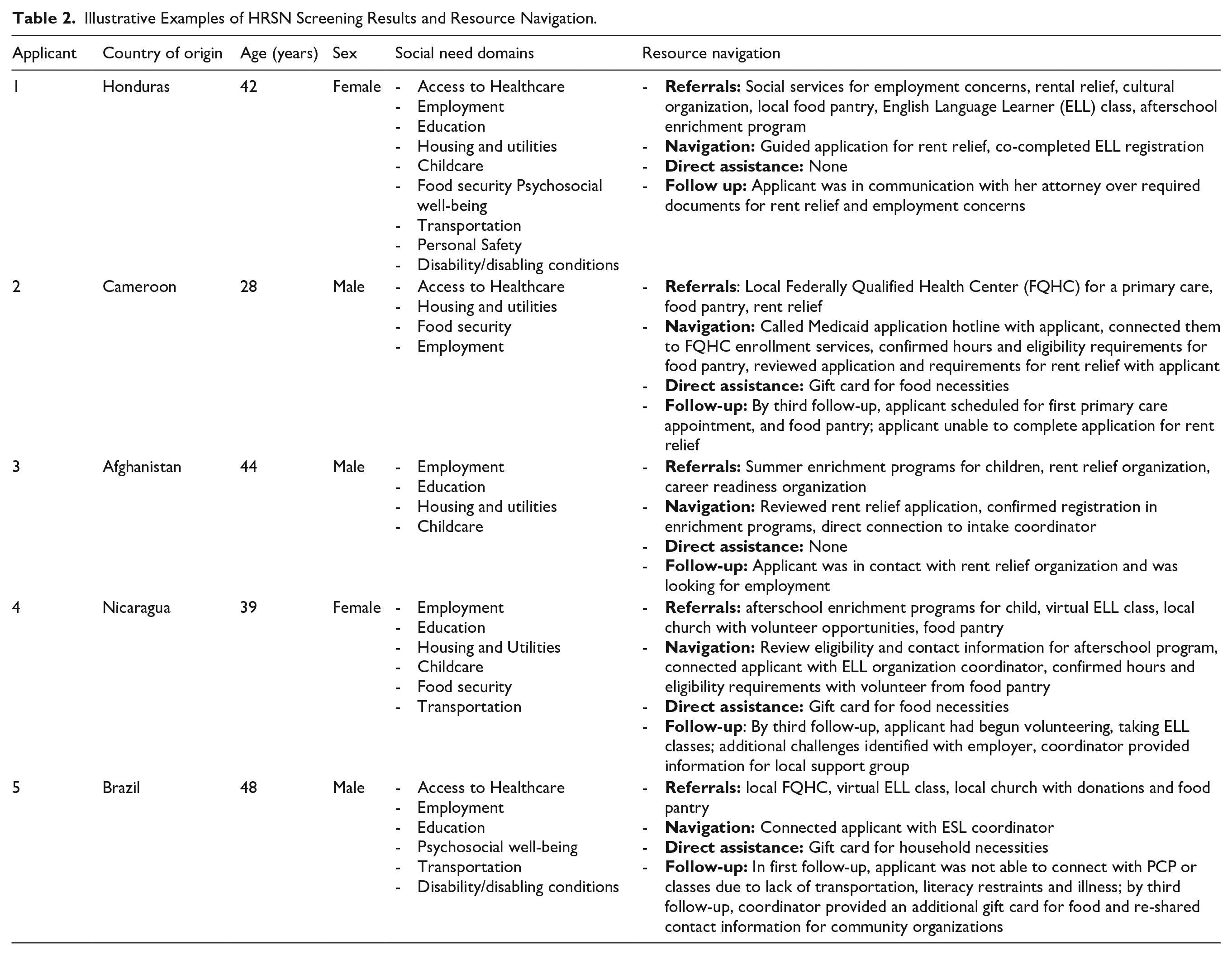
The 4 most common domains with positive screens were healthcare (n = 24, 86%), employment (n = 13, 46%), social engagement (n = 12, 43%), and education (n = 12, 43%; Figure 2), with illustrative cases of referrals and actions taken outlined in Table 2. On average, applicants screened positive for multiple domains (Mean = 3.3, SD = 2.2, range = 1-8). No urgent or emergent needs were identified.

Summary of domains identified in HRSN screening.
Illustrative Examples of HRSN Screening Results and Resource Navigation.
Discussion
In this study we present results from the implementation of a pilot HRSN screening and resource navigation program at the MGH Asylum Clinic with a goal of providing insights that may be transferrable to healthcare environments where programs are engaged with asylum applicants or other marginalized populations. The study demonstrates the feasibility and effective implementation of screening and navigation.
A program coordinator performed screening in approximately a quarter of asylum applicants seen in the clinic across a diverse group of participants to produce an individualized set of resources followed by active resource navigation. The 4 most common HRSN domains identified were healthcare, employment, social engagement, and education, however, we also found that applicants had broad needs, with all of those screened reporting needs across at least 1 domain. Barriers documented by the program coordinator included individual factors like competing priorities, health literacy, and mistrust in the healthcare system and local environment factors such as long wait lists for primary care, high cost of living, inadequate access to safe/affordable housing, shortages of language concordant mental health services, and eligibility restrictions for safety net services, consistent with prior literature.3,21
Participants were provided with referrals to a broad range of resources and received resource navigation including accompanied registration, review of requirements and eligibility, and frequent follow-up. Our study highlights the importance of navigation to overcome barriers to access for marginalized populations. For example, community resources often had cumbersome applications that took significant time for applicants, introducing a larger issue about administrative burden as a mechanism of inequity in policy implementation. 22 In this way, our resource navigation reduced the “time tax” that is disproportionately imposed on marginalized communities by assisting with this administrative burden. Additional barriers to resource access included geography and language. Resource availability was lower outside of the major metropolitan area, and existing application materials or resources were often available in English and Spanish only, highlighting the need to expand language access.
Finally, coordination of telephone calls for screening and resource navigation was challenging due to factors related to health-related social needs, including competing time constraints of work and childcare, and difficult finding functioning contact numbers or emergency contacts for applicants. We utilized contact with attorneys representing the applicants in their immigration case to set-up appointments and follow-up with applicants. Since all asylum applicants in our sample had legal representation, we are likely under-representing the burden of this barrier that may exist in a general population of asylum applicants.
Overall, our findings align with the organizing framework on the barriers to resource navigation employed by Sandu et al 23 including approachability, acceptability, availability, accommodation, affordability, and appropriateness. The relationship of health-related social needs and barriers to resource access to local, state, and federal contexts underscores the importance of addressing the upstream social, structural, and policy environments alongside individual-level interventions. 24 For example, applicants voiced safety concerns around crowded housing conditions with people outside their family units, especially women with children and those identifying as LGBTQ+. While addressing the individual’s needs may address resources for temporary, alternative housing options, a structural approach would involve advocating for more affordable housing options for all across the state. As another example, advocating for work authorization earlier in the course of the asylum process would facilitate employment opportunities and mitigate other social needs. Altogether, efforts like health-related social need screening and resource navigation programs must be accompanied by cross-sector and multidisciplinary efforts to truly address social and structural determinants of health. 25 This ultimately translates to increasing social service spending in the U.S., which has been showed to be associated with improved population health. 26
Our pilot also highlights the importance of training staff engaged in screening and resource navigation. This includes education in trauma-informed care, as there were universal and diverse experiences of trauma among the population of asylum applicants. Deficits identified through the screening, like social isolation and experiences of unsafe housing or employment exploitation, are intimately related to individuals’ experiences of trauma. A sensitive, trauma-informed approach was essential to developing the trust and rapport that were prerequisite for effective screening and navigation. Additionally, protocols and back-up support for incidents of safety concerns and mental emergencies are essential as staff may elicit safety concerns that require structured escalation.
Program staff also raised challenges of boundary-setting and vicarious or secondary trauma. For example, applicants sought long-term services more in-line with the role of a social worker or case manager and would reach out frequently to the program coordinators for social connection. Several applicants distrusted the broader healthcare system and sought a therapeutic connection with the program coordinators because they had developed a trusting relationship. Moving forward, we are tracking the number of contacts as a process metric to better understand how frequently and in what ways these highly trauma-exposed applicants interact with the program coordinators. Further, there is currently no standard qualification or training curriculum designed for this role. With more widespread development and implementation of screening programs specifically for asylum applicants and refugees, ongoing education and training programs need to be considered, including how to promote resilience in the role. Further, one can imagine that such screening, if done poorly, could lead to frustration for patients whose perceptions of health care systems could be further eroded. Therefore, in addition to systemizing a supervisory and training protocol, future efforts must be multi-level, including bolstering community resources to connect asylum applicants to community organizations, as well as increasing trust or trustworthiness of healthcare institutions broadly so that individual, compassionate staff are not overburdened.
Following the demonstrated feasibility and overall effective implementation of the pilot program along with new institutional funding, the clinic has been able to expand to provide universal screening to all applicants evaluated in the clinic. Our initial program coordinator was part-time, but with additional funding, we were able to expand the role to full-time and reassign administrative tasks to another staff member. These changes enabled us to scale up to universal screening.
Limitations and Opportunities for Future Research
There are several important limitations to our study. First, our pilot relied on discretion of clinicians refer applicants for screening, so those screened may not have been representative of the general clinic population. Referrals were also limited by factors such as providers’ or attorneys’ awareness of our screening initiative, and the availability of the program coordinator. Second, we did not screen children directly, necessitating further work to investigate and address the unique needs of child asylum applicants including unaccompanied minors. Third, although we did not encounter any challenges with our screening tool, future work could consider whether existing screening tools should be adapted or expanded. For example, our screening used a deficit-based model to identify needs in health-related social domains. Future work could include identifying individual and community strengths and assets. Additionally, prior studies have highlighted gendered experiences among refugees, such as women facing shifting and expanding roles that may require additional support. Other factors, like unequal access to community resources such as green spaces, could also influence community integration and mental health recovery, and could be captured in future assessments. Importantly, the time burden of completing screening instruments will need to be balanced against the need for more comprehensive information. Fourth, we did not evaluate the impact of screening and navigation on health outcomes. This is an important next step, particularly because several studies have raised doubt about whether such screening and referral programs actually improve health.6,27
Conclusion
The implementation of a pilot program for HRSN screening and resource navigation in an academic asylum clinic demonstrates the feasibility of the model. It also highlights the importance of navigation to overcome barriers to resource access and the need to for training and support for staff conducting screening and navigation. This study fills gaps in the existing literature on the role of HRSN screening and resource navigation to address underlying social risks and their adverse impacts on the health and well-being of asylum applicants. Given that individual deficits occur in the context of barriers at local, state, and national levels, individual-level screening and navigation must be accompanied by broader interventions to address social and structural determinants of health.
Footnotes
Ethical Considerations
The Massachusetts General Hospital Institutional Review Board deemed this study to be exempt.
Consent to Participate
All participants provided verbal consent to participate in this pilot program.
Consent for Publication
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data available within the article. Additional data can be made available from authors Drs. Matthew Gartland or Altaf Saadi upon reasonable request.